
Abstract
Background:
Lower limb aerobic exercise is the core component of pulmonary rehabilitation for chronic obstructive pulmonary disease (COPD) patients. The optimal intensity and type (e.g., interval or continuous) of exercise training remains to be determined.
Objectives:
We aimed to evaluate the optimal intensities and types of lower limb aerobic exercise in patients with COPD.
Design:
Systematic review and network meta-analysis of randomized controlled trials.
Data sources and methods:
The PubMed, Web of Science, Embase, and the Cochrane Central Register of Controlled Trials were searched for relevant data. The interventions were classified according to their intensity and type as high-intensity interval training (HIIT), high-intensity continuous training (HICT), moderate-intensity continuous training (MICT), and low-intensity continuous training (LICT). We assessed exercise capacity using peak work rate (Wpeak) and the 6-min walking test (6-MWT). Lung function was evaluated by measuring peak minute ventilation (VE) and the percentage of predicted FEV1 (FEV1pred%). Dyspnea was assessed using the Modified Medical Research Council (mMRC) scale. Quality of life was measured with the Chronic Respiratory Questionnaire (CRQ).
Results:
Fifteen studies were identified (979 subjects). HIIT showed the greatest improvement in Wpeak, 6-MWT, VE, and mMRC compared to usual care (MD 18.48 (95% CI 12.35, 24.60), 67.73 (34.89, 100.57), 6.26 (2.81, 9.72), and −0.53 (−0.89, −0.17), respectively) and showed the improvement in CRQ (MD 10.80 (95% CI 1.65, 19.95)). MICT showed improvement in Wpeak and 6-MWT (MD 18.28 (95% CI 11.20, 25.22), 61.92 (28.34, 95.51)) similar to HICT (MD 16.08 (95% CI 8.19, 23.84), 64.64 (28.70, 100.57)) and showed the highest improvement in CRQ compared to usual care (MD 10.83 (95% CI 1.68, 19.98)). LICT significantly improved Wpeak compared to usual care (MD 13.47 (95% CI 4.77, 22.13)). The quality of evidence for outcomes varied from very low to moderate.
Conclusion:
HIIT and MICT might be optimal training approaches for patients with COPD. LICT exhibited limited clinical efficacy. While HICT was as effective as MICT, it caused more dyspnea.
Trial registration:
This systematic review and network meta-analysis was prospectively registered with PROSPERO (No. CRD 42024520134).
Plain language summary
Pulmonary rehabilitation, which often includes lower limb aerobic exercise, is essential for managing chronic obstructive pulmonary disease (COPD). However, the best intensity and type of exercise for these patients are not yet fully established. This study aimed to identify which exercise intensity and type are most effective for patients with COPD. To achieve this, we reviewed and analyzed data from multiple studies that compared different exercise programs: high-intensity interval training (HIIT), high-intensity continuous training (HICT), moderate-intensity continuous training (MICT), and low-intensity continuous training (LICT). We evaluated their effects on exercise capacity, lung function, breathlessness, and quality of life. Our analysis included 15 studies with 979 participants. The results showed that HIIT led to the most significant improvements in exercise capacity, lung function, and breathlessness, and it also enhanced quality of life. MICT also produced notable benefits, particularly in exercise capacity and quality of life, similar to HICT. LICT was effective in improving exercise capacity but to a lesser extent. Overall, the evidence suggests that HIIT and MICT may be the most effective exercise approaches for patients with COPD. However, the quality of the evidence varied, so further research is needed to confirm these findings.

Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a pulmonary disease with chronic respiratory symptoms caused by airway and/or alveoli abnormalities, leading to persistent airflow obstruction. 1 As the disease deteriorates, it can lead to complications in various organ systems, such as the cardiovascular and musculoskeletal systems, significantly impacting the patient’s overall quality of life.2,3 By 2030, COPD will be the third leading cause of death globally, resulting in significant clinical, economic, and social burdens. 4
The global initiative for COPD guidelines proposed that lower limb aerobic exercise, a cost-effective treatment, could alleviate the clinical symptoms, reduce the risk of mortality and cardiovascular burden among patients with COPD, and prolong their life expectancy.1,5 However, there is a wide variety of aerobic exercises with significant variations in their content. Exercise prescribing to maximize patient benefit remains unresolved.6,7
The intensity and type (e.g., interval or continuous) of the exercises play a pivotal role in shaping the exercise prescription.8 –10 Low-intensity training often produces limited physiological outcomes, whereas high-intensity training invariably results in significant dyspnea, especially in individuals with pre-existing lung conditions.8,11 Additionally, interval training has been reported to enhance exercise performance more effectively than constant-load training in healthy individuals, 12 as it increases exercise volume and helps to avoid fatigue and breathlessness. 13 However, it remains unclear whether similar effects are observed in patients with COPD. 14 Some studies have primarily focused on training methods, neglecting the quantitative aspect of intervention intensity, leading to a failure to acknowledge the heterogeneity in different intensity levels.15,16
This meta-analysis examines the impact of exercise intensity and type on exercise capacity, lung function, dyspnea, and quality of life in patients with COPD. The comprehensive analysis of quantifying the intensity of lower limb aerobic exercise will provide more precise guidance for individuals with COPD. 17
Methods
This systematic review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for Network Meta-Analyses (PRISMA-NMA) statement and checklist. 18 The search has been registered in PROSPERO (CRD 42024520134).
Search strategy
Multiple databases, including PubMed, Cochrane Library, Web of Science, and Embase, were searched from their inception to January 25, 2024. The main search strategies were as follows: (“chronic obstructive lung disease” OR “chronic obstructive pulmonary diseases” OR “coad”:ab, ti OR “copd”) AND (“exercise” OR “train” OR “training” OR “lower limb” OR “treadmill” OR “ergometer”) AND (“intensity” OR “endurance” OR “interval” OR “intermittent” OR “continuous”). See Supplemental Part A for a more detailed presentation of the search strategy.
Inclusion and exclusion criteria
The eligibility criteria were reported according to the Population, Intervention, Comparison, Outcome, and Study design approach. 19 Studies were included that matched the following criteria:
i. Participants: Patients were diagnosed with COPD defined by best post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity ratio <0.7;
ii. Intervention: The intervention was mainly lower limb aerobic training with quantifiable intensity based on a maximal test (i.e., Wpeak), and the experimental intensities or types were reported; Groups receiving multiple interventions (e.g., resistance training) were not considered.
iii. Comparator: The control group underwent lower limb aerobic training with intensity or type of exercise different from that of the intervention group, conventional health education, and usual care;
iv. Outcomes: We assessed exercise capacity using peak work rate (Wpeak) and the 6-min walking test (6-MWT). Lung function was evaluated by measuring peak minute ventilation (VE) and the percentage of predicted FEV1 (FEV1pred%). Dyspnea was assessed using the Modified Medical Research Council (mMRC) scale. Quality of life was measured with the Chronic Respiratory Questionnaire (CRQ). The study should include at least one of the above outcomes.
v. Study design: Randomized controlled trials (RCTs) were included. Articles without an abstract or full text published were excluded.
Those studies that could not meet the above criteria were excluded from this review, for example, COPD with other predominant diagnosis, published abstract only, or unpublished data.
Data extraction
Two researchers independently extracted the primary information from a pre-set standardized form. The following data were extracted: (1) Basic information, including first author and year of publication. (2) Characteristics of participants, including sample size, age, and gender. (3) Intervention details include the treatment, dosage, duration, process, and follow-up period. (4) Outcomes information. If the data were not presented in textual format, the “GetData Graph Digitizer” software was utilized to extract the information from visual representations. If necessary, the corresponding authors were contacted for additional information. According to previous research and guidance, exercise intensity was categorized as high intensity (⩾80% of peak work capacity), medium intensity (>50% and < 80% of peak work capacity), and low intensity (⩽50% of peak work capacity).11,20,21 Two researchers (ZTQ and ZWK) independently screened the studies obtained and then analyzed the title, abstract, and full text. An independent researcher (KL) will evaluate if conflicting viewpoints arise.
