
Abstract
Introduction:
COVID-19 pandemic has challenged healthcare systems worldwide. The aim of this study was to assess the results of a Respiratory Telerehabilitation Program implemented to patients post-COVID-19 in postacute phase of mild to critical course of COVID-19 who had persistent respiratory symptoms and had not received any vaccination. The intervention was performed during confinement.
Methods:
A quasi-experimental nonrandomized study was conducted in Spain during confinement. Respiratory Telerehabilitation Program was guided by a specialized physical therapist through a web platform (Zoom by Zoom Video Communications, San Jose, CA, USA). Participants were recruited through social webs. Outcome measures included respiratory rate, heart rate, percutaneous oxygen saturation, Mahler’s Dyspnea Index, anxiety status, and quality of life [EuroQol 5 Dimension 5 (EQ-5D)].
Results:
A total number of 148 participants were recruited, with a final number of 100 participants completing the protocol (50 experimental group (EG)/50 control group (CG)). A total of 500 telerehabilitation sessions were performed for this study. In the EG, pre–post intervention comparative analysis showed significative changes in Mahler’s functional dyspnea (p < 0.001), the State-Trait Anxiety Inventory (p < 0.001), oxygen saturation (p < 0.001), heart rate (p < 0.001), quality-of-life questionnaire (p < 0.001), and respiratory rate (p < 0.001). Participants in the CG showed an improvement in all the variables, but the differences were not statistically significant except in Mahler’s functional dyspnea (p = 0.001) and in the quality-of-life questionnaire (p = 0.043). Percentage changes in pre–post intervention were calculated and compared between EG and CG. There were statistically significative differences in all the outcomes in favor of the EG.
Conclusion:
The implementation of a pulmonary telerehabilitation program for COVID-19 not vaccinated survivors in postacute phase with mild to critical course of COVID-19 with respiratory sequelae has proven its benefits in cardiorespiratory variables and dyspnea-related anxiety.
Introduction
At the beginning of the COVID-19 pandemic, it became clear that the work of the physiotherapist, traditionally linked to physical contact with the patient, needed to be reshaped to ensure the recovery of patients and, at the same time, to protect them against infection.
The use of telematics rehabilitation has been developing for some years. Telematics rehabilitation had already been used before the COVID-19 pandemic, demonstrating its value in rehabilitation of musculoskeletal diseases,1–3 in neurological 4 patients or in respiratory pathology, publishing promising experiences that allowed reaching a greater number of patients and improving the cost/efficiency of rehabilitation in patients with different respiratory diseases such as chronic obstructive pulmonary disease (COPD), interstitial lung disease, bronchiectasis, and respiratory dysfunction in neuromuscular diseases.5–7 During the emergency linked to the COVID-19 pandemic, remote assistance was increased, thus eliminating the barriers of distance, time, and potential contagion through telemedicine. 8
Symptoms associated with COVID-19 are very similar to those present in any respiratory viral infection, commonly cough (54.52%), fever (58.66%), dyspnea (30.82%), and fatigue (28.16%).9,10 Symptoms are usually mild, and the disease resolves within days, but in some cases, severe complications such as bilateral pneumonia make their appearance, usually initiated in the peripheric area of both lungs. In that patients, basal respiratory situation can get complicated, requiring their hospitalization in intensive respiratory care units due to acute respiratory distress and multiorgan failure. 11 The patients may present symptoms such as weakness, intolerance to aerobic exercise, respiratory distress and decreased quality of life that may last months after the infection.12–14
Rehabilitation of COVID-19 sequelae would depend on the severity of the symptoms, and a multidisciplinary approach is necessary. Respiratory Physical Therapy rehabilitation techniques are one of the core pillars for recovering lung function and stabilize the thoracic-lung system. Physical therapy techniques improve pulmonary functional capability and ventilation, reduce dyspnea, strengthen respiratory muscles, and facilitate adaptation to physical activity. 15 Patients may experience postviral fatigue. In order to control desaturation and fatigue, energy conservation techniques such as abdominal breathing and breathing exercises coordinated with arm movements are recommended. 16
Telerehabilitation in physical therapy brings the advantage of reaching a high number of patients with a minimum burden for healthcare systems, providing highly specialized services to populations that, due to physical, economical or purely geographical impediments, did not have access to professional respiratory rehabilitation care. 17
Methods
Design
A quasi-experimental, prospective, longitudinal nonrandomized study was conducted in April 2020. The protocol was approved by ethic committee from Hospital Alcorcón (Madrid, Spain), and was registered in ClinicalTrials.gov (NCT04678700). Informed consent was obtained from the patients prior to the study.
