
Abstract
Background:
Comorbidities of chronic obstructive pulmonary disease (COPD) influence clinical characteristics and prognosis.
Objectives:
This study compared the clinical characteristics and exacerbation rate of COPD according to the presence of depression or anxiety.
Design:
This study used data from The Korea COPD Subgroup Study (KOCOSS) cohort, a nationwide prospective cohort from 54 medical centers, between April 2012 and 2019.
Methods:
Depression and anxiety were diagnosed with the Beck Depression Inventory and Beck Anxiety Inventory. Negative binomial regression analysis was performed to analyze the frequency of exacerbations in depressed patients and anxiety. Differences in lung function trajectory according to presence of depression/anxiety were analyzed using a linear mixed model.
Results:
In all, 2147 patients were enrolled. Depressed patients or anxiety had lower lung function, higher modified Medical Research Council (mMRC) grade, St. George Respiratory Questionnaire (SGRQ) score, and COPD assessment test score, and higher rates of exacerbation in the past year than those without depression/anxiety. Depressed patients had a higher frequency of moderate to severe exacerbations [Incidence Rate Ratio (IRR): 1.57, CI: 1.17–2.11, p = 0.002] and those with anxiety had higher frequencies of moderate to severe (IRR: 1.52, CI: 1.03–2.27, p = 0.038) and severe exacerbations (IRR: 2.13, CI: 1.09–4.15, p = 0.025) during 1-year follow-up compared to those without these comorbidities. The differences in the change in annual forced expiratory volume in 1 seconds (FEV1) over 3 years according to the presence of depression or anxiety were not statistically significant.
Conclusion:
Depressed and anxious patients showed increased respiratory symptoms and exacerbation rate as well as reduced health-related quality of life, whereas there were no significant differences in changes in lung function between groups with and without depression/anxiety.
Background
Chronic obstructive pulmonary disease (COPD) is a disease with persistent respiratory symptoms and chronic airflow limitation, which is caused by a combination of small airway disease and parenchymal destruction due to exposure to toxic gases or particles.1,2 COPD constituted 55% of all chronic respiratory diseases in 2017 with a relative increase of 5.9% since 1990. It is estimated that over 300 million people worldwide are affected by COPD in 2019.3,4 COPD has several clinical impacts, including increased rates of mortality and various comorbidities.5,6 In addition, it is associated with a high socioeconomic burden, with the global economic burden of COPD in 2010 estimated to reach 49.9 billion dollars.7,8
The most important factors affecting the natural course of COPD are the frequency of exacerbations and the presence of comorbidities that impact disease progression and in turn worsen the prognosis of these patients.5,9,10 Psychological morbidities, such as depression and anxiety, are prevalent in COPD. Depression and anxiety have reported prevalence rates of approximately 25% and 40% in COPD, and prevalence may be associated with younger age, female sex, current smoking, poor lung function, and reduced health-related quality of life (QOL) in COPD patients.11–17 The prevalence of depression is also high in patients who have recently experienced exacerbations, and the presence of depression can influence patient mortality. 16 Depression and anxiety are associated with poor lung function and reduced health-related QOL in COPD patients. 18 Furthermore, previous studies in the United Kingdom and China have shown that depression and anxiety significantly increased the frequency of acute exacerbations in COPD patients.19–21
The aim of this study is to explore the differences in demographic and clinical characteristics, lung function trajectory, and exacerbation frequency among patients with COPD based on the presence or absence of depression or anxiety, in a nationwide multicenter Korean COPD cohort.
Methods
Study population and data collection
The Korea COPD Subgroup Study (KOCOSS) is a nationwide prospective cohort study from 54 medical centers in South Korea that began in April 2012.22,23 The inclusion criteria for the KOCOSS study were patient age ⩾ 40 years with fixed airway obstruction according to pulmonary function tests, defined as post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) < 70% of the normal predicted value. The clinical data of patients were collected using a case report form by a doctor or trained nurse. We used the data extracted from the KOCOSS database between April 2012 and 2019.
