
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) is a major cause of mortality and morbidity worldwide. Many patients with COPD experience exacerbations that require hospitalization, which is associated with an increased risk of in-hospital death and impaired ability to perform activities of daily living (ADL). Declining ability to perform ADL is a critical issue for these patients.
Objectives:
To identify predictors of poor clinical outcomes, including in-hospital death and low ability to perform ADL at discharge, in patients who are hospitalized with exacerbation of COPD.
Design:
This retrospective study involved a cohort of patients with exacerbation of COPD who were admitted to Iwata City Hospital in Japan between July 2015 and October 2019.
Methods:
We collected clinical data, measured the cross-sectional area of the erector spinae muscles (ESMCSA) on computed tomography (CT) scans at admission, and investigated the associations of poor clinical outcomes (in-hospital death and severe dependence when performing ADL, defined as a Barthel Index (BI) of ⩽40 at discharge) with clinical parameters.
Results:
Overall, 207 patients were hospitalized for exacerbation of COPD during the study period. The incidence of poor clinical outcomes was 21.3%, and the in-hospital mortality rate was 6.3%. Multivariate logistic regression analyses showed that older age, long-term oxygen therapy, an elevated D-dimer concentration, and a reduced ESMCSA on chest CT at admission were significantly associated with poor clinical outcomes (in-hospital death and a BI of ⩽40).
Conclusion:
Hospitalization for exacerbation of COPD was associated with high rates of in-hospital mortality and a BI of ⩽40 at discharge, which may be predicted by assessment of ESMCSA.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality worldwide. 1 The COPD burden is expected to increase in coming decades because of continued exposure to COPD risk factors and aging of the population. 2 Therefore, an optimal COPD management approach must be established. COPD is a chronic disease, but its clinical course is often aggravated by exacerbations, which are clinically defined as episodes of increasing respiratory symptoms that require additional therapy. 3 Exacerbations have a negative impact on patients’ health status, 4 accelerate decreased ability to perform activities of daily living (ADL) and physical activities, 5 and result in disease progression. 6 Despite recent advances in COPD therapy, exacerbation is the leading cause of hospital admission and death during the clinical course. The risk of exacerbations is one determinant factor of disease severity, and the current guideline therefore emphasizes the importance of exacerbation prevention and treatment in the management of COPD. 7
Exacerbations requiring hospital admission are catastrophic events related to poor outcomes and an increased risk of death. 8 Previous studies have shown that the in-hospital mortality rate in patients with COPD exacerbation is in the range 2.9–10.4%.9–11 Even when these patients survive, many do not return to their pre-exacerbation state,5,12 and some cannot return to their home even after recovery from the exacerbation. Hospitalization for COPD exacerbation is strongly associated with declining ability to perform ADL and reduced physical activity levels. In patients with COPD, physical activity is a well-known strong predictor of long-term all-cause mortality, 13 and is associated with the frequency of exacerbations. 14 Predicting the clinical prognosis is important for clinicians to make decisions pertaining to the management of COPD exacerbation, for example, regarding rehabilitation to maintain physical activity, the length of hospital stay, support for hospital discharge, and advanced care planning when patients are admitted because of COPD exacerbation.
Several prognostic tools for COPD exacerbations have been introduced, but they mainly focus on mortality9,11,15 and readmission.16,17 Declining ability to perform ADL and physical activities is a critical issue in hospitalized patients with COPD exacerbation, but predictors of the ability to perform ADL have not yet been identified. Accurate predictors of poor clinical outcomes (including not only death, but also severe dependence when performing ADL at discharge) are needed for patients who are hospitalized for COPD exacerbation.
Antigravity muscles are more important for the performance of ADL than other muscles. 18 The erector spinae muscles (ESM) are a set of antigravity muscles, and the cross-sectional area of the ESM (ESMCSA), as assessed by chest computed tomography (CT), has been shown to be an excellent predictor for patients with chronic respiratory disease in a stable condition.19–21 ESMCSA is more closely associated with long-term mortality than other CT indices for patients with stable COPD. 21
Although the role of the ESMCSA in determining the clinical outcomes of patients with COPD exacerbation has not been established, we speculated that a reduced ESMCSA at admission is related to poor outcomes in hospitalized patients with COPD exacerbation. In this study, we aimed to identify predictors of poor clinical outcomes in hospitalized patients with COPD exacerbation, including severe dependence when performing ADL at discharge. We also examined whether the ESMCSA, as assessed by chest CT performed on admission, can predict poor clinical outcomes of hospitalization in these patients.
