
Abstract
Background:
We examined the responsiveness of the Manchester Chronic Obstructive Pulmonary Disease (COPD) Fatigue Scale (MCFS) in patients with COPD following 8 weeks of pulmonary rehabilitation (PR).
Methods:
Patients (n = 273) with clinically stable COPD completed 8 weeks of outpatient multidisciplinary PR, comprising 2 h (1 h exercise and 1 h education) weekly. Anxiety, exercise capacity, quality of life, dyspnea, fatigue were measured pre- and post-PR, utilizing the Anxiety Inventory for Respiratory Disease (AIR), Incremental Shuttle Walk Test (ISWT), St. George’s Respiratory Questionnaire (SGRQ), and modified Medical Research Council (mMRC) scale and MCFS, respectively.
Results:
The mean (SD) age of participants was 72 (8) years, and 50% were women. Total MCFS score fell after PR mean (95% confidence interval) −4.89 (–7.90 to −3.79) as did domain scores: physical −1.89 (–2.33 to −1.46), cognition −1.37 (–1.65 to −1.09), and psychosocial −1.62 (–2.00 to −1.62). Total MCFS effect size (ES) was 0.55; and for domains, physical was 0.52, cognition was 0.59, and psychosocial was 0.51. The ES for AIR was 0.30, mMRC was 0.38, SGRQ was 0.66, and ISWT was 1.19. MCFS changes correlated with changes in both SGRQ (p < 0.002) and AIR (p < 0.004), but not ISWT (p = 0.30) or mMRC (p = 0.18). The AIR, SGRQ, mMRC, and ISWT all improved after PR (all, p < 0.001).
Conclusion:
The MCFS scale is a valid and responsive scale to measure fatigue in patients with COPD after pulmonary rehabilitation.
Introduction
Chronic obstructive pulmonary disease (COPD) causes substantial disability and mortality in old age. In 2015, 174 million people lived with a COPD diagnosis worldwide. 1 Most COPD patients experience one or more troublesome symptoms such as pain, dyspnea on exertion, excessive fatigue, and decreased exercise tolerance, anxiety, and depression in their daily activities.2,3
Fatigue commonly coexists in COPD, with prevalence estimates ranging from 39% to 77%.2,4 The wide prevalence estimates for fatigue might be due to sampling methods, severity of illness, or the clinical recruitment setting (e.g. inpatient, outpatient, or community). Untreated fatigue is associated with decreased physical functioning, impaired quality of life (QoL), systemic inflammation symptoms, depression, and anxiety, and increased mortality in patients with COPD.5–7 Few generic well-validated generic fatigue scales have been adopted to measure fatigue in patients with COPD.7,8 The Manchester COPD Fatigue Scale (MCFS) is a disease-specific, valid, and reliable scale to measure fatigue in patients with COPD. 9 The MCFS self-reported, 27-item scale incorporates domains of physical (11 items), cognitive (7 items), and psychosocial (9 items) dimensions to quantify the fatigue level. 9
Pulmonary rehabilitation (PR) improves exercise capacity and QoL in patients with COPD. The efficacy of PR in alleviating fatigue in patients with COPD was inconclusive. This is partly due to lack of sensitive, disease-specific fatigue scales. To date, no studies have examined the efficacy of the MCFS scale in PR. Therefore, accurate assessment of fatigue may aid therapists in devising and instructing individualized or group exercise programs in PR. We examined the responsiveness of the MCFS to PR in patients with COPD. Furthermore, we evaluated the relationship of MCFS to clinically relevant outcomes following PR.
Methods
Other data from these participants have been reported previously. 10 Briefly, we conducted a prospective an 8 week PR program for patients with COPD in a community care setting. Eligible patients were at least 40 years old, with a primary diagnosis of clinically stable COPD and a forced expiratory volume in 1 s (FEV1) <70% predicted. We excluded patients with active lung cancer, preexisting preconditions potentially rendering exercise unsafe (e.g. unstable cardiac disease), and known psychiatric illness (e.g. schizophrenia). All patients gave written informed consent, and the local research ethics committee of the Blackpool Teaching Foundation National Health Service Trust (Ref: SE/0390) approved the study.