Clinical parameters
Baseline characteristics of patients obtained at the initial visit included age, sex, smoking history, and body mass index (BMI). The Beck Depression Inventory (BDI)-II and the Beck Anxiety Inventory (BAI) psychological tests were used to diagnosis depression and anxiety, respectively. Pulmonary function test parameters, for example, FEV1, FVC, FEV1/FVC, diffusing capacity of the lungs for carbon monoxide (DLCO), and residual volume/total lung capacity, were measured at baseline and annually for 3 years. Symptom scores, including the Modified Medical Research Council (mMRC) grade, St. George Respiratory Questionnaire (SGRQ) score, and COPD assessment test (CAT) score, were collected. Exercise tolerance was evaluated using the 6-Minute Walking Test (6MWT). Type 2 inflammation markers, including serum immunoglobulin E, fractional exhaled nitric oxide (FeNO), and blood eosinophil levels, were also measured. Furthermore, the presence of emphysema in chest computed tomography (CT) was assessed. Presence of comorbidities including heart failure, diabetes mellitus, hypertension, cancer, and chronic kidney disease were also collected. Medication regimes for COPD were classified as long-acting beta-agonist or long-acting muscarinic antagonist, long-acting beta-agonist plus long-acting muscarinic antagonist, inhaled corticosteroid plus long-acting beta-agonist, and triple therapy. Exacerbation was defined as acute deterioration of symptoms requiring further treatment. 1 Moderate exacerbation was defined as exacerbation that required antibiotics or systemic corticosteroid on an outpatient basis, whereas severe exacerbation was defined as that requiring an emergency room visit or hospital admission.
Definition of depression and anxiety
The BDI-II and BAI were used to define depression and anxiety in COPD patients. These self-assessment instruments are widely used worldwide to evaluate depression and anxiety, and there are numerous studies that have investigated their reliability and validity, including among Korean adults.24–26 BDI-II score ⩾ 10 was defined as indicating depression, and BAI score ⩾ 8 was defined as indicating anxiety according to the literature.27,28
Statistical analysis
Statistical analyses were performed using R software (ver. 3.6.3; R Development Core Team, Vienna, Austria). Data are expressed as the mean ± standard deviation or number and percentage. We compared clinical differences between patients with depression or anxiety and those without depression or anxiety. Clinical differences between two groups were analyzed using the χ2 test for categorical variables and Student’s t-test for continuous variables. Negative binomial regression analysis was performed to analyze differences in the frequency of exacerbations between patients with and without depression or anxiety. Age, sex, BMI, smoking history, FEV1, and past exacerbation history were adjusted in this analysis. The differences in annual FEV1 change over 3 years between groups were analyzed using a linear mixed model that revised the interaction between time and depression/anxiety. Age, sex, BMI, smoking history, and past exacerbation history were adjusted in this analysis. In all analyses, p < 0.05 was taken to indicate statistical significance. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement (Supplemental Table 1).
Results
Baseline characteristics
In all, 2147 patients with a mean age of 68.9 ± 7.7 were enrolled. Most patients were male (93.1%); 157 (7.4%) were never smokers and 1974 (92.6%) were ever smokers. Table 1 shows the baseline characteristics of all patients.
Clinical characteristics of patients.
