
Abstract
Background and aims:
Patients discharged after treatment for acute exacerbation of chronic obstructive pulmonary disease (COPD) are at high risk for readmission. We aimed to identify the prevalence and risk factors for readmission.
Methods:
We included 16,105 patients who had claimed their medical expenses from 1 May 2014 to 1 May 2016 after discharge from any medical facility in Korea, following treatment for acute exacerbation of COPD. We analysed the potential risk factors for readmission within 30 days of discharge.
Results:
Readmission rate was 26.4% (3989 patients among 15,101 patients) and over 50% of readmissions occurred within 10 days of discharge. Approximately 57% of readmissions occurred due to respiratory causes. Major causes of readmission were COPD (27%), pneumonia (14.2%), and lung cancer (7.1%), in that order. Patients who were readmitted were male, had more comorbidities and were less frequently admitted to tertiary hospitals than those who were not readmitted. Risk factors for readmission within 30 days of discharge were male sex, medical aid coverage, longer hospital stay, longer duration of systemic steroid use during hospital stay, high comorbid condition index, and discharge to skilled nursing facility.
Conclusion:
Readmission occurred in approximately one-quarter of patients, and was associated with patient-related and clinical factors. Using these results, we can identify high-risk patients for readmission and precautions are needed to be taken before deciding on a discharge plan. Further research is needed to develop accurate tools for predicting the risk of readmission before discharge, and development and evaluation of an effective care programme for COPD patients are necessary.
The reviews of this paper are available via the supplemental material section.
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most common leading causes of mortality worldwide. 1 Prevalence of COPD was reported to be 13.1–14.6% in Korea, which is higher than the worldwide prevalence. 2 Acute exacerbation of COPD can be defined as the acute deterioration of the status of COPD patients, and it is characterized by aggravation of respiratory symptoms such as cough, sputum, and dyspnoea. It leads to patients visiting clinics earlier than scheduled and can even result in hospitalization. Acute exacerbation of COPD (AECOPD) can occur during the natural course of COPD and is related to disease progression. Furthermore, exacerbation of COPD not only affects an individual’s physical health with regard to decrease in lung function, 3 increased risk of future events of exacerbation, 4 and mortality, 5 but also their socioeconomic status due to increased medical expenses and strain on resources. 6 Severe exacerbation of COPD requires hospitalization, which is responsible for 70% of COPD-related healthcare expenditure. 7 Patients who have been admitted to the hospital for severe exacerbation are at high risk of being readmitted, further worsening the situation.
Readmission within 30 days of discharge from previous hospitalization for AECOPD is reported to occur in 20% of patients.8,9 Regardless of the cause of readmission, patients who are readmitted within 30 days of discharge from index hospitalization have unfavourable clinical outcomes and even have increased mortality for the next three years. Interestingly, these adverse effects were not exclusively dependent on impaired lung function. 10
South Korea implemented a single, compulsory government-established health insurance system called the National Health Insurance (NHI) in 1998 that covers 97% of the population in South Korea, and the remaining 3% is covered by the Medical Aid Programme. 11 The Health Insurance Review and Assessment Service (HIRA), an agency responsible for evaluating all medical claim data from all hospitals in Korea, evaluates the eligibility of claimed medical expenses and approves insurance reimbursements from the NHI service. It also collects all medical records of patients provided by physicians for insurance claims.
Identifying prevalence and risk factors associated with early readmission within 30 days of previous hospitalization could be helpful in developing practical interventions for reducing readmission. There have been recent studies related to this, but few data from Asia countries. In the present study, we aimed to estimate the prevalence and clinical characteristics of patients who early readmitted after AECOPD. We also identified factors that would allow clinicians to distinguish patients who are at high risk for early readmission in actual practice.