Risk of bias
Cochrane tool for randomized trials (RoB 2.0) was used by two independent researchers (QZT and ZWK) to assess the methodological quality of the RCTs. 22 The third researcher (KL) resolved disagreements as required. During the evaluation process, the risk of bias was assessed based on five domains: randomization process, deviations from the expected interventions, missing outcome data, outcome measurement, and selection of reported outcomes.23,24 Publication bias was assessed via visual inspection of funnel plots. If all areas are classified as “low risk,” the study is considered to have a “low concern.” When an area was categorized as “some concerns,” the study was deemed to possess an “unclear risk of bias” (including inapplicability and lack of information). When one or more areas are rated as having a “high risk,” these studies were regarded as situated in “high concern” areas.
Certainty assessment
The certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology. 25 In adherence to the GRADE system of rating the certainty of the evidence, we rated the certainty for each comparison and outcome as high, moderate, low, or very low. All comparisons were initially rated as “high” due to the inclusion of RCTs but subsequently downgraded based on risk of bias, inconsistency, intransitivity, heterogeneity, imprecision, and publication bias. 26
Statistical analysis
The Stata v16.0 (StateCorp LLC, USA), including the network package and the network diagram package, was utilized for network meta-analysis. The network package employed a random effects model and a frequency-based framework to analyze networks. A visual representation in the form of a network diagram was created, where nodes and lines were used to depict different interventions, with node size indicating population size and line thickness representing the number of studies conducted. In continuous variables, effect sizes were estimated using a mean difference with 95% confidence interval (CI). According to the recommendations of the Cochrane Handbook, if data on the change in standard deviation (SD) of outcomes from baseline were missing, estimates would be based on standard error, 95% CI, p values, or t-statistics. The results obtained from the network meta-analysis encompass all possible pairwise comparisons, including mixed comparisons that combine direct and indirect comparisons. The node-splitting tests assessed local inconsistencies between direct and indirect comparisons. If p < 0.05, it indicates the presence of local inconsistency. In case of observed inconsistency, non-transitivity was suspected, and potential confounding factors that may influence treatment effects were examined. The effectiveness of different interventions is evaluated using the surface under the cumulative ranking curve (SUCRA). SUCRA values range from 0% to 100%, where a SUCRA value of 100% signifies the most effective treatment, while smaller values indicate poorer treatment effects.
