
Abstract
Background:
Severe coronavirus 2019 disease (COVID-19) causes acute hypoxemic respiratory failure requiring invasive mechanical ventilation (IMV). Once these symptoms are resolved, patients can present systemic deterioration.
Objective:
The two objectives of this study were as follows: to describe the results of a pulmonary rehabilitation program (PRP), which is divided into three groups with different numbers of sessions (12, 24, and 36), and to associate the variables of pulmonary function, exercise performance, and functionality with the number of sessions and functional improvement.
Design:
Prospective, observational study.
Methods:
PRP consisted of aerobic + strength + flexibility exercises under the supervision and individualized into 12, 24, or 36 sessions (12s, 24s, and 36s), depending on the evolution of each patient. At the beginning of the study and immediately after the intervention, forced vital capacity (FVC), maximal inspiratory pressure, 6-minute walk test (6MWT), sit-to-stand test (STS), maximal handgrip strength (HGS), Fatigue Assessment Scale, Post-COVID-19 Functional Status (PCFS), and health-related quality of life (HRQoL) were measured.
Results:
The proposed PRP demonstrated a positive effect on pulmonary function, exercise performance, and HRQoL, regardless of the number of sessions. A higher score on the PCFS and more days on IMV were associated with the increased likelihood of needing more sessions, whereas more meters on the 6MWT in the initial evaluation was associated with a reduced likelihood of needing more sessions. Finally, more repetitions on the STS and less distance covered on the initial 6MWT were associated with a greater improvement in exercise performance evaluated with the 6MWT.
Conclusion:
Supervised and individualized PRP for patients with severe post-COVID-19 improves pulmonary function, exercise performance, functionality, and quality of life. Functionality, distance covered on the 6MWT, and the days on IMV are central to the scheduling of the number of sessions for these patients.
Introduction
The severity of the symptoms of coronavirus 2019 disease (COVID-19) caused by the severe acute respiratory syndrome (SARS)-CoV-2 virus can be very heterogeneous. Most subjects develop a mild disease, without complications. However, 14% of patients develop a moderate disease that requires hospitalization, and 5% present a SARS requiring treatment in the intensive care unit (ICU). 1
One of the main complications of COVID-19 is acute hypoxemic respiratory failure. This requires prolonged hospitalization in an ICU on invasive mechanical ventilation (IMV), 2 which can last several days. 3 After hospital discharge, the patients present symptoms for up to 2 months due to the ICU stay and the use of IMV. 4 The most frequent symptoms are dyspnea and fatigue. 5 In this light, the implementation of a pulmonary rehabilitation program (PRP) is recommended.6–8
Due to the lockdown during the COVID-19 pandemic, new PRP delivery strategies gained momentum. Tele-rehabilitation programs have shown positive results. 9 However, this intervention modality presents limitations when the aerobic capacity and functionality of each individual are examined in depth. 10 The latter acquires relevance in individuals with greater functional compromise 11 since they must receive a PRP that considers their individual characteristics.
The PRP must consider the physiological parameters of each individual2,5,6 to be customized and supervised. In addition, it is worth noting that a PRP must take special care in the duration, intensity, frequency, and specificity of the exercise 12 ; this is currently known as a ‘patient-tailored’ PRP.13,14 To achieve this, an initial evaluation is required that includes several tests such as pulmonary function, aerobic capacity, and stress tests for individual thresholds.2,5,6,13,15,16
In this respect, the data on the structure, duration, effect, and safety of PRP are still being collected. Considering the current COVID-19 situation and given the impossibility of waiting for randomized controlled tests, 12 it is necessary to systematize the interventions regarding their duration and structure to then assess their effects. With respect to the duration of the PRP, the existing information indicates an average of between 6 and 8 weeks. 14 However, patients with systemic inflammation as a result of COVID-19 and a prolonged hospital stay generate a greater functional deficit.13,14 This could increase rehabilitation times. Consequently, the primary objective of this study was to describe the results of a PRP, which is divided into three groups with different numbers of sessions (12, 24, and 36) and, second, to associate variables of pulmonary function, exercise performance, and functionality with the number of sessions and functional improvement.
