
Abstract
Chronic obstructive pulmonary disease (COPD) is the most frequent chronic respiratory disease and a leading cause of morbidity and mortality, worldwide. Given that the foremost risk factor leading to the development of COPD is cigarette smoke, the initial treatment for COPD is smoking cessation. Even after smoking cessation, inflammation, apoptosis and oxidative stress can persist and continue to contribute to COPD. Although current therapies for COPD (which are primarily based on anti-inflammatory drugs such as corticosteroids, theophylline and bronchodilators) reduce airway obstruction, limit COPD exacerbation and improve the patient’s health-related quality-of-life, none can prevent disease progression or reduce mortality. Recent advances in stem cell research have provided novel insight into the potential of bone marrow mesenchymal stem cells (MSCs) in the treatment of several pulmonary diseases. This review article discusses the biological effects and mechanisms of action of MSC transplantation in COPD, and highlights the foundation that MSCs provide for novel therapeutic approaches in COPD.
Introduction
The Global Initiative for Chronic Obstructive Lung Disease defines chronic obstructive pulmonary disease (COPD) as ‘a common preventable and treatable disease, characterized by airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases’. 1 COPD is the most frequent chronic respiratory disease and currently the sixth leading cause of morbidity and mortality worldwide; it is projected to be ranked third by 2020 due to an increase in smoking rates. 2 COPD pathology includes small airway inflammation and emphysema, which is characterized by destruction of alveolar septa, leading to enlargement of the remaining distal airspaces. 3 Although COPD primarily affects the lungs, it also has significant systemic consequences. 4
Chronic obstructive pulmonary disease is mainly caused by exposure to noxious gases, such as chemicals and air pollutants, with the foremost risk factor being cigarette smoke. 5 Pathogenic mechanisms of cigarette smoke in COPD include chronic inflammation, protease/antiprotease imbalance, apoptosis and oxidative stress.6–9 Although the initial treatment for COPD is smoking cessation, inflammation, 10 apoptosis 11 and oxidative stress 12 persist even in the absence of cigarette smoke. Current therapies for COPD (which are primarily based on anti-inflammatory drugs such as corticosteroids, theophylline and bronchodilators) can reduce airway obstruction, limit COPD exacerbation, and improve health-related quality-of-life. 13 None of these therapies prevents COPD progression or reduces mortality, so a pressing need exists for the development of novel COPD therapies. 13
Recent advances in mesenchymal stem cell (MSC) therapy have made this approach a strong candidate for clinical use in the treatment of several pulmonary diseases.14–17 These multipotent nonhaematopoietic progenitors can be readily harvested from numerous tissues and expanded with high efficiency, and have strong immunosuppressive properties that can be exploited for successful autologous as well as heterologous transplantations. 18 Transplantation of MSCs has been reported in emphysemic rats, 14 murine asthma, 15 pulmonary hypertension in rats, 16 and acute lung injury in rats. 17 This review article will discuss the biological effects and mechanisms of action of MSC transplantation in COPD.
MSC transplantation may alter inflammatory processes involved in COPD pathogenesis
Chronic inflammation and COPD development
Cigarette smoke has been shown to activate macrophages directly, resulting in the release of oxidants and proteases that mediate alveolar wall destruction and contribute to the establishment of emphysema.
19
Macrophage activation also results in the release of cytokines involved in inflammatory processes in airway and lung parenchyma, including tumour necrosis factor (TNF)-α, interleukin (IL)-1β, and IL-6.
19
In addition, the release of chemokines such as IL-8, monocyte chemotactic peptide (MCP)-1, and leukotriene B4 attracts additional inflammatory and immune cells to the lungs, including neutrophils and T-cells.
20
Activated neutrophils have themselves been shown to contribute to alveolar destruction and mucous hypersecretion via the release of oxidants and proteases.
21
Moreover, activated T-cells, in particular CD8+ T-cells, release cytotoxic perforins, granzyme B and TNF-α, which directly cause cell death and apoptosis of alveolar epithelial cells, a feature of emphysema.
22
In addition to activating macrophages, cigarette smoke has also been shown to activate epithelial cells to secrete a variety of proteases and inflammatory mediators, thereby supporting the inflammatory processes that contribute to emphysema (Figure 1).