Results
Literature screening process and results
The PRISMA flowchart 27 was presented in Figure 1. The initial electronic search identified 17,925 potentially relevant publications. After removing 8296 duplicate records, a total of 9629 records were screened based on reading titles and abstracts, resulting in the exclusion of 9592 records. Among the remaining 37 studies eligible for full-text review, 22 were excluded based on inclusion and exclusion criteria, specifically, 4 non-randomized controlled trials,14,28 –30 1 single-arm experimental study, 31 14 studies32 –45 with interventions lacking quantifiable intensity, 2 studies46,47 without the inclusion of the purpose outcome, and 2 studies48,49 with incomplete/abnormal data. Ultimately, 15 RCTs50 –65 were included.
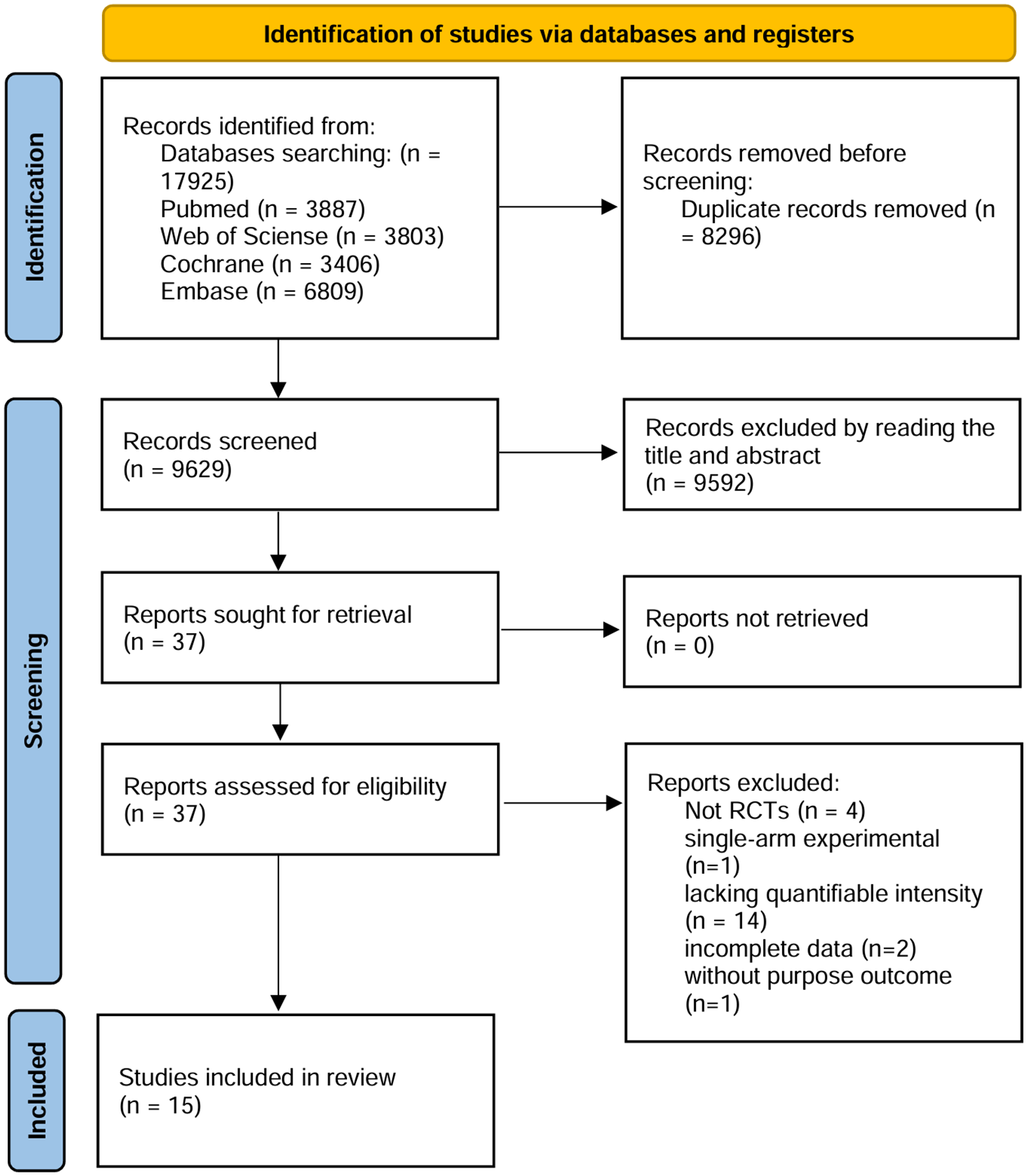
Flow diagram of the studies screened and included according to the PRISMA.
Description of included studies
The study was comprised of 15 studies with 979 participants, including two 3-arm studies. A total of 10 countries contributed to the publication of these studies, with Greece being the most prolific (4 studies, 26.7%). The average age of the participants was 67 years. The duration of the interventions in the 15 studies varied from 3 to 16 weeks, with a predominant treatment period of approximately 8 weeks (5 studies, 33.3%). Among these interventions, HIIT was included in 11 studies, HICT in 4 studies, MICT in 9 studies, LICT in 2 studies, self-paced training (SP) in 2 studies, and usual care (UC) in 4 studies. Twelve studies included Wpeak as an outcome measure; eight studies reported 6-MWT outcomes, FEV1pred% was assessed in four studies, VE was compared across nine studies, mMRC outcomes were reported by three studies, and CRQ results were analyzed by four studies (Figure 2 and Table 1).

Network diagram for Wpeak (a), 6-MWT (b), FEV1pred% (c), VE (d), mMRC (e), and CRQ (f). Each node represents an intervention that has been tested in studies; the size of the nodes is proportional to the number of patients that have received that intervention, and the thickness of the edges is proportional to the number of studies.
Summary of study characteristics.

Data expressed as mean ± SD.
6-MWT, 6-min walking test; CRQ, Chronic Respiratory Questionnaire; FEV1pred%, percentage of predicted forced expiratory volume in 1 second; HICT, high-intensity continuous training; HIIT, high-intensity interval training; LICT, low-intensity continuous training; MICT, moderate-intensity continuous training; mMRC, modified Medical Research Council; SP, self-paced training; UC, usual care; VE, peak minute ventilation; VO2max, maximal oxygen consumption; Wpeak, Peak Work rate (W).
