
Abstract
Background and objective:
This study was performed to investigate the effect of expressive art therapy (EAT) on the health status of patients with chronic obstructive pulmonary disease (COPD).
Methods:
This community-based cluster randomized controlled trial involved patients with COPD from 16 communities in China. Participants received either EAT plus usual care (UC) or UC only. General practitioners were trained in EAT before the intervention. The primary outcomes were depression and anxiety symptoms, measured with the Hospital Anxiety and Depression Scale (HADS) and expressed as the HADS score for depression or anxiety (HADS-D or HADS-A, respectively). The secondary outcomes were the quality of life and dyspnoea, measured with the COPD assessment test (CAT). Dyspnoea was assessed using the modified Medical Research Council (mMRC) dyspnoea scale. Lung function was expressed as the forced expiratory volume in 1 s as a percentage of the predicted value [FEV1 (% pred)]. Outcome data were collected from all participants at baseline, 2 and 6 months.
Results:
In total, 360 participants with COPD and comorbid depression were included in the analysis with the control group of 181 receiving UC only and the intervention group of 179 receiving EAT plus UC. The EAT group showed significantly greater improvement in the HADS-D and HADS-A scores than the UC group at 2 months (p < 0.0001 and p < 0.001, respectively) and 6 months (p < 0.001 for both). The CAT and mMRC scores were significantly lower in the EAT group than in the UC group at 2 and 6 months (p < 0.001 for all). The FEV1 (% pred) was significantly higher in the EAT group than in the UC group at 6 months (p < 0.01).
Conclusion:
General practitioners can deliver EAT interventions. EAT can effectively reduce anxiety and depression symptoms and dyspnoea, improve quality of life and improve the pulmonary function of patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable heterogeneous disease.1,2 It is generally caused by airway and alveolar abnormalities due to long-term exposure to toxic particles or gases and is affected by host factors (e.g. lung dysplasia).1,2 COPD is characterized by airflow limitation and persistent respiratory symptoms.1,2 About 300 million people worldwide are affected by COPD. COPD causes more than 3 million deaths worldwide every year. Although progress has been made in treating symptoms and preventing acute exacerbations, few advances have been made in improving disease progression or decreasing mortality.1,3 COPD is currently the third leading cause of death worldwide following only ischaemic heart disease and stroke. 4 The prevalence of COPD is expected to continue increasing during the next 40 years. By 2060, more than 5.4 million people may be dying of COPD and its related diseases every year. 5 Two recent surveys showed that in Mainland China, 13.6–13.7% of adults aged ⩾ 40 years were affected by COPD.6,7 In 2017, the mortality of COPD was 68 per 100,000 people, and COPD was the fourth major cause of disability-adjusted life years in China. 8 COPD is still a major public health problem worldwide.
Patients are prone to anxiety, depression and other psychological disorders owing to the long course of COPD, high relapse rate and gradually decreasing lung function. 9 Comorbid psychological disorders make patients with COPD prone to fatigue, weight changes, sleep disturbances, agitation, irritability, difficulty concentrating, 10 increased functional impairment, 11 disability, 12 morbidity, 13 lower quality of life 14 and decreased adherence to treatment. 15 Preliminary evidence suggests that psychological factors should be given attention during treatment and rehabilitation.16,17
Studies have shown that early detection and treatment of anxiety and depression in patients with COPD have additive therapeutic benefits.18,19 Although drugs can reduce the symptoms of anxiety and depression, many patients are reluctant to take drugs20,21 and instead prefer non-drug treatments. 22 Clinical guidelines advocate non-drug interventions as the first-line treatments for depression and anxiety in patients with long-term conditions.23,24 The psychosocial interventions can improve both psychological and physical outcomes of patients with COPD. 25
Expressive art therapy (EAT), which includes movement, drawing, painting, sculpting, music, writing, sound and improvisation, provides participants of all ages with a platform to release feelings, increase self-awareness and explore hidden feelings in a supportive setting (schools, outpatient clinics, day treatment centres, other treatment centres, hospitals and non-clinical settings).26–28 The value and usefulness of EAT in various mental health contexts are well documented.27,29
However, no trials have studied the effect of EAT on reducing anxiety and depression symptoms in patients with COPD. In previous studies, EAT was carried out by a team of psychologists, nurse educators and doctors in the hospital setting rather than by general practitioners in the community setting; thus, the study findings did not facilitate continuous promotion of treatment on the community level. Therefore, we conducted a community-based cluster randomized controlled trial to test the hypothesis that EAT intervention provided by general practitioners reduced anxiety and depression symptoms and improved quality of life in patients with COPD.