Methods
Participants
In all, 132 patients were included in this observational study. The sampling was non-probabilistic and consecutive. The study took place between September 2020 and September 2021. This study was approved by the Scientific Ethics Committee of the Central Metropolitan Health Service, Chile (Resolution N° 378/2021). This project has previous publications that provide preliminary results or secondary analyses.8,16,17 All the participants were informed about the procedures of this study, agreed to participate, and gave written consent. The inclusion criteria were as follows: (a) COVID-19 diagnosis, (b) required IMV, (c) medical hospital discharge, (d) check-up with a medical cardiologist and normal electrocardiogram, and (e) check-up with a bronchopulmonary specialist. Patients with a diagnosis of chronic respiratory disease and who do not understand and/or follow orders were excluded. Patients were evaluated prior to beginning the PRP (Pre) and when it was finished (Post).
When the PRP was finished, the patients were distributed into three different groups according to the number of sessions: 12s Group (12 sessions), 24s Group (24 sessions), and 36s Group (36 sessions). For this, the ability to walk continuously for 30 min on a treadmill was evaluated at the end of 12 sessions; if the patient achieved it, this ended their PRP. If this did not happen, the patient had to continue until the end of 24 sessions where they were re-evaluated and, according to the same criterion, the decision was made if the patient ended their PRP or continued up to 36 sessions (Figure 1). The sample size was carried out according to the study by Gloeckl et al. 5 a post hoc power calculation was done using the G*Power 3.1.9.7 software. Based on the mean and standard deviation of the improvements in the primary outcome (6MWT), the Cohen’s d effect sizes were calculated: 1.54 for the 12s group, 1.10 for the 24s group, and 1.58 for the 36s group. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.

Flow diagram for participant enrollment, evaluation, and intervention.6MWT, 6-minute walking test; FAS, Fatigue Assessment Scale; FVC, forced vital capacity; HGS, maximal handgrip strength; HRQoL, health-related quality of life; MIP, maximal inspiratory pressure; PCFS, Post-COVID-19 Functional Status; STS, sit-to-stand test.
Measurements and instruments
Spirometry and Maximal inspiratory pressure (MIP): For spirometry, we used a Medgraphics spirometer (CPFS/D USB 2.02, MGC Diagnostics Corporation, St Paul, MN, USA), the measurement was standardized according to the ERS/ATS standards. 18 The MIP measurement was standardized according to the ERS/ATS standards. For this, we used a differential pressure gauge (PCE-P01/PCE-P05®, PCE Ibérica S.L. Albacete, Spain). 19
Exercise Performance: Aerobic capacity was measured with the 6-minute walk test (6MWT). 20 Lower limb strength was assessed with the STS. 21 Finally, maximal handgrip strength (HGS) was measured with a hydraulic dynamometer (Jamar®, St. Louis, MO, USA). 22
Fatigue, Functional Status, and Dyspnea: Fatigue was measured with the Fatigue Assessment Scale (FAS). 23 Functional status was measured with the Post-COVID-19 Functional Status (PCFS). 24 Dyspnea was categorized with a modified Borg scale (0–10 points) 25 and modified Medical Research Council (0–4). 26
Health-related quality of life: Health-related quality of life (HRQoL) was evaluated using Version 2 of the Short-Form 36 Health Survey (SF-36) questionnaire. The SF-36 has been adapted syntactically and semantically for the Chilean population.27,28
Intervention
Pulmonary Rehabilitation Program: The sessions (2×/week) were divided into 30 min of aerobic exercise, 20 min of strength exercise, and 10 min of flexibility consisting of muscle stretching. The training session was stopped when the participant presented one of the following criteria: dyspnea or fatigue⩾7 points (of 10), a pulse saturometry <91%, or exceeded 80% of their heart rate reserve. 17 In addition, the inspiratory muscle strength training was done in the home of each patient (2× per day for 5×/week). The PRP is detailed in a previous publication.8,17
Statistical analysis
Since most of the variables presented a non-normal distribution, for parsimony it was decided to present the data according to median, and lower and upper limits of the interquartile range. The qualitative data are presented in absolute and relative frequencies.
An intragroup analysis was done using the Wilcoxon test. To estimate initial intergroup differences, the Kruskal–Wallis test was used as an omnibus analysis. When the p value was <0.05, a post hoc analysis was done using the Mann–Whitney U test, considering the Bonferroni correction. This same analysis was used to examine the significant differences in the deltas (post-intervention minus pre-intervention) of the quantitative variables among the groups.