NMA of efficacy outcomes
Peak work rate
Twelve studies involving 595 patients with COPD were analyzed for Wpeak. HIIT showed the highest improvement in Wpeak (85.0%), followed by MICT (80.9%), HICT (61.3%), LICT (50.7%), SP (21.2%), and UC (0.9%; e-Figure 1(A)). HIIT showed a significant improvement compared to SP and UC (MD 11.70 (95% CI 6.93, 16.46) and 18.48 (95% CI 12.66, 24.42)), respectively. Similarly, MICT showed a significant improvement compared to SP and UC (MD 11.43 (95% CI 6.67, 16.20), MD 18.28 (95% CI 11.20, 25.22)), respectively. HICT also showed a significant improvement compared to SP and UC (MD 9.24 (95% CI 4.38, 14.09), MD 16.08 (95% CI 8.19, 23.84)), respectively. However, LICT only significantly improved compared to UC (MD 13.47 (95% CI 4.77, 22.13)). SP was superior to UC but without a significant difference (Figure 3(a) and e-Figure 2).

Summary effects of interventions on changes in Wpeak (a), 6-MWT (b), FEV1pred% (c), VE (d), mMRC (e), and CRQ (f). The arrow in the upper right corner indicates the direction of improvement.
Six-minute walking test
Eight studies involving 620 patients with COPD were analyzed for 6-MWT. HIIT (82.9%) was ranked highest in 6-MWT, followed by HICT (74.3%), MICT (63.4%), LICT (39.7%), SP (29.6%), and UC (10.0%; e-Figure 1(B)). HIIT showed a significant improvement compared to SP and UC (MD 40.00 (95% CI 22.60, 57.40), MD 67.73 (95% CI 34.89, 100.57)). HICT was also significantly better than SP and UC (MD 36.90 (95% CI 18.81, 54.99), MD 64.64 (95% CI 28.70, 100.57)). Similarly, MICT showed significantly better than SP and UC (MD 34.19 (95% CI 21.39, 46.99), MD 61.92 (95% CI 28.34, 95.51)). LICT and SP did not significantly improve compared to UC. (Figure 3(b) and e-Figure 3).
Percentage of predicted forced expiratory volume in 1 second
Four studies, including 294 patients with COPD, were analyzed for FEV1pred%. HICT (59.5%) shows the highest improvement in peak work rate (W), followed by HIIT (58.7%), SP (56.1%), UC (47.4%), and MICT (28.3%) (e-Figure 1(C)). No significant differences were observed between HIIT, HICT, MICT, LICT, SP, and UC (Figure 3(c) and e-Figure 4).
Peak minute ventilation
Nine studies involving 502 patients with COPD were analyzed for VE. HIIT (87.1%) showed the highest efficacy in improving peak VE, followed by MICT (62.4%), HICT (53.4%), SP (44.3%), LICT (41.9%), and UC (10.9%; e-Figure 1(D)). Both HIIT and MICT demonstrated a significant improvement compared to UC, with MD 6.26 (95% CI 2.81, 9.72) and 4.34 (95% CI 0.13, 8.55), respectively. No significant differences were observed among other interventions (Figure 3(d) and e-Figure 5).
Modified Medical Research Council
Three studies involving 223 patients with COPD were analyzed for mMRC. HIIT (83.0%) and MICT (82.8%) demonstrated the highest efficacy in improving mMRC, followed by SP (21.7%) and UC (12.5%; e-Figure 1(E)). No significant differences were observed in the network comparison. MICT and HIIT significantly improved compared to SP (MD −0.44, 95% CI −0.80, −0.08; MD −0.44, 95% CI −0.82 to −0.06). Similarly, both MICT and HIIT showed a significant improvement compared to UC. (MD −0.53, 95% CI −0.91, −0.15; MD −0.53, 95%CI −0.89, −0.17; Figure 3(e) and e-Figure 6).