Methods
Study setting
This community-based randomized controlled trial involved two groups of patients with COPD and was conducted from September 2018 to October 2019 in Xuzhou City. This region is located in the northern region of Jiangsu Province of eastern China and is moderately well developed, containing 3980 villages/communities and a population of 10 million. About 298,000 subjects with COPD were registered in all of the communities (an average of 75 subjects per community). According to the requirements of Chinese health authorities, health care for patients with COPD was provided on three levels: specialized services provided by county-level comprehensive hospitals, a general practitioner team set up by the members of community health service centres and health service stations to take charge of daily management, and general practitioners in community health service stations acting as contracted family doctors. 30 Since private clinics were not allowed to provide public health services, health service stations were typical official units for the management of patients in communities. No geographical or cultural belief differences were present among the paired communities included in this study. The only health care unit in each community was the community health service centre. According to the data provided by the environmental protection department, no air pollution was present in any of the observation areas of this study.
Study design
Communities with sufficiently sized populations were phoned to determine whether their general practitioners had basic skills in singing, painting, dancing and the willingness to participate in this study. Overall, 790 communities had more than 120 patients with COPD. General practitioners in 105 of these communities could not sing, paint or dance; 37 of these communities were reluctant to participate; finally, 648 communities met these criteria. However, 16 were recruited from 648 communities by our researchers with the table of the random digit. These 16 eligible clusters (villages/communities) were randomly assigned to receive EAT plus usual care (UC) [EAT (intervention) group] or UC [UC (control) group] with a 1:1 parallel design. A random number table was used to assign clusters for the EAT or UC interventions on the individual level. The baseline survey was conducted from December 2018 to February 2019. The primary and secondary outcomes and subject-specific variables were collected during the baseline survey, 2 and 6 months. All data collection was completed in September 2019. All assessments were conducted in a face-to-face manner by the investigators of our research team at the community health service station. All participants provided informed consent and received a gift at the end of each investigation.
Participants
Participants with COPD and comorbid depression symptom [Hospital Anxiety and Depression Scale for depression (HADS-D)] score of ⩾8 were invited to participate in this study. The inclusion criteria were COPD meeting the 2017 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, 1 stable condition, normal perception, normal communication skills and provision of written informed consent. The exclusion criteria were a HADS-D score of <8, a medically unstable condition, comorbid malignant tumours, active tuberculosis, severe liver disease or heart failure, a history of alcoholism or psychotropic drug dependence, pregnancy or lactation, mental disorders, incomplete clinical data and refusal to participate in this study. The endpoints were the final follow-up results of each participant. Participants were lost to follow-up if we were unable to contact them or if they moved to another location, withdrew their consent, refused to continue, had invalid data or were unable to complete the study.
Sample size
According to the principle of a two-level cluster random design and assuming statistical test power of 80%, bilateral type 1 error of 5%, intracluster correlation coefficient of 0.22% and follow-up failure rate of 10%, we determined that at least 16 communities and 340 patients with COPD and comorbid depression in the EAT or UC group (20 participants in each community) would be needed to detect a 2.1 relative reduction (standard deviation, 3.9) of depression symptoms (assessed using the HADS) between two groups. 31 Considering that the prevalence of depression in patients with COPD is reportedly 22.8%, at least 88 participants were needed in each community. 32 Finally, considering the potential exclusion of participants based on the above-mentioned eligibility criteria, we estimated that at least 120 patients would be needed in each community. There were 790 communities with more than 120 patients with COPD.
Ethical considerations
This study adhered to the Consolidated Standards of Reporting Trials (CONSORT) extension for cluster trials guidelines. 33 This study was carried out according to the protocols approved by Xuzhou Centre for Disease Control and Prevention and approved by the Xuzhou Medical Science Ethics Committee (Approval No. 2012010). All participants provided written informed consent, underwent a pulmonary function test and completed all required information. The trial was registered with the Chinese Clinical Trials Registry (reference: ChiCTR-TRC-12001958) and conducted according to the 2000 revised version of the Helsinki Declaration.