The association between the groups and baseline clinical evaluations was explored using an ordinal logistic regression. They were examined as confounding variables, age, sex, and body mass index (BMI). In addition, the association between the delta in 6MWT (6MWT post-intervention less 6MWT pre-intervention) and the baseline clinical evaluations was explored using a multiple linear regression model. The significance level was established at p < 0.05 with a 95% confidence interval for the statistical estimations. The statistical analysis was done with the STATA statistics program (StataCorp.Stata Statistical Software, College Station, TX: StataCorp.LP, USA). (version 14).
Data availability
The data associated with the paper are not publicly available but are available from the corresponding author on reasonable request.
Results
Baseline characteristics
Figure 1 indicates the distribution of the groups. The baseline characteristics of the individuals according to group (12s, 24s, and 36s) are provided in Table 1. At baseline, there are no differences among the groups with the exception of the days of hospitalization and the days on IMV, in both variables the 36s group presented more days than the 12s group.
Baseline characteristics of the participants.
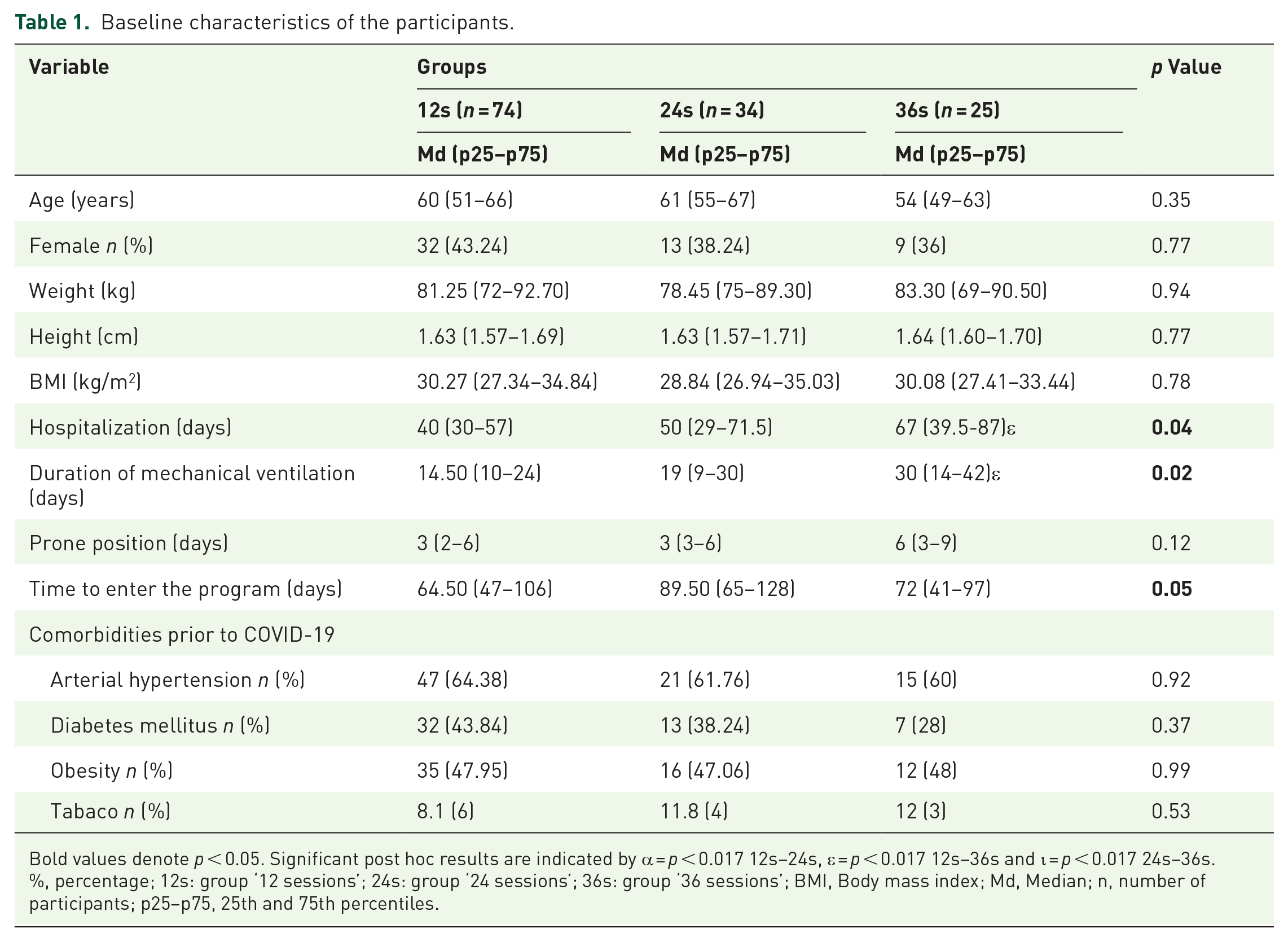
Bold values denote p < 0.05. Significant post hoc results are indicated by α = p < 0.017 12s–24s, ε = p < 0.017 12s–36s and ι = p < 0.017 24s–36s.