Chronic Respiratory Questionnaire
Three studies, including 324 patients with COPD, were analyzed for CRQ. MICT (74.1%) and HIIT (69.5%) demonstrated the highest efficacy in improving peak VE, followed by LICT (51.0%). In comparison, UC (5.4%) exhibited the lowest effectiveness (e-Figure 1(F)). Both HIIT and MICT showed a significant improvement compared to UC (MD 10.80 (95% CI 1.65, 19.95), MD 10.83 (95% CI 1.68, 19.98)). Although LICT outperformed UC, the CIs of these differences in CRQ crossed the null value of 0 (Figure 3(f) and e-Figure 7).
Bias and quality of evidence ROB
One study was assessed as low risk, nine as of some concern, and five as high risk of bias. Regarding each specific domain, the randomization process was classified as low risk of bias in 14 (93.3%) of studies; the deviations from the intended interventions domain were classified as low risk of bias in 1 (6.7%); the missing outcome data domain was classified as low risk of bias in 10 (66.7%); the measurement of the outcome domain was classified as low risk of bias in 14 (93.3%); and the selection of the reported result was classified as low risk of bias in 13 (86.7%; e-Figures 8–15).
Certainty of evidence
The evidence quality of all 67 comparisons was assessed using the GRADE system. Among these, 42 comparisons involved mixed effects (i.e., a combination of direct and indirect effects), while 26 were indirect. Within the mixed-effect group, 8 were deemed moderate-quality evidence, 21 had low-quality evidence, and 1 had very low-quality evidence. All 26 indirect comparisons were rated as very low-quality evidence (e-Figures 2–7).
Comparing efficacy on pairs of outcomes
We evaluated the efficacy of each intervention pair. HIIT, HICT, and MICT demonstrated higher effectiveness in improving 6-MWT and Wpeak, followed by LICT, SP, and UC (Figure 4(a)). For FEV1pred% and VE scores, HIIT, HICT, and SP ranked higher, followed by MICT, UC, and LICT (Figure 4(b)). In terms of improving mMRC and CRQ scores, MICT and HIIT ranked higher, followed by LICT, SP, and UC. At the same time, HICT was not included in the rankings due to insufficient data (Figure 4(c)). The comprehensive pair comparison was presented in e-Figure 16.

Scatterplots of the overall SUCRA score (ranking probability) of improving pairs of efficacy outcomes. (a) 6-MWT and Wpeak. (b) FEV1pred% and VE. (c) mMRC and CRQ.
Inconsistency test
No inconsistencies were identified in Wpeak, 6-MWT, FEV1pred%, mMRC, and CRQ. No overall inconsistency was detected in VE, but local inconsistencies in the MICT and LICT of VE were revealed. Only one study directly compared MICT and LICT for VE. After conducting a sensitivity analysis of the literature for indirect comparisons, no sources of heterogeneity were discerned.
Discussion
The network meta-analysis included 15 randomized clinical trials involving data from 979 participants. Results of SUCRA, with very low to moderate evidence, suggested that HIIT emerged as the optimal choice for improving exercise capacity (Wpeak and 6-MWT), lung function (VE), and Dyspnea (mMRC), and MICT was the preferred option for enhancing quality of life (CRQ). Regarding outcomes, no significant differences were observed among HIIT, HICT, MICT, and LICT. As hypothesized, we identified an intensity-dependent response and a lower improvement ceiling, making HIIT and MICT superior and most effective for all outcomes of interest. The intensity-dependent means that higher exercise levels yield better clinical effects. The lower improvement ceiling in patients with COPD is demonstrated by the lack of further improvement with HICT compared to MICT. 13 This study builds on Zainuldin’s 2011 meta-analysis 11 but goes beyond a simple update. While Zainuldin’s analysis compared higher-intensity versus lower-intensity training and continuous versus interval training, it found no significant differences between these methods. The current study expands the scope by incorporating more recent literature, refining the classification methods for the first time, and utilizing an NMA to enable broader and more detailed comparisons. Specifically, this NMA provides an extensive synthesis of quantitative data from RCTs in COPD rehabilitation to examine the different effects of different intensities and types of lower limb aerobic exercise in patients with COPD.