Randomization and masking
After assessing depression and anxiety, we stratified the cluster randomization according to the number of general practitioners and qualified participants. A research statistician who had no contact with the participants produced the randomization sequence. The corresponding authors randomly assigned 16 communities to receive either EAT plus UC (intervention group) or UC only (control group) in a 1:1 ratio using a random number table. The participants were recruited by our team members and general practitioners. The general practitioners were responsible for notifying and convening the recruited members, our team members were responsible for explaining the patient’s instructions to the participants and signing the informed consent. The general practitioners were informed of the results at the baseline. The chief investigators and statisticians were blinded to the grouping.
Interventions
UC (all participants)
The UC group received UC from general practitioners based on the patients’ individual needs. Every 2 months, the caregivers were asked to ascertain each patient’s health status by telephone or face-to-face interview, recorded the patient’s health status and then reported the information to our research group. In the case of health deterioration, participants received medication or were referred to a respiratory specialist according to the GOLD guidelines. The content and frequency of UC services were not standardized.
EAT
Training of general practitioners
A total of 70 general practitioners from 8 health service centres received 3 working days of training in EAT for the intervention group. The training contents were generated based on previous research and included six sessions, each session involving 45–50 min of lectures and 10–15 min of discussions for three consecutive working days. The six sessions included (1) drawing with the theme of self-knowledge, (2) a sand table game with the theme of self-relaxation, (3) writing with the theme of expelling troubles, (4) music (singing and playing the harmonica, flute and suona horn) with the theme of relieving stress, (5) speech focusing on the topic of a bright future and (6) dance movements (mainly folk dance). Each general practitioner underwent a closed-text examination at the end of each class.
Implementation of EAT sessions for participants
All participants in the EAT group were asked to attend a lecture and were encouraged to practice at home after classes. However, 20–25 people in each group were from the same community, and most of them were familiar with each other. The general practitioners called the participants to the health education room of the health service stations by telephone, Tencent Instant Messenger or WeChat. Each participant should sign in when they arrived, were given the name card and sat in a semicircle, and were required to attend lectures on time, respected each other and kept their privacy. On each day of the first week, trained general practitioners gave participants 45–50 min of lectures followed by 10–15 min of discussions. Members of our study group attended the lecture in the first week; after class, they commented on the lectures and received questions from the participants. The participants subsequently received lectures and discussions twice a week for 6 weeks. After each class, the general practitioner assigned homework to the participants and instructed them in how to record and complete the homework. From the beginning of the second class, the participants were asked about the completion of their homework assigned during the previous class. The general practitioners used mobile phones to record each class and upload it to us to evaluate the quality of the class.
Evaluating intervention fidelity
Sessions were audio-recorded with a smartphone to assess fidelity and provide feedback to providers. Two experienced clinical psychologists rated sessions for adherence and competence using an accepted scale. 34 Scores ranged from 1 to 8, with scores of 4 and 5 considered moderately adherent/competent and scores of 6, 7 and 8 considered good, very good and excellent, respectively. 34
Outcomes
The primary outcomes were depression and anxiety, and were screened and measured with the HADS. The HADS is a 14-item scale; 7 of the items are relevant to anxiety (HADS-A) and 7 are relevant to depression (HADS-D). Scores range from 0 to 21, and scores of ⩾ 8 on a sub-scale are considered an indication of possible anxiety or depression. 35 Higher scores are associated with more serious anxiety or depression symptoms.
The secondary outcomes were quality of life, dyspnoea and lung function. Quality of life was measured using the COPD Assessment Test (CAT), 36 which includes eight items, each with a score of 0–5, giving a total score of 0–40; higher scores indicate a poorer health status. Dyspnoea was assessed using the modified Medical Research Council (mMRC) dyspnoea scale, 37 the score of which ranges from 0 to 4 points, with higher scores indicating more severe dyspnoea. Lung function was expressed as the forced expiratory volume in 1 s as a percentage of the predicted value [FEV1 (% pred)], with lower values indicating more severe airway obstruction.