Procedure
Recruitment was conducted through social websites and COVID-19 patients associations. Respiratory Telerehabilitation Program was guided by a specialized physical therapy professional through a web platform (by Zoom Video Communications, San Jose, CA, USA), in live sessions. Participants were asked to connect themselves to the platform in groups of 20, three times a week, receiving a total number of 10 online sessions.
Patients were recruited and entered the 22 days program in order of arrival, in groups of 20, and the control group (CG) was composed by patients in the waiting list that were offered to receive the intervention later.
Sample size was determined by a pilot study involving the 20 first participants who accomplished the Respiratory Telerehabilitation Program, using Mahler’s Dyspnea Index (MDI) as main outcome measure. G*Power software was used for the calculation, assuming an alpha risk of 0.05 and power of 80%. The estimation, including a 20% loss estimation, was of 74 subjects per group.
Participants should meet the following inclusion criteria: patients who have signed the informed consent; with a COVID-19 medical diagnostic 18 ; in post-infection phase 19 ; 10 days from the last polymerase chain reaction (PCR) positive test 19 ; with dyspnea sensation 20 ; that are able to connect themselves to the web platform 21 ; that could maintain a sitting position for an hour and have access to a pulse oximeter for self-monitoring.
The exclusion criteria were as follows: patients in intensive care unit (ICU) or hemodynamically/respiratory unstable at the time of the study12,19; connected to mechanical ventilation 12 ; moderate to severe heart conditions (Grade III or IV, New York Heart Association) 18 ; with severe stroke or neurodegenerative disease 18 ; with a medical record of acute disease 6 months prior to the study; with cognitive impairment; receiving any other respiratory rehabilitation program.
Outcome measures
The following measures were taken: respiratory rate (RR), heart rate (HR), and percutaneous oxygen saturation (SpO2), measured with a pulse oximeter.
MDI was used to measure the functional dyspnea. An interview-administered scale for self-assessment of dyspnea was used, consisting of three subscales for measuring dyspnea-related functional alterations, task magnitude necessary to provoke dyspnea, and effort magnitude necessary to provoke dyspnea, rating from 0 (null) to 4 (maximum dyspnea). 22
Anxiety status was assessed through the State-Trait Anxiety Inventory (STAI) has 20 items for evaluating trait anxiety and 20 items for state anxiety. 23 Quality of life was assessed through the European Quality-of-Life Questionnaire, EuroQoL [EuroQol 5 Dimension 5 (EQ-5D)], which evaluates descriptively generic quality of life, including five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression).24,25
In order to maintain clinical safety limits, RR, HR, SpO2, and modified Borg scale were monitored at each session. Patients were asked to acquire a pulse oximeter to measure their SpO2 and to self-monitor during the sessions and were also trained in modified Borg scale. If the SpO2 value decreased by 4% and if it fell below 95% or registered an increase of three points with respect to the initial value of the modified Borg scale, the participant had to interrupt the session. Other reasons for interrupting the session were an increase in HR by 20 beats per minute, dizziness, sweating, headache, or chest pressure. 26
Intervention
Sessions were guided by an expert in Respiratory Physical Therapy, with more than 10 years of clinical experience. The program was based in SEPAR Respiratory Physical Therapy Guides 12 and the previous literature.18,27–29 Sessions included (a) abdominal-diaphragmatic breathing, (b) costal expansion exercises – flexion and abduction of upper limbs, (c) active cycle of breathing, (d) self-stretching of neck and thoracic muscles, (e) yoga-based respiratory exercises pranayama, (f) progressive muscular relaxation, and (g) mindfulness.