Materials and methods
Patients and methods
This retrospective study involved a cohort of consecutive patients with COPD exacerbation admitted to Iwata City Hospital in Japan from July 2015 to October 2019. Only the data from each patient’s first admission during the study period were included in the analysis. The inclusion criteria were (1) hospitalization because of a COPD exacerbation, (2) diagnosis of COPD based on spirometric evidence of airflow obstruction (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) of <0.70) when clinically stable, and (3) diagnosis of COPD exacerbation based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guideline. 7 The predicted values for pulmonary function tests were from the Japanese Respiratory Society. 22 The exclusion criteria were an age <50 years, a previous diagnosis of bronchial asthma, active malignancy, neuromuscular disease, a modified Rankin Scale score ⩾4, and hospitalization for a reason other than COPD exacerbation. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Institutional Review Board of Iwata City Hospital, Shizuoka, Japan (Certificate No. 2018-036). The need for patient approval and/or informed consent was waived because of the retrospective nature of the study.
Evaluation of ability to perform ADL
We used the Barthel Index (BI) to assess the ability of the patients to perform ADL at discharge. The BI is used to evaluate the ability to perform ADL, including feeding, transferring, grooming, toileting, bathing, dressing, walking, bowel or bladder control, and stair climbing. 23 The total BI is a cumulative score of 10 items, with a maximum score of 100 (fully independent) and a minimum score of 0 (totally dependent). In clinical practice, a low BI is associated with the loss of basic self-care skills. 23
Clinical outcomes
Patients with a BI >40 at discharge were categorized into the acceptable clinical outcomes group, while patients with a BI ⩽40 at discharge24,25 and those who died in the hospital were categorized into the poor clinical outcomes group. We evaluated the differences in demographic and clinical data between the two groups and determined the prognostic factors.
CT analysis
Chest CT imaging was performed in the supine position at the full inspiration breath-hold for diagnostic purposes on admission. For quantitative analysis of the ESMCSA, chest CT images were reconstructed using the mediastinal setting. The ESMCSA was calculated manually, in line with previous reports.19,26 Briefly, two adjacent axial images (contrast-unenhanced condition, 5-mm slice thickness) at the level of the lower margin of the 12th thoracic vertebra were selected for analysis of the ESMCSA and averaged for each patient. The left and right muscles were subsequently identified using a predefined attenuation range of −29 to 150 Hounsfield unit thresholds and manually shaded (see Figure 1). The ESMCSA was calculated as the average of the sum of the right and left muscles. All CT images were analyzed using SYNAPSE VINCENT version 3.3 (FUJIFILM Medical Co., Ltd., Tokyo, Japan). The image analyses and ESM calculations were independently performed by trained pulmonologists (YM and JS) blinded to the patients’ information.

A representative axial computed tomographic image used to measure the area of the erector spinae muscles in a hospitalized patient with exacerbation of chronic obstructive pulmonary disease.
Statistical analyses
Fisher’s exact test and the Mann–Whitney U test were used to compare clinical characteristics between the acceptable clinical outcomes and poor clinical outcomes groups of hospitalized patients with COPD exacerbation. Data are presented as number (percentage) or median [interquartile range (IQR)]. Univariate and multivariate logistic regression analyses were performed to identify the risk factors for poor clinical outcomes of hospitalization. Factors with a p < 0.05 in the univariate analyses were included in the multivariate model. Statistical tests were two-sided, and p < 0.05 was considered significant. All statistical analyses were performed using EZR version 1.41 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R version 3.6.1 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics and laboratory and imaging findings on admission
The data of 207 patients hospitalized for COPD exacerbation were analyzed in this study. The clinical characteristics of the study population are shown in Table 1. The median age of the patients was 79 years. The median body mass index (BMI) was 19.5 kg/m2. All patients had a history of smoking; the median number of pack-years was 55 and the FEV1 %predicted was 57.2% before the exacerbations. The percentages of patients treated with a long-acting muscarinic antagonist, long-acting β2-agonist, and inhaled corticosteroid before the exacerbations were 52.2%, 55.1%, and 29.5%, respectively, and 38 patients (18.4%) used long-term oxygen therapy (LTOT). The laboratory findings on admission are shown in Table 2. The median (IQR) pH, PaCO2, and PaO2/FiO2 ratio were 7.430 (7.379–7.464), 38.8 (33.5–50.1) Torr, and 264.8 (210.2–307.0), respectively. The white blood cell count and concentrations of C-reactive protein, brain natriuretic peptide, and D-dimer were slightly elevated. The median (IQR) ESMCSA, as assessed by CT, was 29.5 (24.1–35.6) cm2.