23
Schematic diagram summarizing the cigarette smoke-induced pathogenic processes involved in the development of chronic obstructive pulmonary disease (COPD). VEGF, vascular endothelial growth factor; NF-κB, nuclear factor-κB; ECM, extracellular matrix.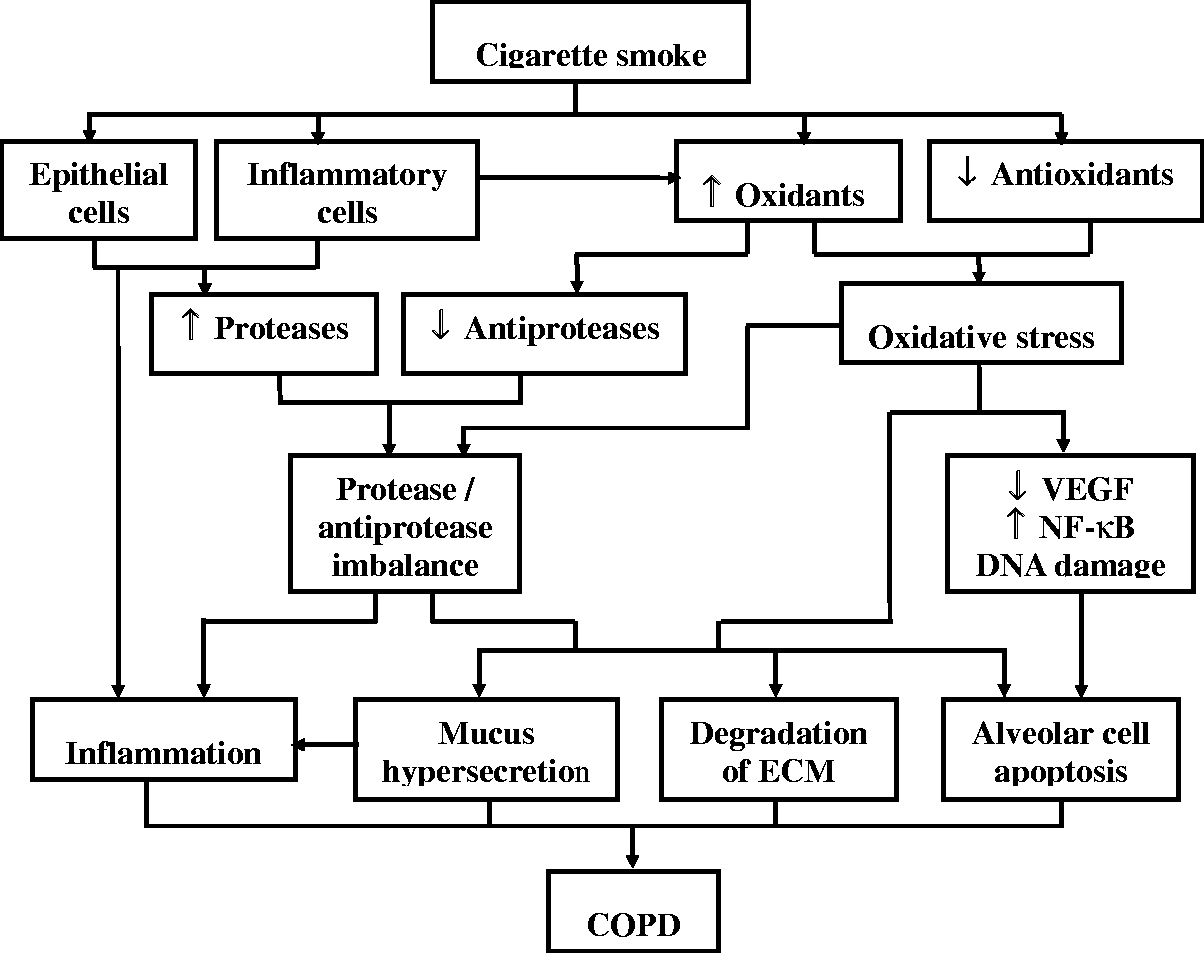
Inhibition of inflammation by transplantation of MSCs
One of the mechanisms postulated for MSC protection against emphysema is suppression of the inflammatory response by modulating the release of soluble anti-inflammatory molecules and activation of cellular anti-inflammatory pathways. 24 Intrapulmonary administration of MSCs in a rat model of cigarette smoke-induced emphysema has been shown to ameliorate emphysematous pathology in these animals, in part via downregulation of proinflammatory mediators such as TNF-α, IL-1β, IL-6 and MCP-1. 24 Moreover, intravenous infusions of allogeneic MSCs suppressed levels of circulating C-reactive protein in a clinical trial of patients with COPD, although no significant differences in pulmonary function testing or frequency of COPD exacerbations were noted between MSC-treated patients and controls. 25 Contradictions between these two studies concerning the effect of MSCs on pulmonary function may be attributed to differences in dosing and treatment, lack of correlation between rodent models and clinical disease, and the small sample size in the clinical trial.24,25 Further larger scale trials will be necessary, to examine the potential effects of MSCs on clinical outcome in patients with COPD in greater detail.