%, percentage; 12s: group ‘12 sessions’; 24s: group ‘24 sessions’; 36s: group ‘36 sessions’; BMI, Body mass index; Md, Median; n, number of participants; p25–p75, 25th and 75th percentiles.
Intragroup pulmonary rehabilitation
The analysis of the deltas (post-intervention minus pre-intervention) among the groups showed differences between the variables FEV1/FVC, 6MWT m, 6MWT % predicted (pred), STS, Borg-dyspnea, and HRQoL (PF and BP; Tables 2 and 3).
Outcomes of a program pulmonary rehabilitation program in 133 post-severe COVID-19 patients in spirometry, maximal inspiratory pressure, exercise performance, fatigue, functional status, and dyspnea.

Bold values denote p < 0.05 intergroups. Significant post hoc results (i.e. p < 0.017) are indicated by: α for 12s–24s, ε for 12s–36s, and ι for 24s–36s.
Denote p < 0.05 in the comparison Pre and Post the intervention in the groups.
6-minute walk test; 12s, group ‘12 sessions’; 24s, group ‘24 sessions’; 36s, group ‘36 sessions’; Borg, modified Borg scale; cmH2O, centimeters of water; FAS, Fatigue Assessment Scale; FEV1, the volume that has been exhaled at the end of the first second of forced expiration; FVC, forced vital capacity; HGS, hand-grip strength; Md, median; MIP, maximum inspiratory pressure; mMRC, modified Medical Research Council; n, number of participants; p25–p75, 25th and 75th percentiles; PCFS, Post-COVID-19 Functional Status; Pre, before the pulmonary rehabilitation program; Post, after the pulmonary rehabilitation program; STS, sit-to-stand test.
Outcomes of a program pulmonary rehabilitation program in 133 post-severe COVID-19 patients in health-related quality of life.
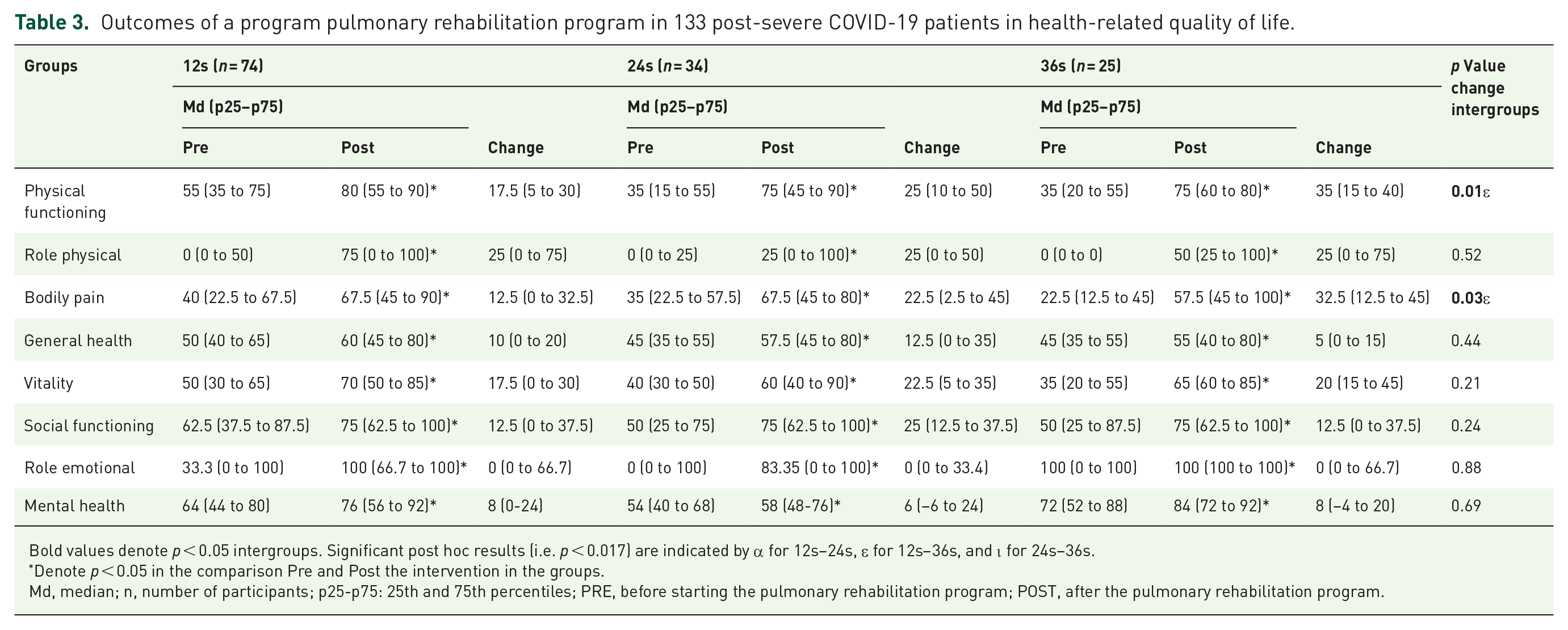
Bold values denote p < 0.05 intergroups. Significant post hoc results (i.e. p < 0.017) are indicated by α for 12s–24s, ε for 12s–36s, and ι for 24s–36s.
Denote p < 0.05 in the comparison Pre and Post the intervention in the groups.
Md, median; n, number of participants; p25-p75: 25th and 75th percentiles; PRE, before starting the pulmonary rehabilitation program; POST, after the pulmonary rehabilitation program.