Material and methods
Data source and subjects
We analysed all medical information as recorded in the HIRA database from 1 May 2014 to 1 May 2016, keeping in mind the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) for diagnoses. To define index hospitalization due to AECOPD we used the following criteria: (1) ICD-10 code for COPD (J44) as the primary or secondary (first or second) diagnosis; (2) and use of systemic steroids for at least 3 consecutive days during hospital stay. Early readmission was defined as readmission within 30 days of discharge from index hospitalization with the presence of ICD-10 code for COPD (J44) as the primary or secondary diagnosis. Patients who had no insurance claim history after discharge from index hospitalization for the following year were considered deceased.
Patients with insurance claims for reimbursements from oriental hospitals, dental clinics, and maternity clinics were excluded. We also excluded claim data from hospitals which were unable to admit patients (e.g. primary health clinics and public health centres). Patients with no history of hospital visits within 3 months after index hospitalization were also excluded.
The institutional review board at the Kangdong Sacred Heart Hospital approved this study and waived the requirement for consent as we used publicly accessible and anonymized data (IRB No. KANGDONG 2019-04-006).
Items for evaluation
We evaluated demographic data (e.g. age and sex), type of insurance (e.g. health insurance and medical aid), type of hospital (secondary or tertiary centre), comorbid conditions with ICD-10 codes, and medication data in the HIRA service database. Intensive management measures during hospitalization such as transfer to intensive care unit (ICU), use of mechanical ventilator (MV) or non-invasive ventilation (NIV) were also identified in the HIRA database. The details of administration of systemic steroids (duration and cumulative dosage during hospitalization and prescription at discharge) and location of discharge (e.g. skilled nursing facility) were also included in the analysis.
Statistical analysis
The baseline characteristics of the patients and their hospital courses were compared using the t-test and Chi square test for continuous and categorical variables, respectively.
Logistic regression analysis was used to identify risk factors for readmission. Univariate and stepwise multivariate logistic analyses with variables selected by a significance level of entry of 0.1 were conducted to identify significant risk factors for early readmission. Data of Cox proportional hazards model analyses were presented as hazard ratios (HRs) and 95% confidence intervals.
All analyses were two-sided and conducted at a significance level of 0.05, unless otherwise stated. All analyses were conducted using the SAS software, version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Cohort selection
Among the 16,612 patients who were hospitalized for AECOPD, 16,142 were discharged but after excluding patients lost to follow-up and transferred to other hospitals, 15,101 patients were included in the analysis. The study flow is outlined in Figure 1.

Flowchart of data extracted from Health Insurance Review and Assessment Service, dated 1 May 2014 to 1 May 2016.
Readmission occurred in 26.4% of patients (3989 among 15,101 patients) after index hospitalization due to AECOPD. Among all causes of readmission, 38.6% and 66.4% occurred within 7 and 15 days after discharge, respectively (Figure 2).

Frequency and percentage of readmission after discharge from index hospitalization for acute exacerbation of chronic obstructive pulmonary disease.
Characteristics of subjects
Patients were divided into two groups: with readmission (n = 3989) and without readmission (n = 11,112). A greater proportion of patients with readmission were male and covered by medical aid than those without readmission (Table 1). Patients who were admitted to tertiary facilities were less likely to be readmitted. Almost all comorbid conditions were more common in patients with readmission, except peripheral vascular disease, and the Charlson Comorbidity Index was significantly higher in the readmission group (8.3 ± 2.5 with readmission vs. 7.3 ± 2.5 without readmission; p < 0.001). Comparing the medications for COPD management, long acting beta2 receptor agonist (LABA) was more frequently prescribed, whereas inhaled corticosteroid/long acting muscarinic receptor agonist was less frequently prescribed in the readmission group. The treatment measures, hospital course, and discharge characteristics at the time of index hospitalization are shown in Table 2. Patients with readmission were less likely to be admitted to the ICU (8.5% with readmission vs. 9.8% without readmission; p = 0.011) and less administered MV care (3.5% vs. 4.6%; p = 0.004). There was no significant difference in NIV use between the two groups. The dose of systemic steroids used for AECOPD was low in the readmission group (41.5 ± 47.7 with readmission vs. 45.2 ± 52.6, without readmission; p < 0.001), but there was no difference in duration of use. Total duration of hospital stay was shorter in the readmission group (15.3 ± 21.1 with readmission vs. 16.7 ± 39.7 without readmission; p = 0.006) than in the other group. Patients with readmission were less frequently prescribed systemic steroids at the time of discharge (77.3% vs. 80%; p < 0.001) than in the other group. None of the patients in the without readmission group were admitted to skilled nursing facilities during 30 days of discharge, while in the readmission group 5% were admitted.