Outcome measures
The 27-item MCFS is a valid and reliable scale, with domains of physical, cognitive, and psychosocial fatigue in patients with COPD. 9 The self-administered tool probes the level of fatigue in the past 2 weeks. The total score ranges from 0 to 54; with the higher score corresponds with worse fatigue score. The MCFS tool is available at: 9 https://thorax.bmj.com/content/64/11/950#supplementary-materials
We measured health status, anxiety, dyspnea, and exercise capacity using the St. George’s Respiratory Questionnaire (SGRQ), Anxiety Inventory for Respiratory Disease (AIR), modified Medical Research Council scale (mMRC), and Incremental Shuttle Walk Test (ISWT), respectively.10–14 The ISWT is a reliable and valid scale in measuring exercise capacity following a PR program.13–16 We employed the adapted five-point Global Rating of Change Questionnaire (GRCQ) for patients to rate their health status after PR and masked to their performance. 15 They rated their health status, how they felt after PR using the GRCQ: ‘1: much better’; ‘2: a little better’; ‘3: no change’; ‘4: a little worse’; and ‘5: much worse’. We expressed FEV1 as percentage of predicted.
Intervention
PR comprised 8 weeks of supervised exercise training sessions. Each weekly session included 1 h of strengthening and endurance aerobic exercises and 1 h of education. Group aerobic exercise included functional, strengthening, and flexibility exercises; walking, cycling, and step-ups; and arm exercises using dumbbells. Each group session had 6–12 patients. Exercise sessions started with warm-up exercise for 5 min, followed by six aerobic exercise stations alternating between arm and leg activities, and finished with a 5 min cool down period. Patients were also encouraged to perform at least 30 min of walking at home daily, as an unsupervised endurance exercise. The group educational seminar discussed nutrition, oxygen and other medications, inhaler techniques, anxiety, panic management, and relaxation. We defined completers as attending >75% of the designated PR sessions and returning for the 8 week follow-up evaluation. 16
Statistical analysis
Descriptive statistics were calculated as frequencies and percentages, expressed as mean (standard deviation). Normal distribution was assessed by Kolmogorov–Smirnov test. Pearson correlations examined the relationship of demographics, clinical characteristics, and current symptoms to baseline fatigue level in patients with COPD. We have established the significance of the relationship as very weak <0.20, weak correlation (0.20–0.40), moderate correlation (0.40–0.60), strong correlation (0.60–0.80), and very strong correlation (0.80–1.00), respectively. 17 The internal consistency for the Cronbach’s alpha coefficients for the total MCFS was 0.97, and subdomains were 0.94 for physical component, 0.92 for cognition component, and 0.95 for psychosocial component, respectively. 9 The test–retest repeatabilities for the intraclass correlation coefficient (r1) were as follows: total MCFS, r1 = 0.97; and domains were physical, r1 = 0.96; cognitive, r1 = 0.91; and psychosocial, r = 0.95, accordingly. 9
Paired t tests examined differences before and after PR. The 95% confidence intervals were calculated for mean group changes in outcome measures after PR. The effect size (ES, defined as mean change/standard deviation of data collected at the baseline and at the end of 8 week) was calculated for each variable, and described as small (0.2), medium (0.5), or large (0.8) as suggested by Cohen. 18 The improvement was expressed as a percentage reduction from the baseline MCFS score, to quantify the magnitude of change following PR. We defined internal responsiveness as the ability of the MCFS to change over an 8 week PR. External responsiveness is the extent to which the changes in MCFS relates to corresponding change to clinical relevant severity markers in patients with COPD after an 8 week PR.
Linear regression analysis was performed to examine factors that predict change in fatigue score after PR. All statistical analyses were performed using the Statistical Package for the Social Sciences (Windows Version 25.0, IBM Corporation, Armonk, NY) software, with significance set at p < 0.05.