The PRP improved all the variables in the post-intervention assessment in the three groups, showing significant differences (all p < 0.05; intragroup analysis).
Intergroup pulmonary rehabilitation
When examining the initial evaluation, it is noted that the groups differ in FVC L predicted (36s > 12s, p = 0.01), FEV1 L predicted (36s > 12s, p = 0.004), 6MWT meters (24s > 12s, p = 0.001; 36s > 12s, p < 0.001), 6MWT % predicted (24s > 12s, p = 0.006; 36s > 12s, p < 0.001), STS (24s > 12s, p = 0.001; 36s > 12s, p = 0.001), total FAS (24s > 12s, p = 0.008), mental FAS (24s > 12s, p = 0.01), PCFS (24s > 12s, p = 0.002; 36s > 12s, p < 0.001), PF (24s > 12s, p = 0.003; 36s > 12s, p = 0.004), and BP (36s > 12s, p = 0.015; these last two from the SF-36). Not so in FVC, FEV1, FEV1/FVC, MIP, HGS, physical FAS, mMRC, and in HRQoL (PR, GH, VT, SF, ER, and MH; Table 2).
The results of the ordinal logistic regression suggest that belonging to the groups was associated with the initial evaluation of the PCFS, days on IMV, and distance covered on the 6MWT. Thus, for PCFS 3 and 4, the odds of belonging to the 36s group versus the combined 24s and 12s are 5.54 and 8.55 times greater, respectively, given the other variables are held constant in the model. For a 1-day increase in IMV, the odds of belonging to group 36s versus the combined 24s and 12s are 1.03 times greater (other variables constant). Finally, for each additional meter on the initial 6MWT, the odds of belonging to group 36s versus the combined 24s and 12s decrease by 0.6% (other variables constant; Table 4). In addition, the variables such as sex, age, and BMI did not modify the predictor variables, nor were they significant.
Ordinal logistic regression for the group.

Bold values denote p < 0.05.
6MWT, 6-minute walk test; 95% CI, 95% confidence interval; IMV, invasive mechanical ventilation; LL, lower limit; PCFS, Post-COVID-19 Functional Status; Pre, before the pulmonary rehabilitation program; OR, odds ratio; SE, standard error; UL, upper limit.