Other demographic variables
Subject-specific variables were collected by a self-designed questionnaire and included sex, age, body mass index, disease course, smoking index, number of acute exacerbations and number of acute exacerbations requiring hospitalization during the follow-up period. Medication regimens were obtained by patient interviews, healthcare databases or prospectively from diary cards, and the frequency of each medication was recorded. The body mass index was calculated by dividing the weight in kilograms by the height in meters squared. The smoking index was equal to the number of cigarettes per day multiplied by the number of years of smoking.
Statistical analysis
EpiData 3.1 (The EpiData Association, Odense, Denmark) was used to input and manage the data. Continuous variables are presented as mean ± standard deviation. Normally distributed data were analysed with a parametric test, and non-normally distributed data were analysed with a non-parametric test. The chi-square test was used to analyse categorical variables, which are presented as frequency and percentage. The t-test or chi-square test was used to analyse between-group differences in continuous and categorical variables at the baseline, respectively. Repeated-measures analysis of variance was used to examine within-group variation before and after the intervention (time × group interaction effect). Intention-to-treat analysis was performed using the last HADS, CAT and mMRC scores, including the non-completers. SPSS 17.0 (SPSS Inc., Chicago, IL, USA) was used for all calculations, and the threshold for statistical significance was set at p = 0.05.
The between-group effect size is represented by Hedges’ g, and the within-group effect size is represented by Cohen’s d. An effect size of 0.2–0.5 was considered small, 0.5–0.8 was considered medium and ⩾ 0.8 was considered large. 38
Results
Setting
A total of 2003 patients with COPD were enrolled in the 16 recruited communities, 38 prospective recruits with acute exacerbation, 198 with evaluated life expectancy ⩽ 1 year and 284 with refused to participate were excluded, 1483 prospective recruits participated in the final assessment. The EAT and UC groups were similar in the cluster and individual levels at the baseline (Table 1). The number of communities had not changed at 2 and 6 months in either group. The number of participants and the number of general practitioners in each community were also similar between the two groups on the group level at these time points (Table 1).
Baseline characteristics between the EAT and UC groups.
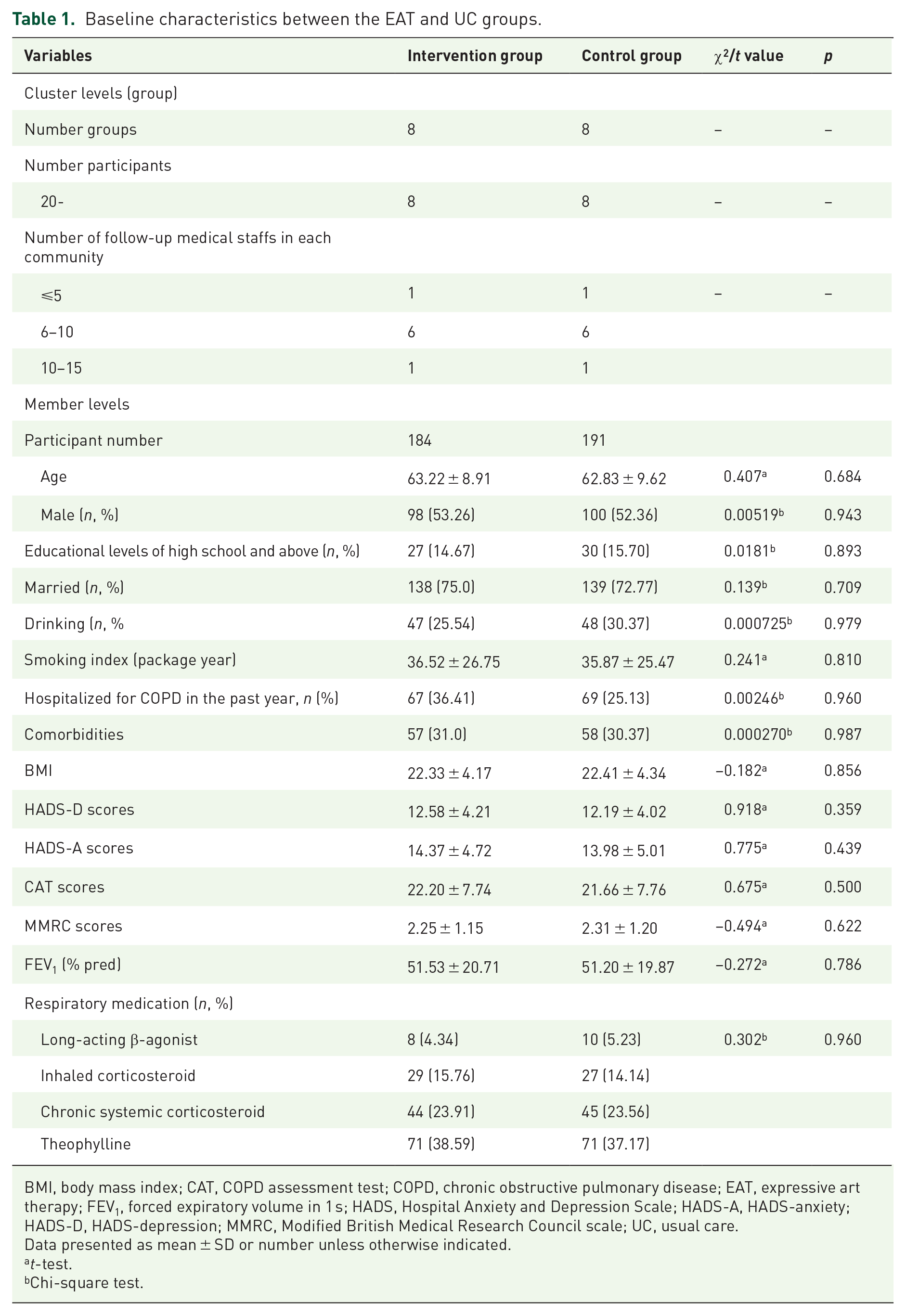
BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; EAT, expressive art therapy; FEV1, forced expiratory volume in 1 s; HADS, Hospital Anxiety and Depression Scale; HADS-A, HADS-anxiety; HADS-D, HADS-depression; MMRC, Modified British Medical Research Council scale; UC, usual care.
Data presented as mean ± SD or number unless otherwise indicated.
t-test.
Chi-square test.
Figure 1 shows a participant flow diagram according to the CONSORT extension for cluster trials. In total, 184 participants from eight different communities were randomly allocated to receive EAT plus UC, and 191 participants from eight different communities were randomly allocated to receive UC. There were no significant differences in the general characteristics at either the group or individual level between the two groups at the baseline (Table 1). The study began on 1 March 2019 and ended on 31 August 2019. The final analysis included 360 participants’ complete data; the data of 15 non-completers (6 and 9 in the EAT and UC group, respectively) were omitted. The general characteristics of the completers were not significantly different at the individual level between the two groups at baseline, 2 and 6 months (p > 0.05). No participants received other non-drug treatments during the 6-month follow-up.

CONSORT flow diagram of the participants.
Intervention fidelity
The general practitioners provided EAT to an average of 21 participants (median, 22; range, 20–24). In total, 48 audio recordings were gathered and evaluated for fidelity. The raters assessed an average of 7.0 sessions for each provider. The average adherence and competence ratings for all general practitioners were in the ‘good’ to ‘very good’ range (adherence, 6.9; competence, 6.5).
Changes across cluster levels (groups)
There were no differences in the number of participants in each group at 2 and 6 months. The number of groups and the number of follow-up medical staff members in each community had not changed at 2 and 6 months.
Changes in HADS-D score
The mean HADS-D scores in the EAT and UC groups were 12.58 ± 4.21 and 12.19 ± 4.02 points at the baseline, respectively, with no significant difference (t = 0.918, p = 0.359). The EAT group had a 2.84-point lower HADS-D score than the UC group at 2 months [95% confidence interval (CI), 2.35–3.35; p < 0.001] and a 2.38-point lower HADS-D score at 6 months (95% CI, 2.11–2.65; p < 0.001). The main effect of time was significant (F = 13.61, p < 0.001), indicating the time of treatment continuation to 6 months. The interaction effect was significant (F = 11.97, p < 0.001), indicating that the effect of time was significantly different between the EAT and UC groups (Table 2).