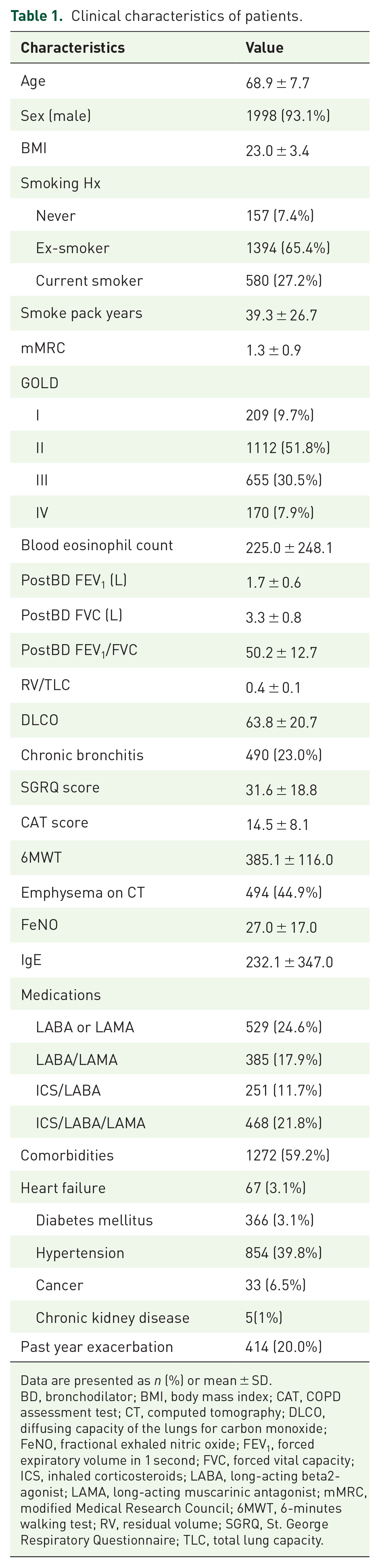
Data are presented as n (%) or mean ± SD.
BD, bronchodilator; BMI, body mass index; CAT, COPD assessment test; CT, computed tomography; DLCO, diffusing capacity of the lungs for carbon monoxide; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; ICS, inhaled corticosteroids; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; 6MWT, 6-minutes walking test; RV, residual volume; SGRQ, St. George Respiratory Questionnaire; TLC, total lung capacity.
Differences between patients with and without depression
Table 2 shows differences in baseline characteristics between patients with and without depression. The incidence of depression in the study population of COPD patients was 27.4%. Depressed patients smoked more (42.5 ± 29.8 pack years versus 37.5 ± 25.8 pack years, respectively, p = 0.008) and had lower FEV1/FVC (48.5 ± 13.8 versus 50.3 ± 12.2, respectively, p = 0.014), lower DLCO (60.5 ± 20.3 versus 64.2 ± 20.9, respectively, p = 0.013), higher mMRC grade (1.5 ± 1.0 versus 1.2 ± 0.8, respectively, p < 0.001), higher SGRQ score (41.2 ± 20.1 versus 25.7 ± 15.9, respectively, p < 0.001), and higher CAT score (18.3 ± 8.4 versus 12.1 ± 7.1, respectively, p < 0.001) than those without depression. Post-bronchodilator FEV1 did not significantly differ between the two groups. In addition, depressive COPD patients were more likely to have chronic bronchitis (30.2% versus 17.1%, respectively, p < 0.001), emphysema (54.1% versus 41.4%, respectively, p = 0.005), and a higher rate of exacerbation in the past year (24.8% versus 16.3%, respectively, p = 0.001) than those without depression.
Clinical characteristics of patients with depression and without depression.

Data are presented as n (%) or mean ± SD
BD, bronchodilator; BMI, body mass index; CAT, COPD assessment test; CT, computed tomography; DLCO, diffusing capacity of the lungs for carbon monoxide; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; ICS, inhaled corticosteroids; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; 6MWT, 6-minutes walking test; RV, residual volume; SGRQ, St. George Respiratory Questionnaire; TLC, total lung capacity.