The analysis of several simple linear regressions suggests that the initial variables such as age, sex, group (12s, 24s, 36s), BMI, FVC, FEV1, MIP, 6MWT, STS, HGS, PCFS, mMRC, Borg-dyspnea, days of hospitalization, days on IMV, and days prone are associated independently with the improvement on the 6MWT (Table 5).
Singles regression lineal for improvement in 6-minute walk test.

Bold values denote p < 0.05.
6MWT, 6-minute walk test; 95% CI, 95% confidence interval; B, unstandardized beta coefficients; BMI, body mass index; FEV1, volume that has been exhaled at the end of the first second of forced expiration; FVC, forced vital capacity; HGS, hand-grip strength; LL, lower limit; MIP, maximum inspiratory pressure; MV, mechanical ventilation; PCFS, Post-COVID-19 Functional Status; SE, standard error; STS, sit-to-stand test; UL, upper limit.
The exploration of various models revealed that the multiple linear regression model that best predicts (explained variability of 42.7%) the improvement on the 6MWT is the one that includes the initial 6MWT and the initial STS. Diabetes mellitus (DM) proved to be a modifier of the effect for the initial 6MWT, but not for the STS. This means it is noted that the effect of the meters on the 6MWT is better at predicting the improvement in the 6MWT in individuals without DM (−0.58 m) than in people with DM (−0.45 m), in both cases significant. Thus, for every additional meter covered on the initial 6MWT, the improvement in this same test at the end of the intervention decreases by 0.58 m in individuals without DM and 0.45 in individuals with DM as with the performance on the STS. With respect to the STS, for every time, an individual managed to stand and sit, the improvement on the 6MWT increased 3.12 m as with the meters on the initial 6MWT. It is worth noting that the origin ordinates were different (constant) and that the constant from which it started was lower in the group with DM (200.27 m) than in the group without diabetes (290.58 m; Table 6).
Multiple linear regression for improvement in 6-minute walk test.

Bold values denote p < 0.05.
6MWT, 6-minute walk test; 95% CI, 95% confidence interval; B: unstandardized beta coefficients; DM, diabetes mellitus; LL: lower limit; Pre, before the pulmonary rehabilitation program; SE: standard error; STS, sit-to-stand test; UL, upper limit.
Discussion
The aim of this study was to describe the results of an individualized and supervised PRP for patients with severe post-COVID-19 and its relation to the number of sessions. The PRP increased pulmonary function and exercise performance, reduced the physical, mental, and total FAS, and improved the HRQoL in all the groups (12s, 24s, and 36s). Belonging to the groups with the most sessions was associated with a lower Pre-functional status, more days on IMV, and less aerobic capacity. Finally, the improvement in the 6MWT was associated with greater strength in the lower limbs and less aerobic capacity.
In relation to the structure of the PRP,5,29,30 there are various forms described in the literature; however, these maintain a multimodal training (aerobic + strength + flexibility). In greater detail on the PRP performed with patients with post-COVID-19, Gloeckl et al. used aerobic training on a cycloergometer from 10 to 20 min with a maximum work rate between 60% and 70% added to ~30 min of strength training, all this with a frequency of 5 days/week (3 weeks). 5 By contrast, Spielmanns et al. scheduled the training through the initial distance covered on the 6MWT. The patients with a distance <200 m did aerobic exercise on a cycloergometer for 5–10 min to reach 35 min added to strength exercises, 5–6 days/week, for 25–30 sessions. In the case of patients with a distance >200 m on the 6MWT, they did a program of aerobic exercise on a cycloergometer and/or treadmill where the training load was 80% of the speed of the 6MWT plus strength training, with the same frequency as the previous group. 29 Unlike the previously described studies, aerobic training in the present study was only done on a treadmill. In this context, it is important to emphasize that (i) walking-based aerobic training has a high functional component, (ii) the strategy of the interval enabled all patients to reach 30 min of training, (iii) the load was reprogrammed weekly, and (iv) three different discharge points were considered, at 12s, 24s, and 36s (Tables 2 and 4).