Results
Out of 352 enrolled patients, 273 (78%) completed PR, with a mean age of 72.0 ± 8.9 years and percentage predicted FEV1 of 59% (12). Half were women, and Table 1 shows baseline characteristics. Figure 1 shows a histogram of MCFS total scores for the study population. There was a wide range of MCFS fatigue that followed a distribution that was approximately normal. However, there was a little evidence of flooring and ceiling effects of MCFS, while a few of the patients had either a score of zero (no fatigue score, n = 5) or 54 (very high fatigue score, n = 2), respectively.
Baseline demographic characteristics of COPD patients.

AIR, Anxiety Inventory for Respiratory Disease; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; ISWT, Incremental Shuttle Walk Test; MCFS, Manchester COPD Fatigue Scale; mMRC, Modified Medical Research Council; SGRQ, St. Georges Respiratory Questionnaire.
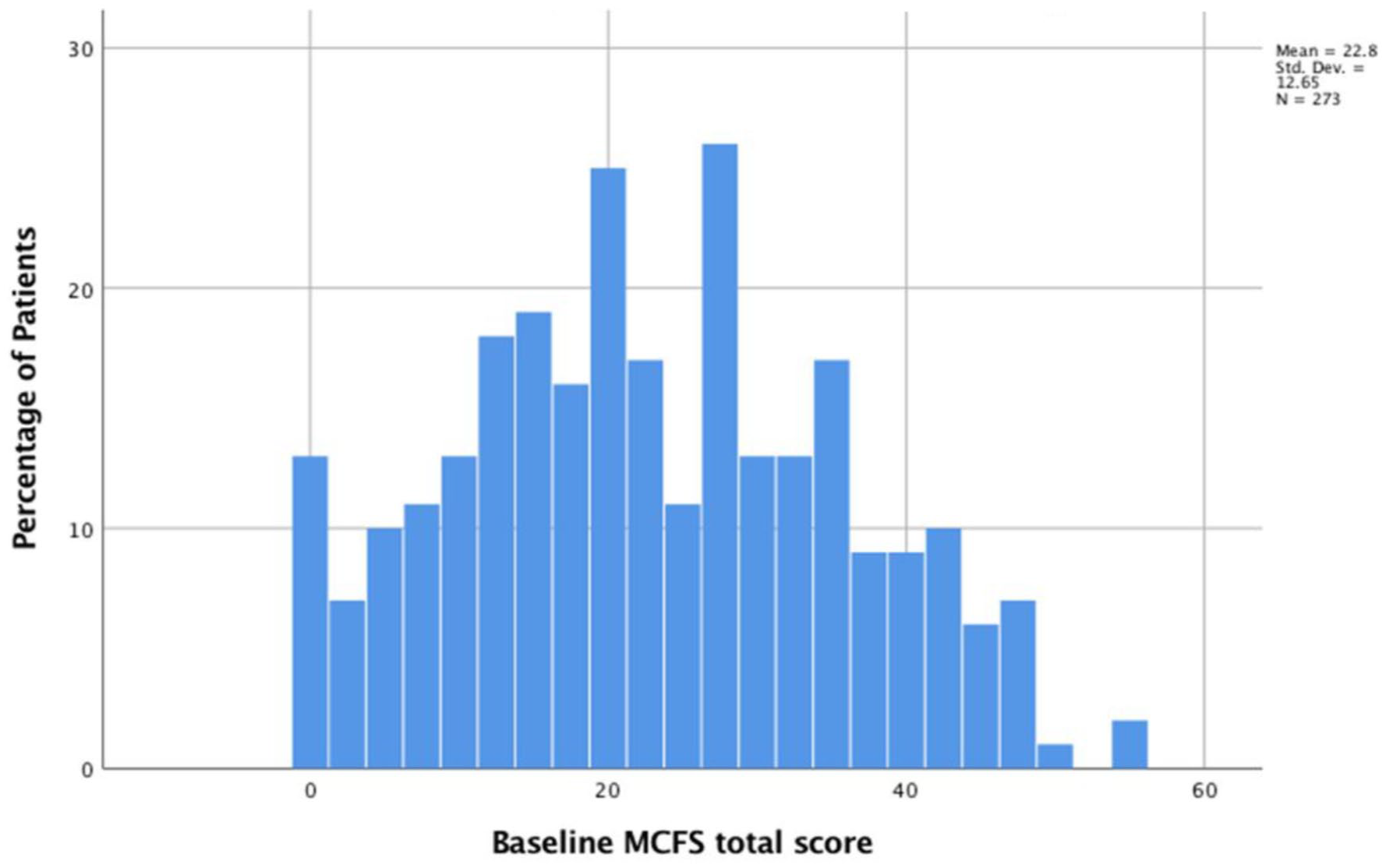
Histogram of the Manchester COPD Fatigue Scale total score.