Differences in patient characteristics depending on readmission status at 30 days after discharge.

Data are presented as number (%) or mean ± standard deviation.
ICS, inhaled corticosteroid; LABA, long acting beta2 receptor agonist; LAMA, long acting muscarinic receptor agonist; SABA, short acting beta2 receptor agonist.
Features of treatment measures, hospital course, and discharge of the index hospitalization.

Data are presented as number (%) or mean ± standard deviation.
ICU, intensive care unit; MV, mechanical ventilation; N/A, not-applicable; NIV, non-invasive ventilation.
Cause of readmission
Respiratory causes accounted for 57% of readmissions and cardiac causes were found in only 3% of patients (Figure 3). Among patients with early readmission, the main cause of readmission based on the ICD-10 code for their primary diagnosis was extracted and these are given in Table 3. The major cause of readmission after acute exacerbation was COPD (27%), followed by pneumonia (14.2%) and lung cancer (7.1%), irrespective of age 65. In males, the causes of readmission were identified as COPD (30.0%), pneumonia (14.7%), and lung cancer (8.7%), in that order. In females, the most frequent causes of readmission were COPD (27.4%), pneumonia (13.0%), and dementia (7.4%).

Causes of 30-day readmission.
Cause of 30-day readmission.
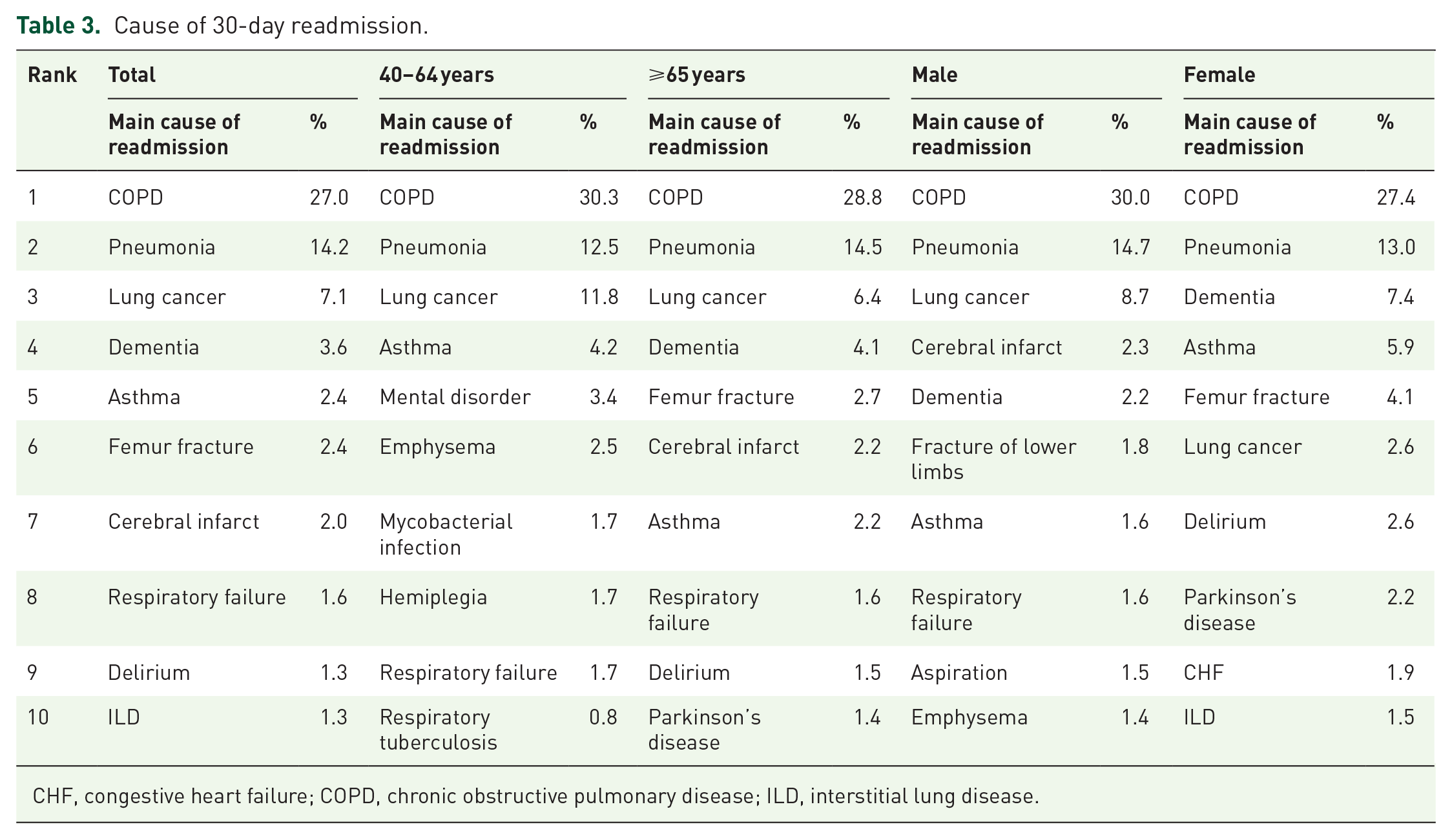
CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; ILD, interstitial lung disease.