Statistical analysis
Only data from patients who had completed the protocol regularly and successfully were included. Frequency of the categorical variables was expressed as absolute number and as a percentage. Qualitative variables were expressed as median and interquartile range (IQR). Chi-square test was used for qualitative variables comparison. For quantitative variables, Mann–Whitney U test (baseline analysis) and Wilcoxon signed-rank test (pre–post analysis) were used. Statistical significance was set at p < 0.05 values. Effect size was calculated through biserial correlation coefficient (rbis). Percentual changes in EG and CG were also calculated. Software IBM SPSS Statistic for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA) was used for the data analysis.
Results
A total number of 148 subjects signed the informed consent document. The first 74 were assigned to the EG and the following 74 were inscribed in a waiting list and composed the CG. Data were collected only from participants who completed the 10 sessions 3 days per week regularly. Finally, with a loss percentage of 32%, 50 subjects of each group completed the protocol.
Table 1 shows the comparative analysis of the demographic and clinical characteristics reported by the patients in the CG and the EG before the start of the intervention. Patients in the CG reported significantly more frequent presence of cough (p = 0.027) than in the EG.
Clinical characteristics reported by the patients at the beginning of the study: experimental group and control group comparison.

ICU, intensive care unit.
Data correspond to median and interquartile range (IQR).
The median age of participants was 49 years (IQR = 38–55.75). The youngest participant was 22 years old and the oldest was 80 years old. A total of 69 were women (69%).
Baseline analysis
A test was carried out to check whether the subjects in the CG and EG had homogeneous characteristics at the beginning of the study. There were no significant differences in socio-demographic and anthropometric variables such as age (p = 0.622), sex (p = 0.829), and BMI (p = 0.26).
Regarding the comparison of the variables initially measured in the EG and the CG (Table 2), there were no significant differences in state anxiety (p = 0.307), Mahler’s functional dyspnea (p = 0.259), RR (p = 0.089), SpO2 (p = 0.891), and HR (p = 0.204). The median trait anxiety, however, was significantly higher in the CG initially (p = 0.026) and the score on the quality-of-life questionnaire was significantly higher in the EG (p = 0.038).
Variables measured at the start of the study: experimental group and control group comparison.

Data correspond to median and interquartile range (IQR).
Pre–post intervention comparative analysis
Pre–post comparative analyses in the EG and CG are shown in Tables 3 and 4. As shown in Table 3, participants in the CG showed an improvement in all the variables, but the differences were not statistically significant except in Mahler’s functional dyspnea (p = 0.001) and quality-of-life questionnaire (p = 0.043).
Pre–post comparison of control group.