Comparison of HADS-D, HADS-A, CAT, mMRC scores and FEV1 values between the EAT and UC groups.
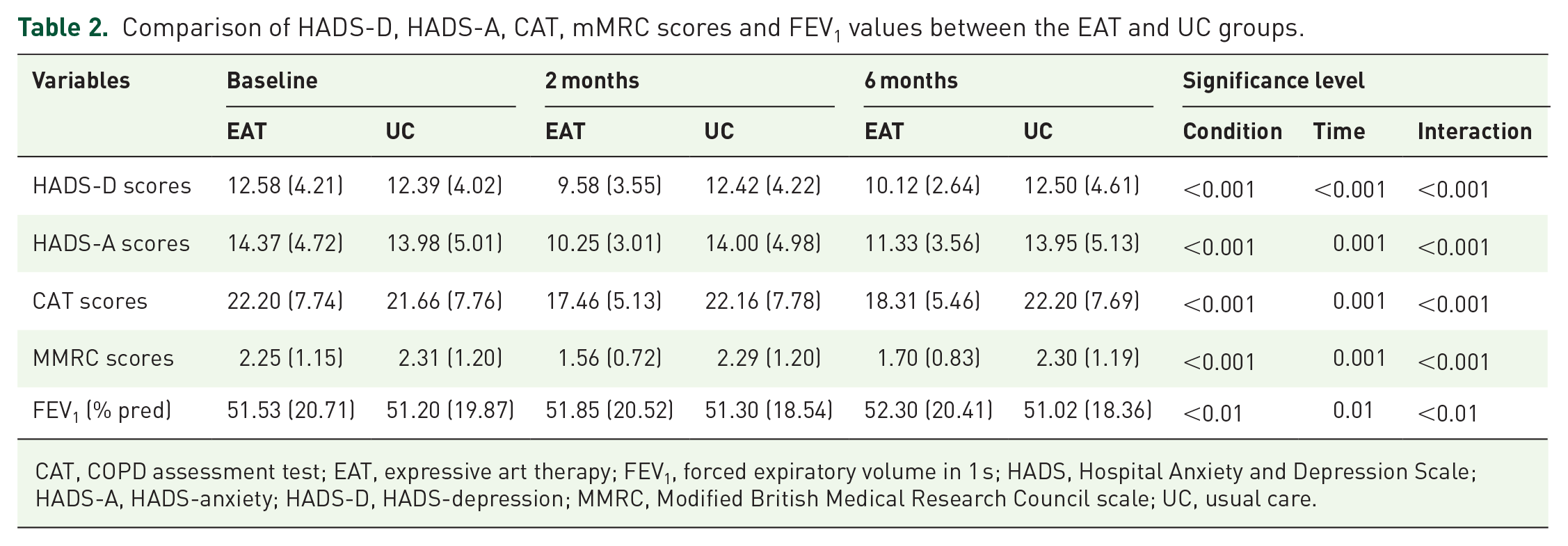
CAT, COPD assessment test; EAT, expressive art therapy; FEV1, forced expiratory volume in 1 s; HADS, Hospital Anxiety and Depression Scale; HADS-A, HADS-anxiety; HADS-D, HADS-depression; MMRC, Modified British Medical Research Council scale; UC, usual care.
Changes in HADS-A score
At the baseline, the mean HADS-A scores in the EAT and UC groups were 14.37 ± 4.72 and 13.98 ± 5.01 points, respectively, with no significant difference (t = 0.775, p = 0.439). After the intervention, the EAT group had a 3.75-point lower HADS-A score than the UC group at 2 months (95% CI, 3.18–4.31; p < 0.001) and 2.62-point lower HADS-A score at 6 months (95% CI, 2.22–3.03; p < 0.001). The main effect of time was significant (F = 13.61, p < 0.001), indicating the time of treatment continuation to 6 months. The interaction effect was significant (F = 11.97, p < 0.001), indicating that the effect of time was significantly different between the EAT and UC groups (Table 2).