Characteristics of patients hospitalized for chronic obstructive pulmonary disease exacerbation according to clinical outcomes of hospitalization.

BMI, body mass index; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; LTOT, long-term oxygen therapy.
Data are expressed as median (interquartile range) or number (%).
Comparison between acceptable and poor clinical outcomes groups.
Laboratory findings on admission and therapies for exacerbation in patients hospitalized for chronic obstructive pulmonary disease exacerbation according to clinical outcomes of hospitalization.

CT, computed tomography; ESMCSA, cross-sectional area of erector spinae muscles.
Data are expressed as median (interquartile range) or number (%).
Comparison between acceptable and poor clinical outcomes groups.
Clinical outcomes of hospitalization
Overall, 13 patients (6.3%) died in the hospital, and 31 (15.0%) had BI scores ⩽40 at discharge. These 44 patients (21.3%) constituted the poor clinical outcomes group. A total of 163 patients (78.7%) were discharged with BI scores >40 and categorized into the acceptable clinical outcomes group (see Figure 2).

Distribution of outcomes in hospitalized patients with exacerbation of chronic obstructive pulmonary disease.
Compared with the patients in the acceptable clinical outcomes group, those in the poor clinical outcomes group were older (p < 0.001) and had a lower BMI (p = 0.021), lower FEV1/FVC (p = 0.036), and more frequent use of LTOT (p < 0.001). There was no significant group difference in the treatment for COPD before hospitalization (see Table 1). Among the laboratory findings on admission, there were significant differences in the PaCO2 (p = 0.038), PaO2/FiO2 ratio (p = 0.006), brain natriuretic peptide concentration (p = 0.003), and D-dimer concentration (p = 0.002) between the two groups. The poor clinical outcomes group had a lower ESMCSA (p < 0.001). The number of cases exhibiting pneumonia on the chest X-ray and CT scan did not differ significantly between the acceptable and poor clinical outcomes groups. There was also no significant group difference in the therapies administered for the exacerbation (see Table 2).
