
Abstract
Objective:
Pulmonary rehabilitation (PR) has been considered to be an effective treatment method for various respiratory diseases. However, the effects of exercise-based PR on patients with severe/very severe chronic obstructive pulmonary disease (COPD) are unclear. This review aimed to investigate the effects of exercise-based PR on patients with severe/very severe COPD.
Methods:
PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov databases were searched from inception to December 23, 2022, without language restrictions. Randomized controlled trials (RCTs) investigating the effects of exercise-based PR on patients with severe/very severe COPD were included. Study selection, data extraction, and risk of bias assessment were conducted independently. RevMan software (version 5.3) was used for meta-analysis. The quality of evidence was rated using the Grading of Recommendations Assessment, Development and Evaluation system.
Results:
Six studies (263 patients) were identified. Compared with the control group, the 6-min walking distance [MD = 52.91, 95% CI (3.80, 102.03)], the St. George’s Respiratory Questionnaire total scores [MD = −7.70, 95% CI (−14.32, −1.08)] and the Borg scale scores [MD = −0.68, 95% CI (−1.28, −0.08)] in the experimental group improved, respectively. The St. George’s Respiratory Questionnaire and Borg scale scores were rated as ‘moderate quality’ and ‘low quality’, respectively, and the 6-min walking distance was rated as ‘very low quality’.
Conclusions:
Exercise-based PR may improve the exercise capacity, quality of life and dyspnea of patients with severe/very severe COPD, which can be regarded as an adjuvant treatment. High quality and large sample RCTs are needed.
Registration:
This systematic review and meta-analysis protocol was prospectively registered with PROSPERO (No. CRD42022294085).
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable disease characterized by persistent respiratory symptoms and airflow limitation, which seriously endangers public health. 1 With the increase in the number of smokers, the continuous accumulation of environmental pollution and social aging, the prevalence, morbidity, and mortality rate of COPD are rising. 2 The World Health Organization predicts that COPD will become the third leading cause of death and the fifth largest economic burden in the world by 2030. 3 Chronic and progressive dyspnea is the most characteristic symptom of COPD, which can further lead to the decline of exercise capacity and quality of life, and bring a heavy disease burden, especially for patients with severe and very severe COPD. 4 In addition to pharmacological therapy, nonpharmacological therapy can be used as a supplement according to the management guidelines of stable COPD. Pulmonary rehabilitation is an important part of nonpharmacological therapy, which has a positive impact on improving exercise capacity, health status, and dyspnea of patients in stable stage. 5
Pulmonary rehabilitation (PR) is a comprehensive intervention aimed at improving the physical and mental status of patients with chronic respiratory diseases, including but not limited to exercise training, education and behavior change. 6 As the core component of PR, exercise training includes endurance training, interval training, resistance/strength training, and upper limb training, among others. 6 Multiple evidences show that exercise-based PR can better improve the exercise capacity, quality of life, and dyspnea of COPD patients compared with non exercise items.7–10 There are differences in disease changes according to disease severity. Most of the existing literature reviews did not distinguish COPD patients with different severity, and the evidences of exercise-based PR were mainly concentrated in moderate-to-severe COPD patients. 1 Whether patients with severe/very severe COPD can tolerate and benefit from PR training, and the safe and effective intensity of exercise training has not been determined. Therefore, this study aimed to evaluate the effects of exercise-based PR on exercise capacity, quality of life and dyspnea in patients with severe/very severe COPD.
Materials and methods
The method of this review strictly followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 11 The protocol for this review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) and the registry number is CRD42022294085.
Search strategy
Search databases including PubMed, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov from database creation to December 23, 2022, with no language restrictions. Elaborated search strategies were developed associated with ‘chronic obstruction pulmonary disease’ and ‘pulmonary rehabilitation’ (including exercise training, exercise therapy, endurance training, resistance training, muscle stretching exercise, upper limb training, and interval training) and ‘randomized controlled trials (RCTs)’. The references and related systematic reviews were also reviewed.