There was no statistically significant difference in baseline MCFS total score between completers (n = 273) and noncompleters of PR (n = 79) mean 23.35 ± 13.24 versus 24.70 ± 17.7, t = 0.55, p = 0.58. However, completers were older in age compared with noncompleters mean 72.0 ± 8.9 versus 67.5 ± 10.9, t = 3.21, p < 0.002.
Comparison between MCFS scores and other clinically relevant measures
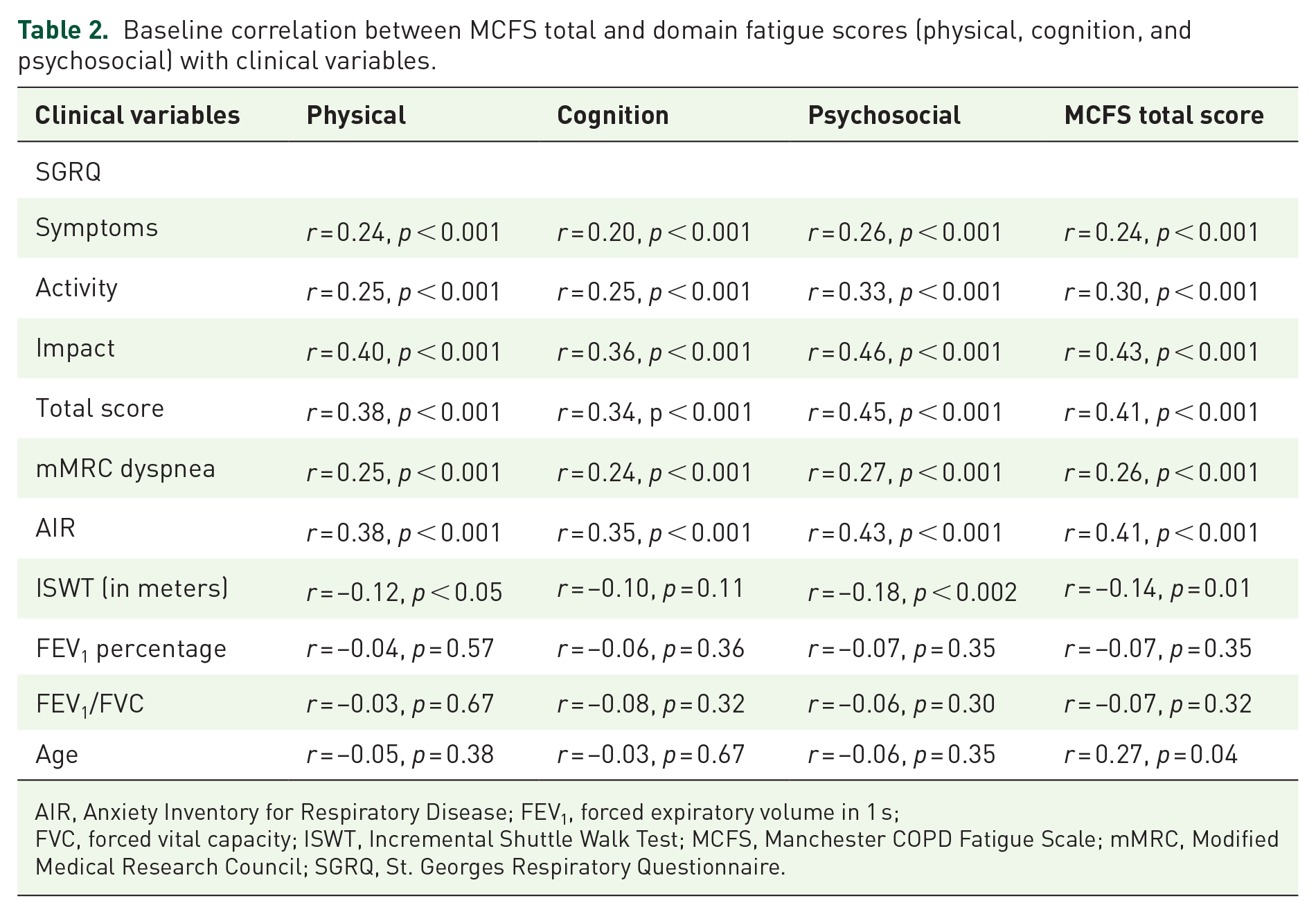
The baseline MCFS total, physical, cognition, and psychosocial scores were weakly associated with the SGRQ total and SGRQ domains (except SGRQ symptoms), ISWT, and AIR scores (all p < 0.001) as shown in Table 2 and Figure 2. MCFS score was weakly associated with SGRQ symptoms score (r = 0.24, p < 0.001), mMRC dyspnea score (r = 0. 26, p < 0.001), age (r = 0.27, p = 0.04), ISWT (r = 0.14, p = 0.01), and uncorrelated with FEV1 (r = 0.07, p = 0.30).
Baseline correlation between MCFS total and domain fatigue scores (physical, cognition, and psychosocial) with clinical variables.
AIR, Anxiety Inventory for Respiratory Disease; FEV1, forced expiratory volume in 1 s;
FVC, forced vital capacity; ISWT, Incremental Shuttle Walk Test; MCFS, Manchester COPD Fatigue Scale; mMRC, Modified Medical Research Council; SGRQ, St. Georges Respiratory Questionnaire.