Univariate and multivariate analyses of risk factors for poor clinical outcomes of hospitalization
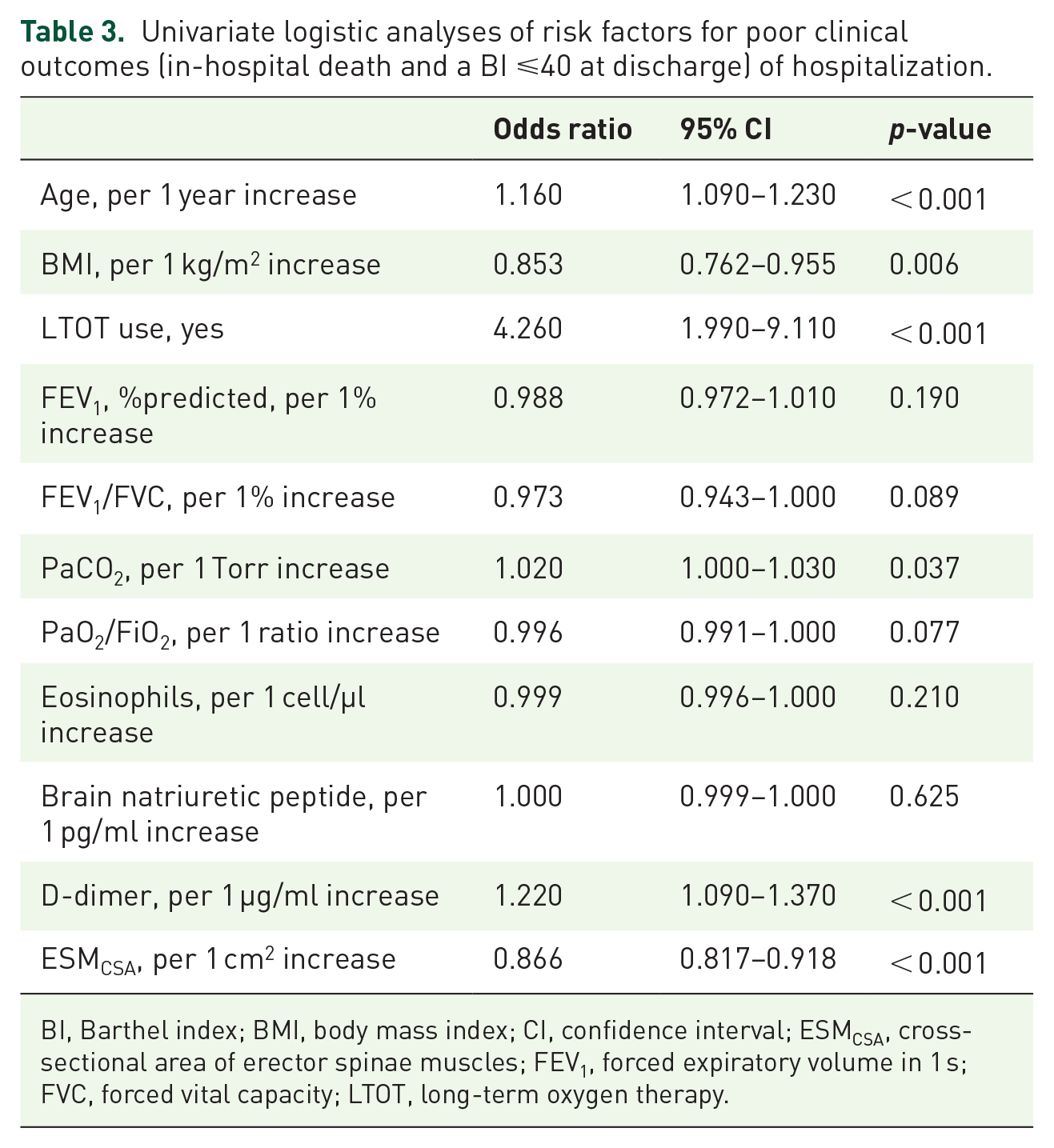
Univariate logistic regression analysis was performed to identify risk factors for poor clinical outcomes of hospitalization. Older age [odds ratio (OR) 1.160; p < 0.001], a lower BMI (OR 0.853; p = 0.006), more frequent use of LTOT (OR 4.260; p < 0.001), higher PaCO2 (OR 1.020; p = 0.037), a higher D-dimer concentration (OR 1.220; p < 0.001), and a lower ESMCSA (OR 0.866; p < 0.001) were significantly correlated with poor clinical outcomes of hospitalization (see Table 3).
Univariate logistic analyses of risk factors for poor clinical outcomes (in-hospital death and a BI ⩽40 at discharge) of hospitalization.
BI, Barthel index; BMI, body mass index; CI, confidence interval; ESMCSA, cross-sectional area of erector spinae muscles; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; LTOT, long-term oxygen therapy.
Multivariate logistic regression analyses were then performed (see Table 4). Two different models were analyzed. In model 1, we included age, LTOT use, PaCO2, D-dimer, and ESMCSA. Age [OR 1.100; 95% confidential interval (CI) 1.020–1.180; p = 0.012], LTOT use (OR 3.310; 95% CI 1.300–8.390; p = 0.012), D-dimer (OR 1.170; 95% CI 1.010–1.350; p = 0.033), and ESMCSA (OR 0.920; 95% CI 0.855–0.990; p = 0.025) were significantly associated with poor clinical outcomes of hospitalization [adjusted coefficient of determination (adjusted R2) = 0.24]. In model 2, we included BMI instead of ESMCSA. Age (OR 1.120; 95% CI 1.050–1.200; p < 0.001), LTOT use (OR 3.780; 95% CI 1.480–9.630; p = 0.005), and D-dimer concentration (OR 1.200; 95% CI 1.050–1.360; p = 0.008) were significantly associated with poor clinical outcomes of hospitalization (adjusted R2 = 0.24). However, BMI was not significantly correlated with poor inpatient outcomes of hospitalization (OR 0.868; 95% CI 0.745–1.010; p = 0.070).
Multivariate logistic analyses of risk factors for poor clinical outcomes (in-hospital death and a BI ⩽40 at discharge) of hospitalization.