Research selection
First, by browsing the title and abstract, duplicate and inappropriate studies were discarded. Screening was then performed based on inclusion and exclusion criteria. Inclusion criteria included all of the following: (a) patients with severe and very severe COPD according to the severity of airflow limitation classified by post-bronchodilator FEV1; (b) interventions involved any exercise-based PR compared with other treatments (drug treatment, routine nursing, patient education, etc.), such as endurance training, resistance training, exercise training, upper limb training, flexibility training and interval training; (c) at least one of the results recorded exercise capacity, quality of life or dyspnea; (d) the study was designed as a RCT. Because the exercise plan could not be blind and had great heterogeneity, the blind method of this study was not limited. Exclusion criteria were (a) participants with other complications of respiratory discomfort in addition to COPD; (b) the type of literature was a study protocol; and (c) insufficient original materials or unable to obtain full text, such as meeting summaries or supplementary information. The detailed retrieval strategies and steps are presented in the Supplementary Materials Appendix 1.
Data extraction
Two investigators conducted the study and any disagreements were resolved in consultation with the third investigator. Extracted information comprised author information, region, design scheme, sample size, participant status, intervention measures, course, and outcomes. The extracted outcomes were as follows: exercise capacity measured by 6-min walking distance (6MWD), quality of life measured by St. George’s Respiratory Questionnaire (SGRQ) sores, and dyspnea measured by Borg scale scores.
Risk of bias evaluation
Two researchers assessed the risk of bias using the Cochrane risk of bias tool, 12 and the third researcher acted as an arbitrator for the inconsistency. The aspects of evaluation included random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Each study was divided into low risk of bias, unclear risk of bias or high risk of bias.
Data analysis
RevMan software (version 5.3) was used for meta-analysis. Continuous data were estimated by mean difference (MD) and 95% confidence interval (CIs). In the process of heterogeneity test, P ⩽ 0.10 and I2 ⩾ 50% were regarded as the basis for statistical significance evaluation. If p > 0.10 and I2 < 50%, it could be judged that the heterogeneity was relatively low, and the fixed effect model was used for research. If P ⩽ 0.10 and I2 ⩾ 50%, it was judged that the heterogeneity was high, the random effect model was adopted, and the analysis content is shown in the forest map.12,13
Evidence quality evaluation
Using GRADEpro (gradeprogdt, http://www.gradepro.org/) evaluated the evidence quality of the main results. 14 The factors that reduce the quality of evidence (risk of bias, inconsistency, indirectness, imprecision, and publication bias) were rated, and the quality of evidence was evaluated as ‘very low’, ‘low’, ‘moderate’, or ‘high’.
Results
Literature selection
A total of 6442 articles were identified through the search, of which 1928 were duplicates. After reading the title and abstract, 31 articles were considered eligible for further evaluation, of which 25 were excluded after careful reading of the full text. Finally, six studies9,15–19 (263 participants) were included. The research screening process is shown in Figure 1. A list of excluded studies is provided in the Supplementary Materials Appendix 2.

Study flow diagram for this review.
Data extraction and risk of bias evaluation
Due to the particularity of the intervention measures, it is difficult to implement blinding for patients. All studies9,15–19 described specific random methods. Four studies16–19 were blinded to investigators and outcome statisticians. The sample sizes of the EG (experimental group) and the CG (control group) included in the study were 147 and 116, respectively, of which the maximum sample size was 55 and the minimum sample size was 4. The basic features of the included literatures are shown in Table 1, and the quality evaluation results of methodology are shown in Figure 2(a) and (b).
Basic characteristics of the included studies.

6MWD, 6-Min Walk Distance; BODE, body-mass index, airflow obstruction, dyspnea, and exercise capacity index; CCQ, Clinical Chronic Obstruction Pulmonary Disease Questionnaire; CG, control group; COPD, chronic obstructive pulmonary disease; CRQ, Chronic Respiratory Disease Questionnaire; EG, experimental group; HADS, Hospital Anxiety and Depression Scale; NA, not available; PR, pulmonary rehabilitation; RCT, randomized controlled trial; SF-36, the MOS 36-item short form health survey; SGRQ, St. George’s respiratory questionnaire; VO2, peak, peak oxygen uptake.