Scatter plot of the Manchester COPD Fatigue Scale (MCFS) total score versus St. Georges Respiratory Questionnaire (SGRQ) total score.
Internal responsiveness
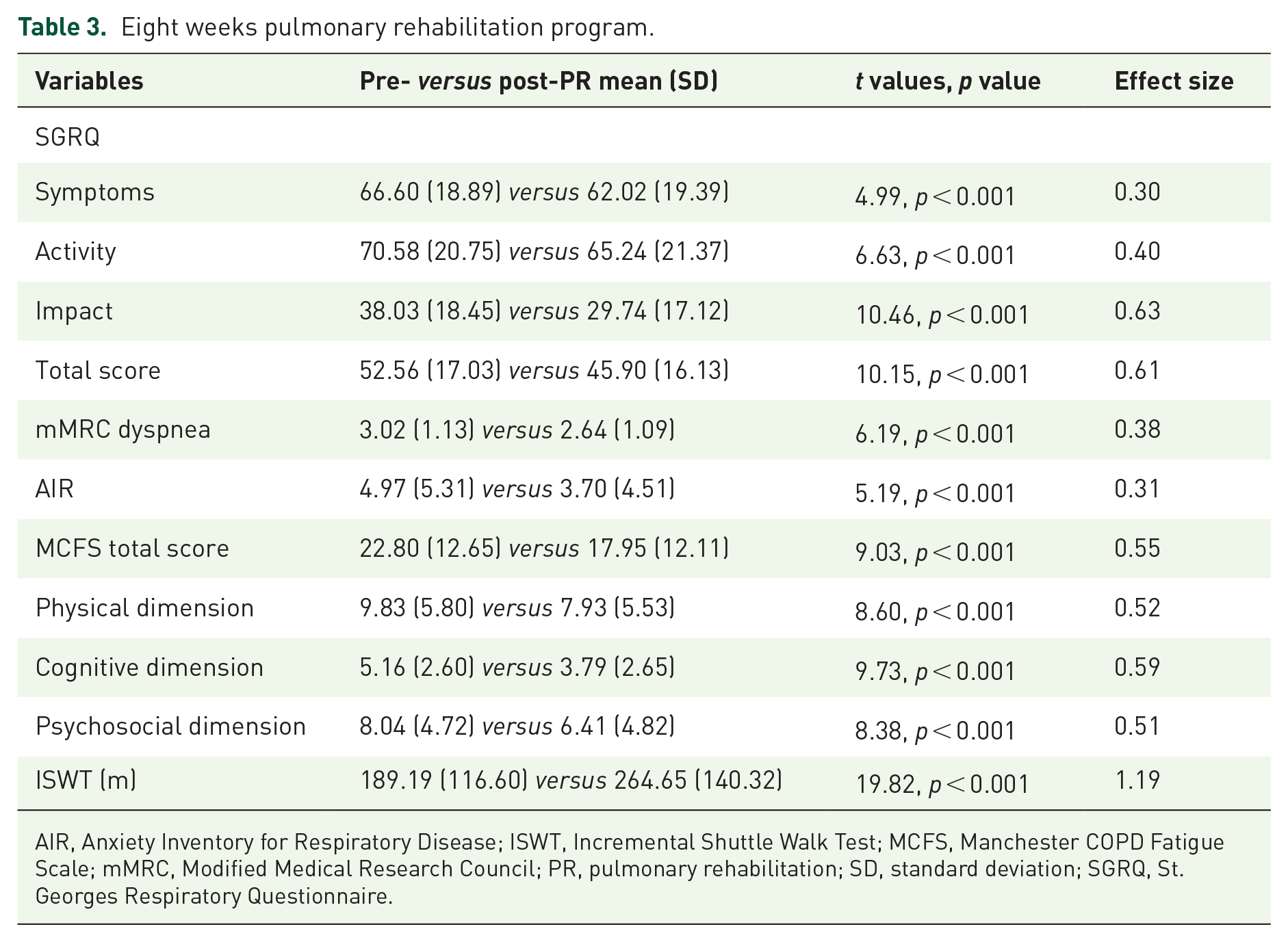
Following PR, we observed clinically significant improvement in the total MCFS, total SGRQ, and domains (symptoms, activity, and impact), mMRC dyspnea, anxiety, and exercise capacity (Table 3). MCFS total score fell −4.85 (–7.9 to −3.79) and MCFS domains all fell: physical, −1.89 (–2.33 to −1.46); cognition, −1.37 (–1.65 to −1.09); psychosocial, −1.62 (–2.00 to −1.24). Other measures also improved after PR: total SGRQ, −6.66 (–5.37 to 7.95); mMRC dyspnea, −0.38 (–0.26 to 0.50); AIR −1.27 (–0.79 to 1.75); and ISWT 75.45 (67.96–82.95). ES for MCFS and domains were moderate: total MCFS, 0.55; physical, 0.52; cognition, 0.59; and psychosocial, 0.51. Effect sizes for other measures were small to large: AIR, 0.21; SGRQ, 0.66; mMRC dyspnea, 0.38; and ISWT, 1.19. The improvement for the total MCFS was 4.85 points, corresponding to a 21% reduction from baseline.
Eight weeks pulmonary rehabilitation program.