BI, Barthel index; BMI, body mass index; CI, confidence interval; ESMCSA, cross-sectional area of erector spinae muscles; LTOT, long-term oxygen therapy.
Discussion
In this study, we focused on both death and low ability to perform ADL at discharge to evaluate clinical outcomes after hospitalization. The in-hospital mortality rate was 6.3%, and the proportion of poor clinical outcomes of hospitalization, including severe dependence when performing ADL at discharge, was 21.3%. Older age, LTOT use, a higher D-dimer concentration, and a lower ESMCSA on chest CT at admission were significantly associated with poor outcomes of hospitalization (in-hospital death and a BI ⩽40 at discharge) in patients with COPD exacerbation.
An exacerbation is a critical event in patients with COPD. Most patients with exacerbation improve in the ambulatory care setting, but some require hospitalization. COPD exacerbation–related hospitalization can lead to in-hospital death or readmission. Hospitalization is also a substantial socioeconomic problem.27,28 An excellent prognostic tool that can predict the outcome and guide clinical decision-making at the point of admission is urgently needed for clinical practice. Several useful predictors for hospitalized patients with COPD exacerbation have been reported, but they are mainly focused on death and readmission. The CURB65 score 15 and DECAF score 11 predict short-term mortality, and the CODEX score 16 and PEARL score 17 predict the combined outcome of death and readmission in hospitalized patients with COPD exacerbations.
In this study, we explored predictors of poor clinical outcomes (in-hospital death and a BI ⩽40 at discharge). A common sequela of COPD exacerbations is reduced physical activity, 5 which is an independent risk factor for readmission 29 and mortality. 13 A low ability to perform ADL is related to poor clinical outcomes after discharge, and we therefore considered it meaningful to assess both the ability to perform ADL and in-hospital death in this study. Overall, 31 (15.0%) patients had BI scores ⩽40 at discharge, which was regarded to reflect severe dependence when performing ADL. The BI is a widely used measurement tool to evaluate the ability to perform ADL and is recommended as a standardized assessment tool for older people. 30 A lower BI is associated with readmission, 31 disability, socioeconomic loss, 32 and mortality.31,33 Previous studies used a BI score ⩽40 as a cut-off point for the ability to perform ADL;34–37 we also adopted this cut-off. In one study, the rates of death and staying at long-term care facilities at 6 months after discharge were higher in patients with a BI ⩽40 at discharge. 25 Granger et al. 24 showed that patients with a BI ⩽40 had impaired mobility, and fewer than half of them were independent in very basic skills such as feeding, grooming, and bowel/bladder control.
In patients with COPD, muscle dysfunction progresses during exacerbations. 38 In particular, hospitalized patients with COPD exacerbation are markedly inactive during and after hospitalization, 5 and skeletal muscle strength is reduced during hospital admission. 39 It is well established that COPD exacerbations accelerate disease progression, and 20% of patients do not recover to their pre-exacerbation state. 12 Once COPD patients have become physically inactive, their mortality risk does not improve even if their activity level increases. 40 Therefore, maintenance of the ability to perform ADL and engage in physical activity is critical for hospitalized patients with COPD exacerbation. Predicting the ability to perform ADL at discharge is important for these patients.
This is the first study to assess the role of the ESMCSA in patients hospitalized for COPD exacerbation. In the multivariate logistic regression analyses, the ESMCSA was a significant predictive factor for poor clinical outcomes of hospitalization (in-hospital death and a BI ⩽40 at discharge), independent of age, LTOT use, PaCO2, and D-dimer concentration. Loss of skeletal muscle mass is an excellent predictor of mortality in patients with COPD, and the importance of skeletal muscle mass has been emphasized. 41 Of the skeletal muscles, the antigravity muscles, which maintain normal posture against gravity, are the most important muscles for performing ADL. 18 Recent advances in imaging techniques have enabled quantitative assessment of the antigravity muscles. The usefulness of analysis using the CT-derived ESMCSA, which reflects the number of antigravity muscles, has been reported in some respiratory diseases.19–21,26,42 A recent report showed that the ESMCSA was closely correlated with total body muscle mass. 43 Tanimura et al. 26 demonstrated that the ESMCSA was correlated with severe airflow limitations, respiratory symptoms, and emphysema severity, and was a strong risk factor for mortality in patients with stable COPD. Another study showed that, in the acute setting, a smaller ESMCSA on chest CT performed at admission was significantly associated with poor recovery of the ability to perform ADL in hospitalized patients with pneumonia. 44 Although frequent exacerbations were related to the ESMCSA-detected loss of antigravity muscles in patients with COPD, 45 the significance of the ESMCSA as a predictor in patients with COPD exacerbations remains unclear. This study showed that the ESMCSA was a significant predictor of poor clinical outcomes of hospitalization in patients with COPD exacerbation. Previous studies have revealed that the BMI is a useful prognostic factor in hospitalized patients with COPD exacerbation.9,46 In this study, the ESMCSA, but not the BMI, was a significant predictive factor in the multivariate logistic regression analyses. This result indicates that the ESMCSA is useful for predicting poor clinical outcomes of hospitalization (in-hospital death and a BI ⩽40 at discharge) in patients with COPD exacerbation.