Changes in quality of life
Changes in the CAT score in the EAT and UC groups are shown in Table 2. At the baseline, there was no significant difference in the mean CAT score between the two groups (t = 0.675, p = 0.500). However, the EAT group had a 4.70-point lower CAT score than the UC group at 2 months (95% CI, 3.98–5.43; p < 0.001) and a 3.90-point lower CAT score at 6 months (95% CI, 3.39–4.42; p < 0.001). The main effect of time was significant (F = 13.61, p < 0.001), indicating the time of treatment continuation to 6 months. The interaction effect was significant (F = 11.97, p < 0.001), indicating that the effect of time was significantly different between the EAT and UC groups (Table 2).
Dyspnoea
Changes in the mMRC score in the EAT and UC groups are shown in Table 2. At the baseline, there was no significant difference in the mean mMRC score between the two groups (t = −0.494, p = 0.622). After the intervention, the EAT group had a 0.73-point lower mMRC score than the control group at 2 months (95% CI, 0.48–0.99; p < 0.001) and a 0.60-point lower mMRC score at 6 months (95% CI, 0.38–0.82; p < 0.001). The main effect of time was significant (F = 13.61, p < 0.001), indicating the time of treatment continuation to 6 months. The interaction effect was significant (F = 11.97, p < 0.001), indicating that the effect of time was significantly different between the EAT and UC groups (Table 2).
Lung function
Changes in the FEV1 (% pred) value in the EAT and UC groups are shown in Table 2. At the baseline, there was no significant difference in the mean FEV1 (% pred) value between the two groups (t = 0.272, p = 0.786). After the intervention, the EAT group had a 0.55% higher FEV1 (% pred) value than the control group at 2 months (95% CI, 0.30–0.81; p > 0.05) and a 1.25% higher FEV1 (% pred) value at 6 months (95% CI, 1.01–1.51; p < 0.01). The main effect of time was significant (F = 13.61, p < 0.001), indicating the time of treatment continuation to 6 months. The interaction effect was significant (F = 11.97, p < 0.001), indicating that the effect of time was significantly different between the EAT and UC groups (Table 2).
Adverse events
In total, 8 participants in the EAT group and 19 participants in the UC group were re-hospitalized within 6 months because of COPD. The difference between the two groups was statistically significant (χ2 = 4.65, p < 0.05).
Discussion
In this study, EAT delivered by general practitioners was clinically effective in patients with COPD and comorbid symptoms of depression and anxiety. EAT in the form of a group intervention also improved participants’ quality of life. The mean CAT scores at 2 and 6 months’ post-intervention were significantly lower in the EAT group than in the UC group. The mMRC scores improved at 2 months after implementation of the group EAT intervention, and the improvement persisted after 6 months. The FEV1 (% pred) values improved at 6 months along with an improved quality of life.
EAT was superior to UC in terms of the primary outcome measured at 2 months with a difference of 2.84 in the HADS-D scores and of 3.75 in the HADS-A scores at the primary endpoint, consistent with previous study findings.39–41 Our results also suggested that EAT had a medium (6-month) lasting effect on reducing HADS scores in patients with COPD.42,43
There are several possible explanations for the improved related health status of patients with COPD after the EAT intervention. One factor is that singing, playing creative music and listening to music can reduce anxiety and depression symptoms,39–41 improve quality of life40,43 and increase the 6-min walking distance 44 in patients with COPD. Patients with COPD have abnormal respiratory muscle function, which is caused by mechanical defects due to excessive lung expansion, diaphragm dysfunction, respiratory asynchrony and reduction of respiratory muscle strength. A posture that enhances diaphragm function may help alleviate dyspnoea. 45 Singing relies on an adequate air supply to the lungs to regulate the airflow and produce a large lung volume. Exhalation is active during singing, and singing thus requires active diaphragm contraction and good posture. 46 This means that singing requires the use and mastery of techniques to control breathing, making it a plausible therapy for patients with respiratory disease. Previous studies have proven that regular practice of singing by patients with COPD can not only improve functional capacity 47 but also preserve the maximal expiratory pressure. 43 One study showed that a community singing group for adults with COPD also reduced the HADS-A score and increased the 6-min walking distance at 1 year, 47 and another study demonstrated that 12 weeks of harmonica training significantly improved the 6-min walking distance in patients with COPD. 48 EAT intervention reduces dyspnoea39,49 and improves the quality of life, possibly because anxiety and depression are related to dyspnoea and quality of life in patients with COPD.50,51 Thus, when anxiety and depression symptoms are reduced, dyspnoea is also reduced and quality of life improves.