The distribution of readmissions due to respiratory and cardiac reasons within 30 days of discharge is presented in Supplemental Material Figures 1 and 2 online.
Risk factors for readmission
Using multiple logistic regression analysis, we found that factors related to increased risk of readmission within 30 days of discharge were being male (HR, 1.20), getting medical aid care (HR, 1.15), hospital stay more than 7 days (HR, 26.87), higher comorbidity index (HR, 1.20), discharge to skilled nursing facilities (HR, 1.82), and longer duration of systemic steroid use in hospital stay (HR, 1.23) (Table 4). Type of inhaler treatment did not significantly affect the risk of readmission. Factors associated with respiratory causes of readmission were similar to those for any other cause of readmission (Supplemental Table 1).
Risk factors associated with all causes of readmission.
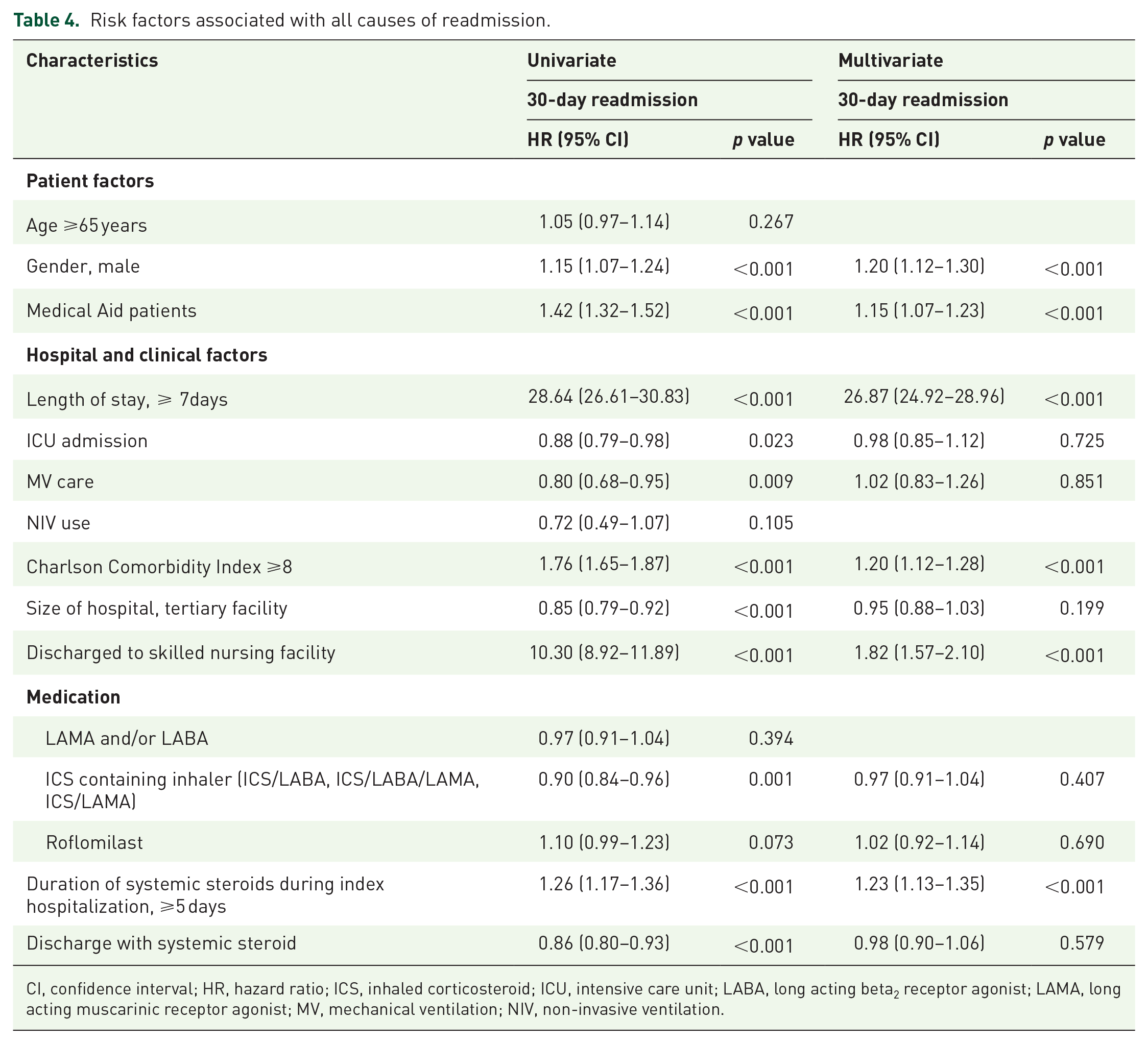
CI, confidence interval; HR, hazard ratio; ICS, inhaled corticosteroid; ICU, intensive care unit; LABA, long acting beta2 receptor agonist; LAMA, long acting muscarinic receptor agonist; MV, mechanical ventilation; NIV, non-invasive ventilation.
Discussion
This report details the prevalence of COPD and its clinical features using a nationwide database of COPD patients. We found that a considerable number of COPD patients who were hospitalized for acute exacerbation eventually went through repeated hospitalizations. We also demonstrated that a number of patient-related and clinical factors were associated with readmission, including sex, higher comorbidity burden, medical aid coverage, duration of systemic steroid use during index hospitalization.
Each year, COPD is responsible for as many as 800,000 hospitalizations, and approximately 20% of patients experience rehospitalization within 30 days of discharge.8,12 It is estimated that nearly 50 billion US dollars are spent on COPD-related healthcare expenditure annually, and rehospitalization-related healthcare costs alone account for over 15 billion US dollars in the United States.6,13 Considering the social and financial impact of rehospitalization in COPD patients, there have been several clinical trials14–16 for developing a COPD-specific risk stratification tool to predict patients who are at high risk of readmission or interventions to reduce rehospitalization. However, no such tool has been found to be effective. Boourbeau et al. 16 and Casas et al. 15 reported interventions that focused on disease-specific programmes (e.g. COPD education and teaching inhaler use) and post-discharge programmes (e.g. home visits, telephone call, and patient hotline) to reduce rehospitalization. Notably, they only focused on reducing rehospitalizations at 12 months and not on decreasing early rehospitalization as the endpoint. On the other hand, Fan et al. 14 reported termination of a clinical trial due to unanticipated excess mortality in an intervention group that received a COPD care programme including education. In addition to the heterogeneity of study designs, many trials have dealt with the effectiveness of post-discharge interventions that may not have consistent results.