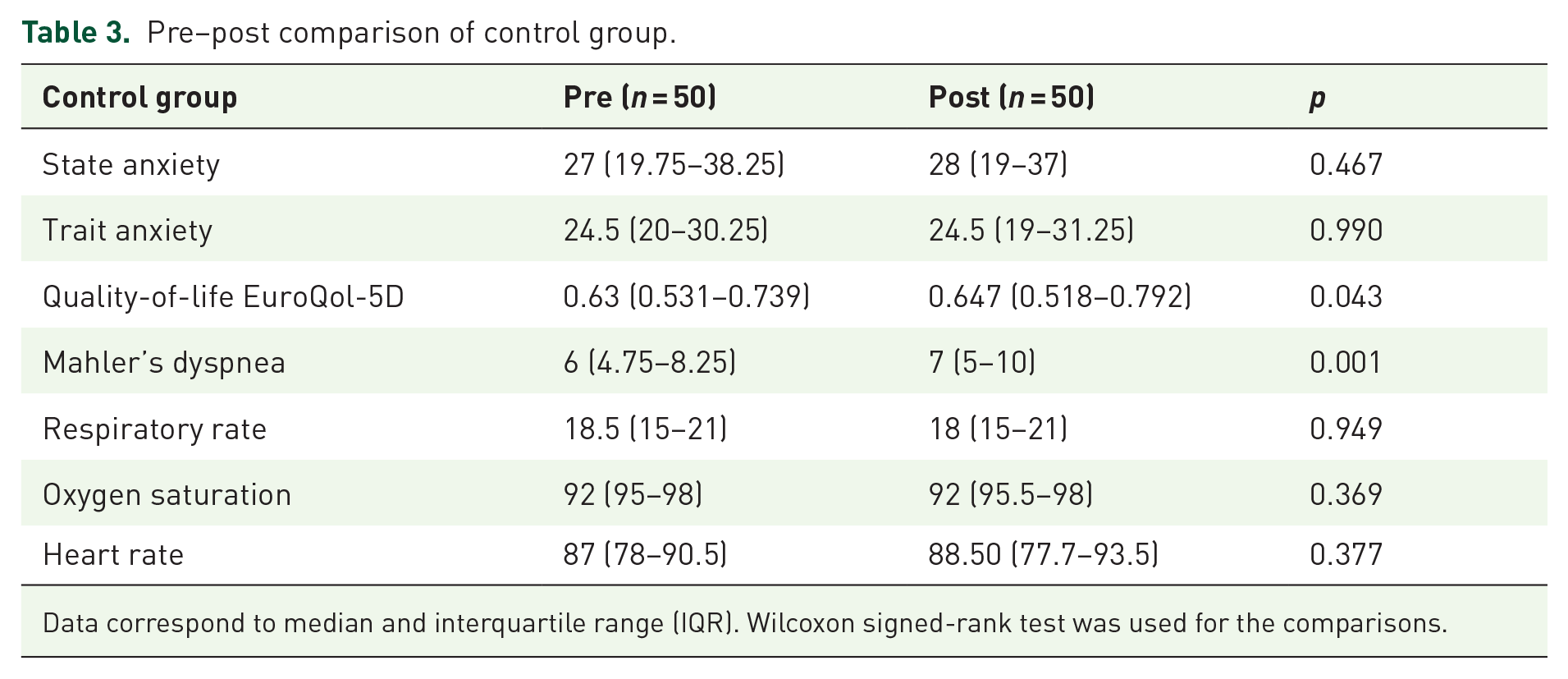
Data correspond to median and interquartile range (IQR). Wilcoxon signed-rank test was used for the comparisons.
Pre–post comparison of experimental group.

Data correspond to median and interquartile range (IQR). Wilcoxon signed-rank test was used for the comparisons.
Pre–post comparative analyses in EG are shown in Table 4. There were statistically significant improvements in all studied variables: state anxiety (p < 0.001), trait anxiety (p = 0.004), quality-of-life EuroQol-5D (p < 0.001), Mahler’s functional dyspnea (p < 0.001), RR (p < 0.001), SpO2 (p < 0.001), and HR (p < 0.001). Dyspnea rated from 7 to 10 points after the intervention.
Intervention effect size in the EG (Table 4) was calculated through rbis, showing a medium effect (0.3) for trait anxiety and a big effect (rbis > 0.5) for state anxiety, quality of life, RR, SpO2, HR, and dyspnea. Regarding dyspnea, although the medians in both groups showed improvement, in the CG rated from six to seven points and in the EG from seven to ten points.
Percentage changes in pre–post intervention were calculated and compared between groups. There were statistically significant differences in all the outcomes in favor of the EG, as showed in Table 5. The greatest percentage change occurred in RR, followed by dyspnea and quality of life. Percentage change in dyspnea had a median of 30.95% in the EG, whereas in the CG was of a 10%. In the CG, percentage change median was 0 for trait anxiety, state anxiety, quality of life, and SpO2.