AIR, Anxiety Inventory for Respiratory Disease; ISWT, Incremental Shuttle Walk Test; MCFS, Manchester COPD Fatigue Scale; mMRC, Modified Medical Research Council; PR, pulmonary rehabilitation; SD, standard deviation; SGRQ, St. Georges Respiratory Questionnaire.
External responsiveness
Table 4 shows the significant association of mean change in total MCFS score with mean change in SGRQ impact (r = 0.21, p < 0.001), SGRQ total (r = 0.19, p < 0.004), AIR (r = 0.19 p < 0.002), and dyspnea (r = 0.12, p = 0.04). The change in total MCFS did not significantly correlate with change in SGRQ symptoms (r = 0.01, p = 0.86), SGRQ activity (r = 0.10, p = 0.10), or ISWT (r = 0.06, p = 0.30). Change in the domains of physical related with change in SGRQ impact (r = 0.17, p < 0.006), in SGRQ activity (r = 0.16, p < 0.007) in SGRQ total (r = 0.19, p < 0.001), and dyspnea (r = 0.20, p < 0.001). Likewise, change in cognition related with change in SGRQ impact (r = 0.22, p < 0.001), in SGRQ total (r = 0.21, p < 0.001) and mMRC dyspnea (r = 0.16, p < 0.001). Equally, change in psychosocial related with change in SGRQ impact (r = 0.19, p < 0.002), in SGRQ total (r = 0.17, p < 0.004) and dyspnea (r = 0.17, p < 0.005) after PR.