MSC transplantation and regulation of protease/antiprotease imbalance in COPD pathogenesis
Protease/antiprotease imbalance in COPD
A delicate balance between protease and antiprotease activity is required for proper lung maintenance; derangement of this can result in increased alveolar destruction and the development of emphysema. 6 The inflammatory and oxidative processes associated with exposure to cigarette smoke have been shown to increase protease production and release from inflammatory and structural cells, and to reduce the activity of antiproteases such as α1-antitrypsin. 26 The resulting protease/antiprotease imbalance contributes to alveolar wall destruction and airspace enlargement via degradation of the extracellular matrix, promoting apoptosis of structural cells in the alveolar walls, and increasing mucus hypersecretion (Figure 1).
Inhibition of protease release by MSC transplantation
Pulmonary administration of MSCs has been shown to reverse the induction of matrix metalloproteinase (MMP)-9 and MMP-12 in the lungs of rats with cigarette smoke-induced emphysema, at both the mRNA and protein levels. 24 Although the mechanistic basis of this effect is not completely understood, it has been attributed in part to the inhibition (by MSCs) of a positive feedback loop, involving the release of proteases by inflammatory and structural cells activated by cigarette smoke, and the recruitment by these proteases of additional inflammatory cells. 27
Suppression of alveolar apoptosis by MSC transplantation in COPD
Apoptosis and COPD
Apoptosis is a tightly regulated form of cell death that is critical for the maintenance of normal tissue homeostasis and which, under normal conditions, is in equilibrium with cell proliferation. 28 Apoptosis of alveolar epithelial cells is known to play a pivotal role in the pathogenesis of emphysema. 7 It has been shown that increased apoptosis of alveolar epithelial cells in patients with COPD is not balanced by an increase in their proliferation, a state that may contribute to a disturbance in COPD of the steady state balance between apoptosis and proliferation in lung tissue (Figure 1). 11
Inhibition of alveolar cell apoptosis by MSC transplantation
Blocking the vascular endothelial growth factor (VEGF) signalling pathway leads to apoptosis of the alveolar cell; and decreases in VEGF and VEGF receptor 2 (VEGFR2) at both the protein and mRNA levels have been described in emphysematous patients and smokers. 29 Given that MSCs stimulate VEGF secretion24,30 and VEGFR2 induction, 24 amelioration by MSC transplantation of alveolar cell apoptosis in the lungs of papain-31 or cigarette smoke-induced 24 rat models of emphysema has therefore been postulated to involve reversal of the effects of cigarette smoke exposure on the VEGF signalling pathway.
An alternative mechanism by which MSCs suppress alveolar cell apoptosis has been suggested to involve alterations in the expression of apoptotic or antiapoptotic genes in these cells. 32 It has been reported, for example, that the apoptotic gene Bax and the antiapoptotic gene Bcl-2 are induced and repressed, respectively, after pulmonary administration of MSCs in a papain-induced model of emphysema in rats. 32 A third mechanism for MSC amelioration of alveolar apoptosis is suggested by the suppression by MSCs of alveolar levels of cleaved-caspase 3, 33 a key player in the apoptotic programme in these cells.