Percentage change pre–post intervention in EG versus CG.

CG, control group; EG, experimental group.
Data correspond to median and interquartile range (IQR). Wilcoxon signed-rank test was used for the comparisons.
Discussion
Our results show that participants who completed the telerehabilitation program based on dyspnea control techniques and mindfulness statistically improved the variables of arterial blood oxygen saturation, RR, heart rate, dyspnea, anxiety, and quality of life.
The collapse of the health system generated by the pandemic has accelerated the revolution of the digital era in all domains, including health care. Telemedicine systems have increased rapidly in all specialties.8,30,31 The use of physiotherapy via video conference in patients with sequelae of COVID-19 has been recommended in most international guidelines.32–34
The conclusions drawn in the latest systematic review of respiratory telerehabilitation in patients with COVID-19 published in 2022 35 coincide with the results of this study; however, this review raises the need to assess the variables of anxiety and depression, which were evaluated in our study, As the program was designed to improve the variables of dyspnea, cardiac and pulmonary function, anxiety, and quality of life in patients with postacute respiratory problems of mild to critical course of COVID-19.
The program was conducted during confinement in Spain, when participants had not yet received any vaccine doses. Participants were confined in the first wave of the pandemic, with no possibility of geographical mobility, so variables were self-reported.
Given the limited mobility due to confinement, variables were collected using validated questionnaires, scales, and pulse oximetry. The EG participants improved the variables (RR, HR, SpO2, and RPE). Variables measuring exercise capacity such as 6 min walking test (6MWD), cardiorespiratory fitness (VO2 max), or spirometry could not be taken. While other studies using face-to-face pulmonary rehabilitation were able to measure, demonstrating good results.18,36
The patients in this study had not been vaccinated, so they were more affected. Along the same lines, another study carried out in patients without vaccination was that of Hermann et al., 19 which included dyspnea control techniques such as abdomino-diaphragmatic ventilation in hospitalized patients, with positive results. The respiratory physiotherapy program included different exercises with slow and controlled breathing. Several authors claim that these techniques increase the activity of the vagus nerve (parasympathetic nervous system), inducing relaxation, reducing stress, and dyspnea.37,38 Similar results were obtained in this program, obtaining statistically significant improvements in the variables anxiety and dyspnea. Although the results showed that dyspnea improved in both groups, it was greater in the EG (p = 0.000).
Many publications state that progressive muscle relaxation and mindfulness decrease anxiety, increase sleep quality, and produce parasympathetic activation.39–41 Both techniques performed telematically in this study and reduced anxiety levels and dyspnea, leading to a relaxation state.
Similar experiences have been published in the last years of the COVID-19 pandemic, such as a pulmonary rehabilitation program using smartphones and remote monitoring, which showed improvements in exercise capacity, lung function, quality of life, and dyspnea in the 59 patients who received rehabilitation. 42 Another study by a Spanish research group that based its program on muscle toning exercises in patients with COVID-19 with mild to moderate symptoms in the acute phase also carried out via live videoconference with a specialized physiotherapist 43 showed positive results, coincident with this study. The results demonstrate that the techniques used for dyspnea control and mindfulness were useful for improving post-COVID-19 patients through telerehabilitation, breaking the barriers of distance, and reaching a greater number of patients.
Conclusion
The implementation of a pulmonary telerehabilitation program for post-COVID-19 patients in postacute phase of mild to critical course, not vaccinated with respiratory sequelae has proven its benefits in the variables (RR, HR, SpO2, and RPE) and dyspnea and anxiety variables. Telemedicine provide adequate care for patients, transcending local healthcare systems’ limitations, social distance, and reaching remote environments with no easy access to this specialized attention.
Limitations
This study has limitations. The first limitation was that no disease stratification process was applied; postacute patients with mild to critical course were included. Another limitation was the choice of study variables; confined patients could not be moved to assess variables such as exercise capacity, which is widely recommended in telerehabilitation programs.