The DECAF score has been used previously to predict mortality in hospitalized patients with COPD exacerbation. 11 When we included the DECAF score in two multivariate models, the ESMCSA was still a significant predictor of poor outcomes (Supplementary Table S1). This result suggests that the ESMCSA at admission contributed to poor clinical outcomes (in-hospital death and a BI ⩽40), independent of the intensity of the exacerbation event evaluated by the DECAF score. Therefore, the pre-exacerbation ESMCSA might determine the outcomes of hospitalized patients with COPD exacerbation. Rehabilitation reduces the annual decline in the ESMCSA 47 and leads to a shift away from physical frailty toward a more robust state. 48 Therefore, rehabilitation should be considered for COPD patients with physical frailty to maintain the ESMCSA and overcome the impact of exacerbation.
This study had several limitations. First, it was a retrospective single-center study, and prospective studies are needed to confirm its results. Although COPD exacerbations have been reported in large international clinical trials,49,50 considerable differences in the patients’ characteristics, such as age and general condition, exist between these studies and real-world practice. COPD exacerbation is an important problem, particularly in older populations. The in-hospital mortality rate was 6.3% in this study and the median patient age was 79 years, which is consistent with previous studies.9,11,51,52 Second, the ability to perform ADL, as assessed by BI before the exacerbation, was not evaluated because of the retrospective nature of the study. Patients with a modified Rankin Scale score ⩾4 before the exacerbations were excluded from this analysis. Furthermore, only the first exacerbation was analyzed because the physical activity level was worse after the exacerbation. 5 Third, chest CT is needed to evaluate the ESMCSA. In Japan, chest CT is usually performed on hospital admission to evaluate the disease severity and exclude other critical diseases in patients with COPD exacerbation requiring hospitalization. Therefore, ESMCSA data are available from the CT scan on admission. Fourth, the FiO2 is affected by a multitude of patient factors, including mouth breathing, degree of nasal congestion, respiratory rate, and minute volume. Although it is difficult to accurately calculate the FiO2, we estimated the FiO2 using validated formulae based on the volume of oxygen administered or the manufacturer’s instructions for conventional oxygen support devices, similar to previous literature.53,54
In conclusion, this observational study revealed that the rate of poor outcomes of hospitalization, including in-hospital death and a BI ⩽40 at discharge, was 21.3% in patients with COPD exacerbation requiring hospitalization. The ESMCSA obtained from chest CT on admission was a significant predictive factor for poor clinical outcomes of hospitalization, as were age, LTOT use, and the D-dimer concentration. The ESMCSA was superior to the BMI in the multivariate analyses. This result indicates that the ESMCSA is a good predictor of outcomes in patients with COPD exacerbations and might provide useful information for clinicians at the point of admission. Further research is needed to confirm this result in a prospective manner.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231172924 – Supplemental material for Predictors of poor clinical outcomes including in-hospital death and low ability to perform activities of daily living at discharge in hospitalized patients with chronic obstructive pulmonary disease exacerbation
Supplemental material, sj-docx-1-tar-10.1177_17534666231172924 for Predictors of poor clinical outcomes including in-hospital death and low ability to perform activities of daily living at discharge in hospitalized patients with chronic obstructive pulmonary disease exacerbation by Yurina Murakami, Hideki Yasui, Jun Sato, Tomohiro Uto, Naoki Inui, Takafumi Suda and Shiro Imokawa in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.