Differences between patients with and without anxiety
Table 3 shows the differences in baseline characteristics between patients according to the presence or absence of anxiety. The rate of anxiety among COPD patients was 19.3%. Anxious COPD patients were younger than those without anxiety (67.3 ± 8.0 versus 69.7 ± 7.4, respectively, p < 0.001). There were no significant differences in FEV1 between the two groups, whereas DLCO was lower in the anxiety group (60.1 ± 19.2 versus 64.0 ± 20.2, respectively, p = 0.023). mMRC grade, SGRQ score, and CAT score were higher in the group with than without anxiety. Patients with anxiety were more likely to have chronic bronchitis (32.8% versus 16.6%, respectively, p < 0.001) and a history of exacerbation in the past year (28.5% versus 14.5%, respectively, p < 0.001).
Clinical characteristics of patients with anxiety and without anxiety.

Data are presented as n (%) or mean ± SD.
BD, bronchodilator; BMI, body mass index; CAT, COPD assessment Test; CT, computed tomography; DLCO, diffusing capacity of the lungs for carbon monoxide; FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; ICS, inhaled corticosteroids; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; 6MWT, 6-minutes walking test; RV, residual volume; SGRQ, St. George Respiratory Questionnaire; TLC, total lung capacity.
Association between depression/anxiety and frequency of exacerbation
Depressed patients had a higher frequency of moderate to severe exacerbations (IRR = 1.57, CI: 1.17–2.11, p = 0.002) during 1 year of follow-up than those without depression (Table 4). Patients with anxiety had higher frequencies of both moderate to severe (IRR = 1.51, CI: 1.02–2.26, p = 0.040) and severe exacerbations (IRR = 2.12, CI: 1.08–4.15, p = 0.026) during 1 year of follow-up than those without anxiety.
Frequency of exacerbation in patients with depression compared with without depression.

Adjusted variables: age, sex, BMI, smoking history, FEV1, past exacerbation history.
FEV1, forced expiratory volume in 1 second; IRR, incidence rate ratio.
Association between depression/anxiety and changes in lung function
The differences in the change in annual FEV1 over 3 years between groups with and without depression (p = 0.19) or anxiety (p = 0.97) were not statistically significant (Figure 1).

Lung function change in patients with depression and anxiety: (a) Depression, (b) Anxiety.
Discussion
We observed differences in clinical characteristics and exacerbation risk according to the presence or absence of depression or anxiety. Depressed patients were more likely to have higher smoking pack-years, more severe symptoms, chronic bronchitis, exacerbations in the past year, lower health-related QOL, and lower DLCO than those without depression. In addition, patients with anxiety were more likely to be younger, have more severe symptoms, chronic bronchitis, exacerbations in the past year, lower health-related QOL, and lower DLCO than those without anxiety. There were no significant differences in rates of lung function decline according to presence of depression or anxiety. We found that depressed patients were at higher risk for moderate to severe exacerbations, and those with anxiety showed significantly higher risk for moderate to severe and severe exacerbations during 1 year of follow-up than those without these comorbidities.
The impacts of comorbidities in COPD have been studied in detail, as they may substantially affect disease course and prognosis. These comorbidities may arise independently or be causally related to COPD; the two diseases may share risk factors or one disease may affect the severity of the other. 1 Depression and anxiety are among the most frequent comorbidities of COPD and are associated with poor clinical course.17,21,29,30 Several studies have investigated the relations between depression or anxiety and acute exacerbations of COPD, and our results are consistent with most of those studies. Of 24 studies included in a systematic review from the United Kingdom in 2014, 17 showed that depression and anxiety are significantly associated with higher risk of hospital admission and readmission due to acute exacerbation of COPD. 31 Yohannes et al. 19 demonstrated that a high depression score at baseline was associated with a significantly increased risk for moderate to severe exacerbations and severe exacerbations, whereas past moderate-to-severe exacerbation history was the strongest predictor of exacerbations during 3 years of follow-up. Similarly, Huang et al. 21 reported that depressed patients with a self-rating depression scale score ⩾ 53 and patients with a self-rating anxiety scale score ⩾ 50 had higher risk for acute exacerbation.