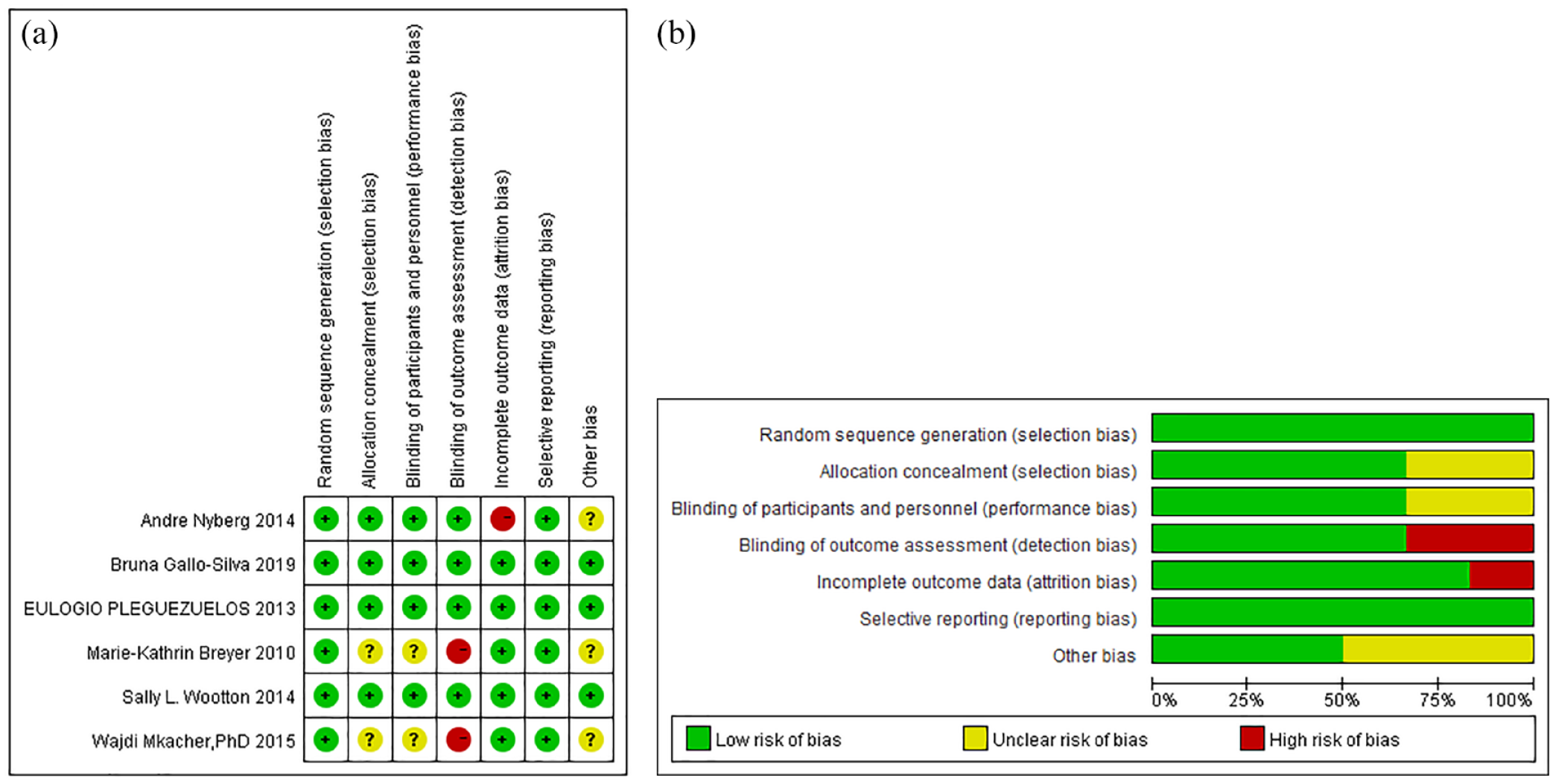
(a) Risk of bias summary. (b) Risk of bias graph.
Effects
6MWD
Six studies9,15–19 investigated 6MWD. Among them, five studies9,15–18 provided 6MWD numerical data, which were included in meta-analysis; after testing the heterogeneity, the random effect model was adopted (χ2 = 54.90, p < 0.00001, I2 = 93%). The results showed that the 6MWD of the EG was longer than that of the CG, and the difference was statistically significant [MD = 52.91, 95% CI (3.80, 102.03), Z = 2.11, p = 0.03] (Figure 3, Table 2). One study 19 was not included in the meta-analysis, which reported the average 6MWD of the two groups, 538 m in the EG and 486 m in the CG.