The exercise capacity serves as the most immediate manifestation of the impact of training. 66 Morris et al. proposed that higher exercise intensity may enhance skeletal muscle oxidative capacity and capillary density. 67 In exercise capacity, both HIIT and continuous moderate to high-intensity lower limb aerobic exercise significantly improved Wpeak and 6-MWT compared to UC and SP. At the same time, LICT only significantly improved Wpeak compared to UC. 68 Furthermore, Latimer et al. proposed that whole-body and muscle mitochondrial responses to exercise were robust in healthy individuals, evident in healthy old individuals, but deficient in patients with COPD. 69 This partly explains the poor performance of the COPD patients to sustain an HICT throughout the whole training program. It supports that improving exercise capacity necessitates a certain level of exercise intensity in patients with COPD.68,70 However, MICT showed superior efficacy to HICT in enhancing Wpeak, indicating that training intensity may not be the sole determinant of training outcomes in individuals with COPD. 71 Several studies proposed that high-intensity exercise could impair extradiaphragmatic respiratory muscle perfusion in patients with COPD.71,72 Similarly, HIIT provides appropriate rest during high-intensity training, demonstrating the highest exercise improvement ability. Additionally, respiratory challenges during HICT may impede patient participation, rendering higher-intensity exercises unsuitable for individuals with significant comorbidities. 73
In addition, current meta-analysis indicated that HIIT and MICT significantly improve VE, mMRC, and CRQ compared to UC. Butcher et al. proposed that exercise training generally enhances VE by promoting the restoration of elasticity following hyperventilation. 74 The lack of improvement in VE in the HICT group may be attributed to an excessive burden on the respiratory muscles. 75 Similarly, this negative effect was observed with high-volume/intensity resistance training. For example, single-limb low-load/high-repetition-resistance training did not further increase mean 6-MWT compared with two-limb low-load/high-repetition-resistance training, but it reduced exertional dyspnea and enabled more people to reach clinically relevant improvements in 6-MWT. 76 In addition, various lower limb aerobic exercises may not effectively improve FEV1pred%, suggesting that incorporating pulmonary function-focused training may yield superior effects for patients with COPD. 77 Furthermore, patients with COPD suffer from respiratory issues that act as a barrier to future planning, substantially impacting the quality of life. 78 Research indicates that HIIT and MICT, rather than LICT, are feasible for patients with COPD and can comprehensively improve their quality of life. 79 While the impact of HICT on mMRC and CRQ remains uncertain due to the lack of supporting studies, further comparisons across different intensities are still needed.
The study has certain limitations. First, the intensity classification is based on previous research. However, this classification may be debatable due to the absence of a universally accepted standard for exercise intensity in patients with COPD based on different research protocols. Additionally, the specificity of the metabolic data collection equipment influenced the decision to focus on lower limb aerobic training. It remains uncertain whether the findings from lower limb aerobic training can be extrapolated to training in other anatomical regions. Meanwhile, caution is warranted when interpreting the comparison results, as they may partially violate the assumptions of consistency and transitivity, and there is an increased risk of bias inherent to the NMA. Finally, the experimental results are limited by the small sample size, and further high-quality studies are necessary to validate the experimental results in the future, which is essential for developing precise exercise programs.
Conclusion
HIIT and MICT might be the optimal training approaches for patients with COPD. HICT did not demonstrate superior performance compared to MICT, potentially leading to more dyspnea. LICT showed only limited improvement. Optimal cost-effectiveness is not achieved with either excessive or insufficient training volumes. Furthermore, the limitations of the current study underscore the necessity for future research to validate these findings.
Supplemental Material
sj-docx-1-tar-10.1177_17534666251323190 – Supplemental material for Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs
Supplemental material, sj-docx-1-tar-10.1177_17534666251323190 for Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs by Zhengtong Qiao, Ziwei Kou, Jiazhen Zhang, Daozheng Lv, Xuefen Cui, Dongpan Li, Tao Jiang, Xinjuan Yu and Kai Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666251323190 – Supplemental material for Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs
Supplemental material, sj-docx-2-tar-10.1177_17534666251323190 for Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs by Zhengtong Qiao, Ziwei Kou, Jiazhen Zhang, Daozheng Lv, Xuefen Cui, Dongpan Li, Tao Jiang, Xinjuan Yu and Kai Liu in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.