Another possible explanation for the participants’ improved health status is that dance is widely considered to include breathing, rhythm, pedestrian movement and gestures or postures, with special emphasis on imagery, symbols and metaphors. 52 Resultant improvements to physical fitness include improved exercise capacity and greater strength and balance. 53 Wshah et al. 54 confirmed that dance performed twice a week for 8 weeks increased the 6-min walking distance and improved the dyspnoea of patients with COPD. The enjoyment and social connections experienced in dance classes may also play an important role in improving mood and encouraging attendance and completion of the therapy. 53 Therefore, dance effectively improves functional capacity, balance, emotion, anxiety and depression, physical activity and health-related quality of life of both healthy people and those with chronic respiratory disease,52,53,55,56 whereas music, singing and dancing enhance participation, improve disease management and boost mood and self-confidence,57,58 potentially helping to enhance confidence and reduce psychological symptoms.
Our results are consistent with those from other studies in which painting and storytelling improved the participants’ moods. Collie et al. 59 showed that by appreciating artworks or painting graffiti, participants’ breathing frequency slowed, their length of breath increased, they were able to remain attentive and focus their attention, and they attained a good sedative effect. In other studies, older adults experienced significant improvement in their emotional well-being and protection against depression.60–62 Storytelling intervention can significantly reduce symptoms of depression and anxiety. 63 This might be explained by the fact that to be an accomplished storyteller, a participant must orchestrate many simultaneously converging processes including attention, cognition, memory, inferencing and theory of mind. 64
EAT is a particular therapy that mainly involves non-verbal media to help patients accept and integrate external stimuli and emphasize visual symbols or images. People who have experienced trauma often have many disaster scenes and emotions engraved in their brains. Through music, manual creation, visual symbols, intentional performance and other forms of art therapy, traumatized people can publicize their originally suppressed desires, emotions and traumatic experiences in the subconscious; try new methods and ways of thinking; deal with inner conflicts and develop an enhanced self-awareness so as mastering interpersonal skills, correct abnormal psychology and promote mental health. 65 Therefore, EAT can be used to treat people’s psychological and mental disorders and improve their quality of life.
The strengths of this study are that it was a community-based, two-level, randomized controlled trial with a large sample, and there was a low rate of loss to follow-up. We first incorporated EAT into UC to manage patients with COPD. The results showed that such a therapy can effectively reduce dyspnoea and anxiety and depression symptoms and improve quality of life and lung function. These findings suggest that the combination of EAT and UC for routine primary care management in China is feasible and effective. Moreover, the UC group showed no improvement in psychological outcomes and lung function, indicating the need for better routine care for the management of patients with COPD.
Some limitations of this study should also be noted. First, we used self-report questionnaires to assess anxiety and depression, quality of life and dyspnoea, which may have led to response errors and bias. Second, the sampling strategy may limit the generalization of these findings to other regions, countries and ethnic populations. However, we recruited participants from 16 communities, which may help to improve the generalizability. Third, there are potential ethical problems in that the control group did not receive EAT and that participants with sub-clinical anxiety and depression, who may have benefitted from EAT, were not included because of the strict inclusion criteria. Fourth, because interpersonal and social group communication could improve patients’ psychology, the results of this article might be overestimated.
In conclusion, EAT allows patients to fully integrate into an artistic atmosphere, express and release emotions, improve their life initiative, increase communication and regain self-esteem and self-confidence to restore their social function. It can effectively reduce patients’ dyspnoea and anxiety and depression symptoms, and improve quality of life and lung function. Some researchers have showed that non-pharmacological intervention could improve the physiology of patients with refractory breathlessness. 66 This was suggested that the COPD patients with refractory breathlessness and complications may be recruited in the next intervention. Our study also demonstrated that general practitioners are able to deliver EAT to participants and that such interventions may improve the management of patients with COPD in communities. Given the large numbers of individuals with COPD with low health status and the high prevalence of undertreated anxiety and depression in China, our findings suggest new strategies for the management of patients with COPD in community-based public health services.