The PRP implemented in this study was with the use of a treadmill for all the patients. Although the use of a cycloergometer is common and has evidence,5,30 we suggest that treadmill-based training has the benefit of strengthening walking, this being relevant given the existing relation between walking, functionality, and the accomplishment of basic daily life activities. 31 In addition to this, treadmill training has already been shown to reduce dyspnea and impact the daily life activities of patients with chronic obstructive pulmonary disease (COPD). 32
In this context, we must be aware of two important points in relation to the initial performance of the 6MWT of the study sample. First, it was below 500 m, agreeing with Huang et al., who reported a median of 495 m on the 6MWT in patients with post-COVID-19 at 6 months from hospital discharge. 33 Second, the patients are below the limit of ‘normality’ proposed by Hussain et al. if we consider the distance on the 6MWT as an indicator of functional limitation, 34 which is why the increase in the distance covered may be related to the proposed PRP and its personalization in the number of sessions. In this regard, the results of the present study indicate that patients with more days on IMV and less functionality and distance covered increased their likelihood of doing more sessions (i.e. 36s). By contrast, covering a greater distance on the 6MWT reduced the probability of having more sessions, a situation that is consistent with Gloeckl et al., who indicate that a higher baseline leads to a certain ceiling effect that limits the possibilities of improving the 6MWD after PRP 34 (Table 4).
Patients with a score of four points in PCFS were 8.55 times more likely to need 36 sessions compared to the rest (Table 4). This result could point to the PCFS as an important instrument when evaluating patients with severe post-COVID-19. Since it is a low-cost, simple, and fast instrument that is easy to understand, its incorporation into the routine evaluation would be of great value. However, the scale is not validated for COVID-19. 24 The results of the present study can be interpreted as an advance on this topic, given the described association. However, further research is needed on this instrument and its psychometric properties to be able to consolidate its use.
Another result of this study was the impact of exercise performance on the distance covered on the 6MWT. A greater magnitude in the improvement of the distance covered on the 6MWT was predicted by a better performance on the initial STS and by a poorer performance on the initial evaluation of the 6MWT. This deterioration could be explained by the reduction in skeletal muscle mass in the lower limbs due to the strict isolation and reduced mobility of the patient during hospitalization. 35 Results in patients with COPD have demonstrated that the 6MWT and the STS are reliable clinical tests to measure aerobic capacity and muscle strength, respectively. A positive correlation has been reported between the meters walked on the 6MWT and the number of times on the STS (r = 0.47; p = 0.001) 36 and in patients with COPD (r = 0.716; p < 0.001) 37 . In this sense, the strength gained in the lower limbs due to the training implemented in the present study increased the number of repetitions on the STS and was complemented with the treadmill training for the increase in meters on the 6MWT.
DM modified the effect of this association, with the magnitude of this being greater in patients without DM. Unlike the previously mentioned studies,9,13,29,30 the percentage of DM in the study sample on average exceeded 30%. Although the relationship between DM and COVID-19 is in development,37,38 its impact after hospitalization remains unknown.38,39 However, in the absence of COVID-19, DM causes a loss of skeletal muscle mass that patients with DM present per se added to the altered muscle metabolism,40,41 which causes greater muscle fatigue, dyspnea, and less production of muscle strength that will lead to a reduction in physical performance. 42
There is varied information available on the duration of a PRP. In Germany and other European countries, 3 weeks has been established for the PRP. 34 In addition to the 3 weeks, the authors emphasize the number of sessions (mean = 24 ± 5 days) 29 that range from 25 to 30. 30 Our study considered the patient-tailored concept for the implementation of the PRP, including the number of sessions, because the variability of sequelae from COVID-19 makes it necessary to adjust the PRP to the needs of each individual, including personalizing the number of sessions.
On the other hand, the suggestions in relation to the PRP indicate that, in addition to doing physical exercise, there is attention paid to the psychological aspects and HRQoL5,6,12,42 of the discharged patients with COVID-19, especially women and older adults. 42 In this context, the results of the present study showed a significant increase in the HRQoL after PRP in the three intervention groups. This situation partially agrees with the report by Gloeckl et al., who managed to significantly improve the HRQoL in patients with severe/critical COVID-19 on the total score of the mental component of the SF-36 (from 38.5 to 52.9 points; p < 0.001). 5
This study has some limitations: (1) the non-inclusion of a control group could have caused possible selection bias and (2) the redistribution of resources to the closed healthcare system had a bearing on the time of admission to the PRP.
Conclusion
The supervised and individualized PRP for patients with severe post-COVID-19 improves pulmonary function, exercise performance, functionality, and HRQoL. The PCFS, days on IMV, and the distance covered on the 6MWT were associated with the number of sessions. In addition, our data suggest STS was associated with the improvement in the 6MWT.