Under these circumstances, the Hospital Readmission Reduction Programme (HRRP) included AECOPD as a targeted medical condition. 17 In response to the HRRP, Ohar JA et al. 18 performed a retrospective observational cohort study and reported that a comprehensive care plan for AECOPD admission reduced all-cause readmission and mortality at 30 days from discharge. This implies that an effective intervention could improve outcomes for COPD patients. However, before the implementation of an intervention, it is necessary to find and validate the causes of readmission and predictors in a large cohort and to develop an individual-focused readmission risk stratification tool. Relatively consistent predictors of readmission include a history of previous admission, comorbid conditions, prolonged length of stay, and Medicaid support 19 but there are no uniformly accepted prediction tools that can reliably assess the risk for early readmission. Moreover, there have been few data in Asia, so trials to reduce readmission are difficult to launch.
Recently, David et al. 20 analysed a nationwide readmission database in the United States for AECOPD in accordance with the HRRP, and found early readmission within 30 days after index AECOPD admission was associated with both patient-related factors (Medicaid payer status, low household income, and more comorbid condition) and clinical factors (longer hospital stay and discharge to a skilled nursing facility). Similarly, these factors were reconfirmed in our study using another nationwide database. In addition, our study found that sex and systemic steroid use significantly influenced rehospitalization. The effect of sex on susceptibility to readmission after AECOPD is controversial. Male sex was one of the risk factors for death and rehospitalization after a severe event of AECOPD.4,21,22 However, some have suggested that males have a lower risk of adverse outcomes from COPD than females. 23 Although the characteristics and prognosis of COPD patients by sex have not been fully elucidated, susceptibility to toxic inhalation, airway structures, and female sex hormone have been identified as relevant factors.24,25 Recommendations for the management of COPD include systemic steroid treatment for 5 to 7 days 26 and a daily dose of 40 mg prednisone. 27 Although the mechanisms for clinical improvement of lung function, oxygenation, and outcomes (i.e. early relapse, treatment failure, and length of hospitalization) among patients who are administered corticosteroids during exacerbation events have not been fully elucidated, reduction in airway inflammation or decrease in airway oedema may be contributing factors. 28 We reported interesting results for association between corticosteroids and early readmission in AECOPD patients by showing that corticosteroid use for more than 5 days was associated with an increased risk of rehospitalization. Our results correspond to recent meta-analysis results and recommendations that long-term corticosteroid use during hospitalization has no benefit compared with short-term use. 29
This is the first study to report on the status and related predictors of AECOPD rehospitalization using a nationwide healthcare database in Korea. Although the prevalence of readmission was relatively high, predictors of rehospitalization in this study were similar to those according to a US study by David et al. 20 However, we further discovered that the use of systemic steroids was a significant factor associated with readmission.