Correlation change in MCFS total fatigue, physical, cognition, and psychosocial scores with changes in clinical variables.

AIR, Anxiety Inventory for Respiratory Disease; ISWT, Incremental Shuttle Walk Test;
MCFS, Manchester COPD Fatigue Scale; mMRC, Modified Medical Research Council; SGRQ, St. Georges Respiratory Questionnaire.
Table 5 identifies factors best determining change in MCFS score following PR, identified by linear regression. A baseline high MCFS score and reduced exercise capacity both significantly contributed, with adjusted R2 = 0.19. Further analysis showed that baseline high-level fatigue score contributed 15% of the variance, low score exercise tolerance contributed only 4% of the variance.
Predictors of change in total MCFS score (multiple regression analysis).

AIR, Anxiety Inventory for Respiratory Disease; ISWT, Incremental Shuttle Walk Test;
mMRC, Modified Medical Research Council; MCFS, Manchester COPD Fatigue Scale; SGRQ, St. Georges Respiratory Questionnaire.
After PR, 156 of 273 (57%) patients reported feeling much better, 91 (33%) patients reported feeling a little better, 24 (8%) reported no change, and 4 (2%) patients reporting a feeling a little or much worse. The mean change in total MCFS in those feeling ‘much better’ was − 5.05 (–6.31 to −3.79). For those feeling ‘a little better’, the mean change in total MCFS was −4.73 (–6.93 to −2.53).
Discussion
This is the first study to demonstrate the MCFS scale validly and responsively measures fatigue in patients with COPD after PR. The change in MCFS correlated with changes in established, disease-specific health-related QoL and anxiety scales in patients with COPD. Notably, after successful completion of PR, 90% of participants reported feeling better, with a mean change of 4.9 points in total MCFS.
Previous, small sample size studies in PR using the Multidimensional Fatigue Inventory (MFI), a generic fatigue scale, were inconclusive. Lewoko and colleagues showed that 7 weeks of PR for 23 patients with COPD significantly reduced fatigue, but not equally distributed across the 5 components of fatigue. 19 In a randomized, controlled trial with 26 patients, Theander et al. found 12 weeks of PR ineffective at improving fatigue frequency, duration, and severity. 20 These studies may have simply been underpowered to detect clinically significant changes in fatigue after PR, or the MFI may lack sensitivity in patients with COPD. In contrast, with a large sample size, we found the MCFS improved after PR: with a 4.9-point change that is likely to be clinically significant. Furthermore, our focus on improving in their health status far outweighed those who had worsening (90% versus 2%, rendering to GRCQ), perhaps suggesting a larger effect of PR, which, in turn, augmented the observed improvement in total MCFS and its domains. In addition, the moderate ES for the total MCFS and physical, cognitive, and psychosocial domains highlights the potential utility of MCFS as a clinical tool to measure fatigue in PR.