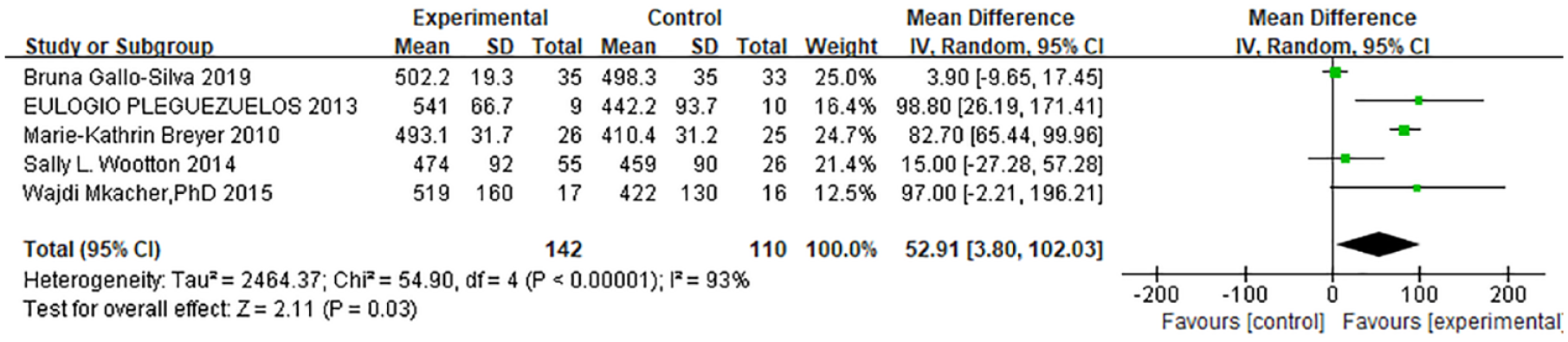
Forest plot of 6MWD.
Meta-analysis of exercise-based PR for COPD.
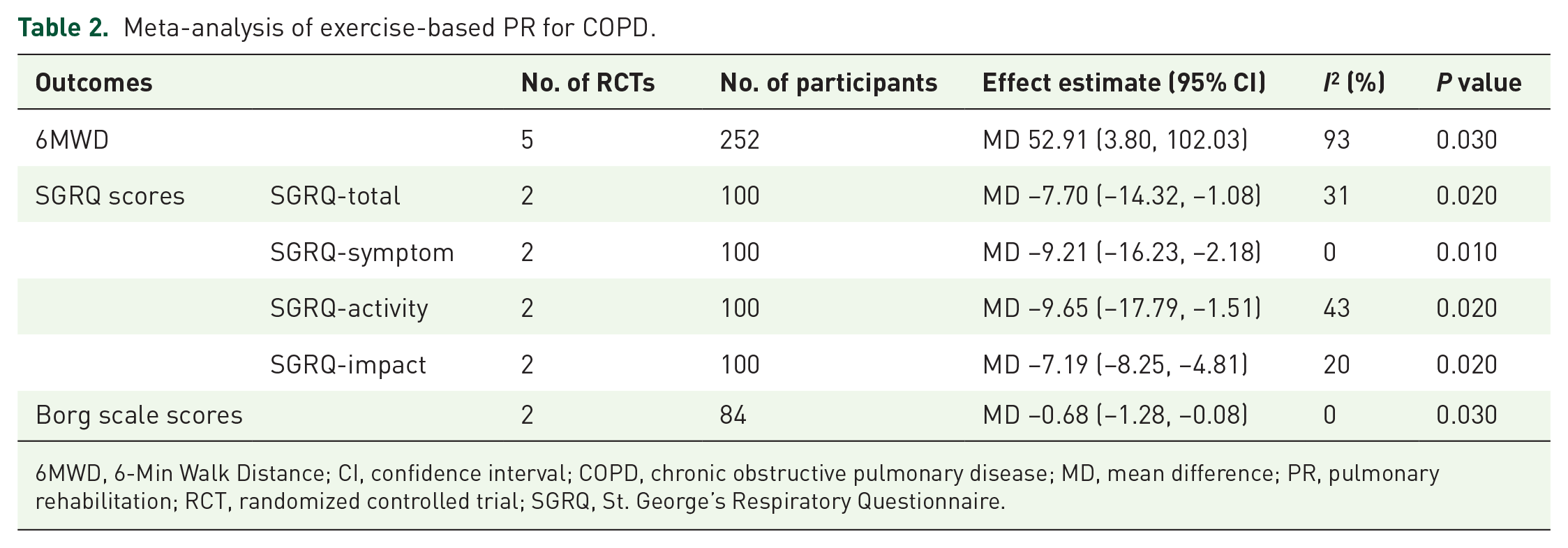
6MWD, 6-Min Walk Distance; CI, confidence interval; COPD, chronic obstructive pulmonary disease; MD, mean difference; PR, pulmonary rehabilitation; RCT, randomized controlled trial; SGRQ, St. George’s Respiratory Questionnaire.