Respiratory reasons account for 57% of readmissions and were the most common causes of readmission for COPD-related events regardless of both age and sex. Cardiac causes of readmission included heart failure, ischaemic heart disease, and arrhythmias, which cumulatively accounted for 3% of readmissions. The remaining 40% of readmissions were due to conditions other than respiratory and cardiac causes. We evaluated the natural course (up to 30 days) of patients who were discharged after acute exacerbation of COPD and found that there were some differences in the pattern of occurrence depending on the cause of readmission. In particular, respiratory causes of readmission showed a pattern similar to that of all causes of readmission, accounting for more than half of the events (51.7%) that occurred within 10 days of discharge. The occurrence of events gradually decreased after this period. On the other hand, the majority of cardiac cause-related readmissions (48.5%) also occurred within 10 days of discharge, but even after 3 weeks of discharge more than 10% of events occurred and there was no pattern of gradual decrease. Congestive heart failure (CHF) has been reported to be the most common readmission diagnosis after respiratory-based disease according to studies conducted in the United States,8,9 and also one-fifth of COPD patients have been known to have unrecognized coexisting heart failure. 30 Unlike previous studies,8,9,20,31 we reported that the cardiac reasons for readmission after AECOPD in Korea accounted for as little as 3% of patients. Nationwide data have shown that Korean COPD patients have a lower body mass index, lower comorbid hypertension and dyslipidaemia, which are known as risk factors for cardiac disease, and a lower prevalence of myocardial infarct than other races or ethnic groups. 32 Similarly, low rates of cardiac cause-related readmissions may be due to racial differences. Additionally, it is not easy to distinguish symptoms and signs between heart failure and AECOPD in actual clinical practice. Thus, the clinical manifestations of heart failure commonly mimic those of AECOPD. Since there is no acceptable biomarker for COPD, unlike cardiac troponin in ischaemic heart disease 33 and B-type natriuretic peptide in CHF, 34 this overlap of symptoms and signs makes diagnosis difficult and complicates coding of the diagnosis at the time of hospitalization. Even readmission in patients with COPD is a very complex phenomenon considering various well-known comorbidities. A single disease-specific approach for prediction is probably not sufficient, especially since readmission itself in COPD patients is related to high healthcare costs and adverse outcomes. 6
This study has a strong advantage since it can be generalized; we could analyse medical claim data for all citizens due to the unique nature of the health insurance system in Korea. However, when interpreting the results of this study, some limitations should be considered. First, our study was based on the HIRA database and was observational and retrospective. Although a nationwide database provides a large sample size and various clinical data related to hospitalization and discharge, we did not include clinically important biomarkers for prediction of readmission risk such as forced expiratory volume in 1 s (FEV1), 35 body mass index, 36 and severity of dyspnoea. 37 Second, there is no objective index such as FEV1 to assess disease severity at the time of index hospitalization. However, considering the serious admission indicators, including ICU admission or MV care, it is estimated that the severity of AECOPD at that time was comparable between groups. Third, our 30-day readmission rate was relatively high and length of hospital stay at index hospitalization was longer compared with previous studies, possibly due to the relatively easy access to medical care in Korea and more comorbidities associated with prolonged treatment. Last, biases in estimating health care utilization and cause of readmission may be present because we used the ICD-10 code for defining hospitalization and readmission.
In conclusion, after AECOPD, a considerable number of Korean patients experience rehospitalization, which is one of the major concerns in the healthcare system considering the prevalence and socioeconomic impact of COPD. Considering the incidence of readmission within the first few days after discharge, a full assessment of the prognosis before discharge is necessary. We found that both patient-related and clinical factors contribute to the risk of readmission. These results are meaningful as they provide a better understanding of an individual patient’s risk of readmission. Further research is needed to develop accurate tools for predicting any possible subsequent adverse events. Clinicians can use these tools to understand when precautions need to be taken and to guide comprehensive care plans to reduce early readmission.
Supplemental Material
Author_Response_1 – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Author_Response_1 for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Supplemental Material
Online_Data_Supplement – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Online_Data_Supplement for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1_1 – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Reviewer_1_v.1_1 for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1_1 – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Reviewer_2_v.1_1 for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplementary_Figure_1 – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Supplementary_Figure_1 for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplementary_Figure_2 – Supplemental material for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease
Supplemental material, Supplementary_Figure_2 for Risk factors for early readmission after acute exacerbation of chronic obstructive pulmonary disease by Yong Suk Jo, Chin Kook Rhee, Kyung Joo Kim, Kwang Ha Yoo and Yong-Bum Park in Therapeutic Advances in Respiratory Disease
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
The reviews of this paper are available via the Supplemental Material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.