MSC transplantation may alter levels of oxidative stress in COPD
Oxidative stress and COPD development
Oxidants contributing to the pathogenesis of COPD may originate endogenously, by metabolic reactions, or exogenously, primarily in the form of cigarette smoke. 34 The release of oxidants by inflammatory cells activated by cigarette smoke further increases the oxidative burden imposed by exogenous oxidants. 35 Under normal conditions, a robust pulmonary extra- and intracellular antioxidant defence system protects lung cells from oxidant damage by maintaining a balance between oxidants and antioxidants. 36 A shift in this balance associated with exposure to cigarette smoke, resulting either from an excess of oxidants or depletion of antioxidants, is referred to as oxidative stress, and has been suggested as a pathogenic mechanism in patients with COPD (Figure 1).8,9
The contribution of oxidative stress to COPD is thought to encompass a variety of mechanisms. For example, oxidative stress has been suggested to enhance lung inflammation via induction of redox-sensitive inflammatory transcription factors such as nuclear factor-κB (NF-κB) and activating protein-1 (AP-1), and subsequent stimulation of their cognate transcriptional programmes. 37 In addition, oxidative stress has been shown to increase neutrophil sequestration in the lung, enhancing lung inflammation and establishing a vicious cycle of increased oxidative stress and enhanced inflammation. 38 Oxidative stress has also been associated with protease/antiprotease imbalance 39 and increased alveolar cell apoptosis by inhibition of the VEGF receptor. 40 It has also been linked with direct DNA damage, stimulation of the release of mucus by airway epithelial cells, and impaired mucociliary clearance. 41
Inhibition of oxidative stress by MSC transplantation
Modulation by MSCs of the redox environment is a rapidly emerging area of interest. For example, the increased survival rate of lipopolysaccharide-induced lung injury rats after transplantation of bone marrow MSCs has been shown to be accompanied by decreased oxidative stress. 42 Moreover, reduction by MSCs of pulmonary levels of malondialdehyde occurs in parallel with increased synthesis of heme oxygenase-1, an enzyme with strong antioxidative stress and cytoprotective effects. 43 In addition, transplantation of bone marrow MSCs is known to decrease oxidative stress in the brain of a rat model of spontaneous stroke, 44 suggesting that MSCs may decrease oxidative stress in cigarette smoke-induced emphysema. Further studies are needed to understand the effects of MSCs on oxidative stress in emphysema, and the antioxidative mechanism of its action in alveolar cells.
Alveolar differentiative potential of transplanted MSCs in COPD
The beneficial role of transplanted MSCs in emphysema has been attributed in part to differentiation of MSCs into alveolar cells, although the exact type of cell is an area of controversy.14,45–48 Differentiation of MSCs into type I and/or type II alveolar epithelial cells has been reported in rat models of lipopolysaccharide- and cigarette smoke-induced emphysema 14 and bleomycin-induced lung injury.45–47 On a mechanistic level, Liu et al. 48 have shown that differentiation of MSCs into type II alveolar epithelial cells in a coculture system was associated with activation of the canonical Wnt signalling pathway.
Conclusions
At present, there are no therapies that can reduce the disease progression or mortality associated with COPD. Transplantation of MSCs represents a potentially promising therapy for COPD, and may involve modulation of inflammation, protease/antiprotease balance, apoptosis and oxidative stress, or the differentiation of MSCs into lung parenchyma cells. A major obstacle to the clinical application of MSCs in COPD is the dearth of data on the long-term safety of MSCs in patients with COPD. It should be noted, however, that a clinical trial has shown no infusional toxicity, serious adverse events, or attributable deaths in MSC-treated patients during a 2-year follow-up period. 25 Further larger scale clinical trials will be necessary, to more fully assess the efficacy and long-term safety of MSCs in patients with COPD. A second major challenge to the clinical application of MSCs in COPD is that the therapeutic schedule is not clear, and additional studies are warranted to ascertain the appropriate cellular dose, infusion rate and route of administration. A final challenge is the poor survival of MSCs and the low level of engraftment in host organs, 49 therefore, a pressing need exists for the development of approaches that increase survival and engraftment of MSCs in host organs. In summary, although several challenges exist, transplantation of MSCs represents a potentially promising therapy for COPD.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The development of this review was supported by a grant from the Applied Basic Research Project Fund of Yunnan Province, China (grant no. 2012FB106).