SGRQ scores
Two studies16,18 provided numerical data for SGRQ scores and were included in meta-analysis (Figure 4, Table 2). Both studies provided scores of SGRQ domains. No heterogeneity was found in the total domain (χ2 = 1.44, p = 0.23; I2 = 31%), and a fixed effect model was accepted. The pooled results showed that the total domain scores of EG were lower than CG, and the difference was statistically significant [MD = −7.70, 95% CI (−14.32, −1.08), Z = 2.28, p = 0.02].

Forest plot of SGRQ scores.
Two studies provided SGRQ symptom domain scores and found no heterogeneity (χ2 = 0.00, p = 0.96; I2 = 0%), and a fixed effect model was adopted. The pooled results showed that the symptom domain scores of EG were lower than CG, and the difference was statistically significant [MD = −9.21, 95% CI (−16.23, −2.18), Z = 2.57, p = 0.01]. No heterogeneity was found in the activity domain (χ2 = 1.74, p = 0.19; I2 = 43%), and a fixed effect model was adopted. The pooled results showed that the activity domain scores of EG were lower than CG, and the difference was statistically significant [MD = −9.65, 95% CI (−17.79, −1.51), Z = 2.32, p = 0.02]. No heterogeneity was found in the impact domain (χ2 = 1.25, p = 0.26; I2 = 20%), and a fixed effect model was adopted. The pooled results showed that the impact domain scores of EG were lower than CG, and the difference was statistically significant [MD = −7.19, 95% CI (−8.25, −4.81), Z = 2.27, p = 0.02].
Borg scale scores
Two studies9,17 provided Borg scale scores and were included in meta-analysis; no heterogeneity was found (χ2 = 0.01, p = 0.91, I2 = 0%), using fixed effect model. The results showed that the EG scores were lower than CG, and the difference was statistically significant [MD = −0.68, 95% CI (−1.28, −0.08), Z = 2.23, p = 0.03] (Figure 5, Table 2).

Forest plot of Borg scale scores.
Evidence quality evaluation
6MWD, SGRQ and Borg scale score were rated as ‘very low quality’, ‘moderate quality’, and ‘low quality’, respectively, due to limited sample size, high heterogeneity, wide confidence interval, lack of blindness, and unclear concealment of distribution. The summary of grade evidence is shown in Table 3.
Quality of evidence for outcomes in patients with COPD.

6MWD, 6-Min Walk Distance; CI, confidence interval; CG, control group; COPD, chronic obstructive pulmonary disease; EG, experimental group; MD, mean difference; SGRQ, St. George’s Respiratory Questionnaire.
Lack of blinding and concealment of allocation are not clear.
High heterogeneity (I2 > 50%).
Limited sample size and wide confidence interval.
Discussion
As a more effective way of PR intervention, exercise training can improve the adaptability of patients and optimize the functions of other systems of the body through whole-body exercise training. It has attracted the attention of respiratory researchers all over the world and has been widely used in various chronic respiratory diseases including COPD.20–24 This systematic review and meta-analysis aimed to summarize the effects of exercise-based PR on patients with severe/very severe COPD, so as to produce proofs for clinicians and decision-makers. In this study, 6MWD was used to test exercise capacity, SGRQ and Borg scale scores were used to assess the quality of life and dyspnea in COPD patients, respectively. The reliability, feasibility, and sensitivity of these indicators have been unanimously recognized, and gradually become the important means to evaluate the treatment effects of COPD patients.25,26
Exercise capacity is considered as a highly sensitive index to evaluate the effect of PR treatment in COPD patients, and 6MWD is one of the indicators that can reflect exercise capacity recognized at home and abroad. 27 Borg scale scores can quickly and simply evaluate the severity of dyspnea in patients under exercise. 28 It is usually combined with 6MWD, which can truly reflect the patients’ cardiopulmonary endurance and ventilator energy level. In our review, 6MWD and Borg scale scores were used to evaluate the exercise capacity and dyspnea of patients. After exercise-based PR, the 6MWD and Borg scale scores of COPD patients were significantly higher than those of CG, suggesting that exercise-based PR can significantly improve their exercise capacity and dyspnea. The MD between the two groups of 6MWD was 52.91 m, exceeding the minimal clinically important difference (MCID) of 6MWD in COPD patients, which could indicate the potential of exercise-based PR in improving the exercise capacity of patients with severe and very severe COPD. 29
SGRQ scale is a standardized questionnaire that can comprehensively and accurately evaluate the quality of life and clinical symptoms of COPD patients, predict the risk of death, and has a good correlation with pulmonary function, 30 which is widely used in clinical practice.31,32 There are 50 items in the SGRQ questionnaire, which are divided into three dimensions, including respiratory symptoms, activity limitation, and disease impact. The three dimensions are weighted and averaged to obtain a final score of 100. Our meta-analysis showed that after exercise-based PR, the scores of SGRQ total domain, symptom domain, activity domain, and impact domain in patients with severe/very severe COPD were significantly lower than those in the conventional treatment group. Although there was no MCID available for each domain, each MD was more than four units (the MCID of the total SGRQ scores of COPD patients), 33 suggesting that exercise-based PR can significantly improve the symptoms, activity, and disease impact of COPD patients, thereby further improving the quality of life.