There are several possible reasons for the increased risk for COPD exacerbation in patients with poor mental health. There may be some risk factors in common between poor mental health and COPD exacerbation, for example, both cigarette smoking and poor socioeconomic status are risk factors for both COPD exacerbation and depression/anxiety.32–35 In addition, depressive and anxious patients may neglect use of medications, including inhalers, leading to reduced adherence to therapy, which may increase the risk for future exacerbation. 36 It is a vicious circle in that past exacerbations cause poor mental health, leading to reduced physical activity and QOL, which may provoke frequent exacerbation and lead to progressive worsening of the patient’s condition. 36 Finally, there is evidence that systemic inflammation may be associated with depression and lung function decline in COPD patients, which may explain the increased risk for exacerbation in depressive patients. 37
Our data showed no significant differences in lung function according to the presence of depression or anxiety. However, previous studies have shown that depressive patients have greater impairment of lung function.18,29,38 Consistent with Yohannes et al., 29 we also found no significant differences in lung function decline according to the presence or absence of depression or anxiety. Interestingly, in our study, depressive or anxious patients had decreased DLCO compared to patients in good mental health. Frequent presentation of chronic bronchitis may explain reduced DLCO in depressed patients and anxiety, but further investigations are necessary to address this issue. 39
Due to their clinical and socioeconomic importance, it is important to manage psychological comorbidities in patients with COPD. Depressive patients with COPD have a significantly increased rate of suicide attempts compared to non-COPD patients.40–42 However, only 27–33% of depressed COPD patients receive treatment for depression. 31 As there may be veiled psychological comorbidities among COPD patients, efforts should be made to identify depressed/anxious patients and administer appropriate treatment, including psychological and pharmacological interventions as well as pulmonary rehabilitation. Psychological therapy includes relaxation therapy, cognitive behavioral therapy, and self-management strategies. 43 Several studies have reported positive effects of psychological therapy in COPD patients.44–46 A systemic review showed that mind–body exercise (e.g. yoga, qigong) can improve the symptoms of depression and anxiety in COPD patients, which may be part of the benefits of relaxation therapy. 47 In terms of pharmacotherapy, some studies have reported improvement of symptoms using selective serotonin reuptake inhibitors and tricyclic antidepressants in COPD patients.48,49 In addition, some studies have shown the importance of pulmonary rehabilitation in depressed and anxious COPD patients.50,51
This study had some limitations. First, the patients enrolled in our study were from the KOCOSS cohort and were mostly from tertiary hospitals, and so may not be representative of the general population. Second, as most enrolled patients were male (93.1%) and smokers (92.6%), the population may not accurately reflect depression and anxiety in COPD patients as both are associated with female sex and nicotine dependence.29,32 Third, as the cutoff value of the BDI score was lower than in some other studies, patients with milder depression may have been included in our cohort 26 ; we used a BDI cutoff value of 18 points, and although there was a trend, it was not statistically significant. However, as a BDI score of 10 has been validated in several studies, the cutoff value of 10 points may also be appropriate.28,52,53
Conclusion
Depression and anxiety are both associated with more severe symptoms and poorer health-related QOL in patients with COPD. In addition, depression and anxiety can independently predict the frequency of exacerbations of COPD, which is associated with prognosis. Therefore, this study provides evidence that mental health should be taken into account when treating patients with COPD, particularly those with severe symptoms and frequent exacerbations. Clinicians should always strive to evaluate depression and anxiety early, from the diagnosis of COPD to the treatment period, to manage them appropriately.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231216591 – Supplemental material for Associations between depression and anxiety index and frequency of acute exacerbation in chronic obstructive pulmonary disease
Supplemental material, sj-docx-1-tar-10.1177_17534666231216591 for Associations between depression and anxiety index and frequency of acute exacerbation in chronic obstructive pulmonary disease by Yu Jin Hong, Youlim Kim, Ji-Yong Moon, Shinhee Park, Jung-Kyu Lee, Ki-Suck Jung, Kwang Ha Yoo, Yu-Il Kim and Joon Young Choi in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.