Baseline total MCFS and domains were weakly correlated with clinically relevant markers of QoL, anxiety, dyspnea, and exercise capacity (Table 2). These findings confirm prior clinical studies showing the relationship between fatigue and impaired QoL, anxiety, and depression in patients with COPD.4,9,20 Interestingly, the relationship between fatigue and exercise capacity is weaker than reported previously. 19
Further analysis between changes in fatigue and clinically relevant outcome measures of PR uncovered improved total SGRQ score and reduced anxiety weakly correlated with reduced MCFS. A potential explanation for this finding might be as fatigue is one of the common symptoms of COPD that patients may experience in their daily activities, as the burden of fatigue reduced, which, in turn, may have improved their general health status. Others have shown that untreated high level of fatigue was related with increased respiratory symptoms, anxiety, and depression, 21 and a 10-fold increased risk of future hospitalization in patients with COPD. 22
A number of factors predicted change in fatigue score after PR (Table 5). The most significant predictor of change in fatigue score was the presence of baseline high load of fatigue symptoms, contributing 15% of the variance in MCFS scores and indicating that such patients are most likely to derive significant benefit following PR. Likewise, we found that those with baseline low exercise capacity achieved the greatest improvement in fatigue score, with exercise capacity accounting for 4% of the variance. Our findings corroborate with a recent systematic review and meta-analysis confirmed the efficacy of an exercise program the short-term improvements in physical functioning and in reducing in level of fatigue in patients with breast cancer with 6 months of follow up. 23 Our observed significant reduction in fatigue score after PR highlights the MCFS scale is a sensitive and, therefore, useful tool in patients with COPD.
Some of the limitations of our study need to be highlighted. First, this is an observational and uncontrolled design, examining the responsiveness of MCFS after PR. Second, the cross-sectional nature of the population and lack of follow-up after PR did not allow us to examine the persistence of PR benefits over time or to examine whether MCFS in patients with COPD can predict healthcare utilization (e.g. emergency care or hospital admission). Previous studies have shown that increased fatigue was related with frequency of acute exacerbations, hospitalizations, and in-creased length of stay.21,22,24 Furthermore, elevated fatigue was related with high mental illness burden, which challenged patients coping resources and making fatigue as a symptom difficult to accept. 25 Thus, future studies need to focus on prospective randomized controlled trial to examine the effect of fatigue and healthcare costs in this patient group. Third, this single site study may have limited generalizability. However, our participants from an outpatient community setting, with equal distribution of gender and mild-to-moderate respiratory impairment, reflects a real-world setting in clinical practice. The drop-out rate from our PR was about 22% and slightly younger in mean age than who completed the program and comparable to previous studies.16,26 In addition, we have not explored the potential impact of comorbidities (e.g. cardiovascular or metabolic disorders), obstructive sleep apnea, falls, and the use of long-term oxygen therapy and domiciliary noninvasive mechanical ventilation on fatigue level in patients with COPD. Moreover, we did not examine the impact of low-grade inflammation, such as C-reactive protein that may contribute to increased fatigue or daytime sleepiness in this patient group. The self-report nature of fatigue did not allow us to delve in the cause(s) of fatigue neither physiological, which is normal (owing to tiredness from physical exercise), nor pathological, due to medical or emotional disorder; to distinguish may require further testing. Finally, caution is required as the findings of the study may not apply to the entire COPD population, especially those who are unable to attend outpatient PR such as homebound COPD patients because of their severe respiratory impairment. Moreover, the study was conducted in the UK; thus, it is important to replicate the findings in international studies. The strengths of our study include the prospective design and its large sample size, the effect size of the intervention was moderate to high in many of the clinical markers. Our findings highlight fatigue is common in patients with COPD. It should be examined and treated accordingly whenever raised as perceived problems in activities of daily living by patients and excessive sleepiness or tiredness observed by physicians during physical examination and/or consultation. It is noteworthy that 8 weeks of PR was effective in ameliorating fatigue in patients with COPD.
In conclusion, our study demonstrates that the MCFS is responsive to the effects of PR in patients with COPD, and change in MCFS correlated with reduced dyspnea, anxiety, and improved QoL following PR. Further prospective randomized controlled trials are needed to examine the efficacy of MCFS with long-term follow up.
Footnotes
Acknowledgements
We are most grateful to Joanne Tomlinson, Helen Sanderson, and Janet Porter who helped us in the data collection and for all patients who participated in our PR program.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AMY and SD have no conflicts of interest. NAH has received consultation fees and expenses paid for serving on advisory boards or as a consultant from Astra Zeneca, GSK, Boehringer Ingelheim, Mylan, Sunovion, Sanofi Genzyme, and Novartis. His institution received research grant support on his behalf from Astra Zeneca, GSK, and Boehringer Ingelheim.