Among the six RCTs, three studies took the guided exercise training three times a week, and the program lasted for 8 weeks. No serious adverse reactions were reported in the included studies, and the implementation was feasible. We performed sensitivity analysis on the difference between baseline and end-point changes of each indicator, which showed that the study results were reliable (Supplementary Materials Appendix 3). We also reviewed the relevant systematic review and meta-analysis of exercise-based PR in COPD in recent years. The results showed that exercise-based PR significantly increased 6MWD of stable COPD patients and improved their health-related quality of life. Most of the literatures did not distinguish the severity of the disease, one of the literatures evaluated patients with very serious chronic obstructive pulmonary disease. 34 Because of the very severe patients with poor pulmonary function, severe dyspnea, repeated acute attacks, mostly combined with anxiety and depression, poor tolerance and compliance, and the amount of exercise should be gradual. Continuous high-intensity endurance training is beneficial to very severe but stable COPD patients. 34 In terms of emotional impact, a relevant study shows that exercise training has a significant effect on improving people’s negative emotions, such as anxiety and depression. 35 In this review, two studies9,19 investigated hospital anxiety and depression scale (HADS) scores. The numerical data of one study 9 showed that the HADS scores of EG were lower than CG, and there was a significant difference. One Study 19 reported the average HADS scores of both groups, in which EG was significantly lower than CG in anxiety and depression scores.
There were some limitations in our study. First, due to the different rehabilitation approaches and benefits of COPD patients with different severity, different rehabilitation training were required, and the sample size and literature quality needed to be further expanded and improved. Nevertheless, this is the only systematic review and meta-analysis to evaluate the effects of exercise-based PR on patients with severe/very severe COPD. Second, due to different interventions, it was difficult to measure the impact of a single exercise modality. Third, exercise programs could not be blinded, and the study might have potential bias. Fourth, some data were in original form, could not be included in quantitative analysis and be fully utilized.
Conclusions
Exercise-based PR may improve the exercise capacity, quality of life and dyspnea of patients with severe/very severe COPD, and can be used as an adjuvant treatment for COPD management. Continuous training exercise mode should be adopted for patients with very severe but stable COPD, which can improve their anxiety and depression to a certain extent. High-quality and large sample RCTs are required.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666231162250 – Supplemental material for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-tar-10.1177_17534666231162250 for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis by Wenqing He, Jiajia Wang, Zhenzhen Feng, Jiansheng Li and Yang Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666231162250 – Supplemental material for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-tar-10.1177_17534666231162250 for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis by Wenqing He, Jiajia Wang, Zhenzhen Feng, Jiansheng Li and Yang Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666231162250 – Supplemental material for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis
Supplemental material, sj-pdf-3-tar-10.1177_17534666231162250 for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis by Wenqing He, Jiajia Wang, Zhenzhen Feng, Jiansheng Li and Yang Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-4-tar-10.1177_17534666231162250 – Supplemental material for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis
Supplemental material, sj-pdf-4-tar-10.1177_17534666231162250 for Effects of exercise-based pulmonary rehabilitation on severe/very severe COPD: a systematic review and meta-analysis by Wenqing He, Jiajia Wang, Zhenzhen Feng, Jiansheng Li and Yang Xie in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.