
Abstract
Background:
Soluble urokinase-type plasminogen activator receptor (suPAR) is positively correlated with immune system activity. Inflammation can promote the development of chronic obstructive pulmonary disease (COPD). Therefore, this study conducted a systematic review and meta-analysis to assess the association between suPAR levels and the pathogenesis of COPD, and further assess the exact clinical value of suPAR in COPD.
Methods:
PubMed, Excerpt Medica Database (Embase), Web of Science (WOS), and Cochrane Library databases were searched for studies that reported the value of suPAR diagnosis for adult COPD patients.
Results:
A total of 11 studies were included, involving 4520 participants. Both COPD patients with predicted forced expiratory volume in 1 s (FEV1)⩾80% [weighted mean difference (WMD) = 320.25; 95% confidence interval (CI): 99.79–540.71] and FEV1 < 80% (WMD = 2950.74; 95% CI: 2647.06–3254.43) showed higher suPAR level. The sensitivity and specificity of suPAR for diagnosis of COPD were 87% and 79%, respectively, and AUC was 84%. This can not only effectively identify acute exacerbation of COPD (AECOPD) in a healthy population (WMD = 3114.77; 95% CI: 2814.66–3414.88), but also has the potential to distinguish AECOPD from stable COPD (WMD = 351.40; 95% CI: 215.88–486.93). There was a significant decrease of suPAR level after treatment [WMD = –1226.97; 95% CI: –1380.91– (–1073.03)].
Conclusion:
suPAR as a novel biomarker has potential for early diagnosis of COPD and prediction of AECOPD. There is a potential correlation between the level of suPAR and the state of COPD, which may also indicate the early state and severity of COPD. When the suPAR level of COPD patients is further increased, the risk of acute exacerbation increases and should be highly valued. This also shows potential as a measure of treatment response, and as a guide to the clinical management in COPD.
The reviews of this paper are available via the supplemental material section.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by persistent airflow limitation and recurrent acute exacerbations, and is associated with chronic inhalation of noxious particles and gas-induced pulmonary inflammation.1,2 Acute exacerbation of COPD (AECOPD) is characterized by deterioration of the respiratory symptoms beyond normal daily variations, usually leading to adverse outcomes. 3 The World Health Organization predicts that, by 2030, COPD will be the third leading cause of death, and may rise to the fifth-largest leading cause of disability-adjusted life years.4,5 Accurate and timely diagnosis will provide a strong guarantee for screening high-risk groups and improving the clinical course and outcome of COPD. However, the biomarkers used to assist the diagnosis and prediction of COPD are still insufficient. 6
Soluble urokinase-type plasminogen activator receptor (suPAR) is a soluble form of the urokinase plasminogen activator receptor (uPAR), which is released by membrane-bound plasminogen activator, and is positively correlated with the activation of the immune system. 7 suPAR is found in various body fluids, including blood, urine, and cerebrospinal fluid. 8 It is expressed by endothelial cells, macrophages, monocytes, neutrophils, lymphocytes, and fibroblasts, and is upregulated by infection and pro-inflammatory cytokines. 8 suPAR can promote plasminogen activation, cell adhesion, chemotaxis, and immune cell activation. 9 In recent years, it has become a potential inflammation biomarker. 10 Airway inflammation plays an important role in the development of COPD. Inflammatory products are the main source of destructive and structural changes in the pathological process of COPD. 11 Previous studies suggest that serum suPAR may reflect the inflammatory process of COPD, and this increase may be particularly effective for patients with stages III and IV of the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD).12,13 Therefore, the level of suPAR has the potential to guide the diagnosis of COPD.
Biomarkers for COPD should be able to help clinical diagnose, determine the early state of the disease, predict acute exacerbation, and monitor responses to existing and new treatment strategies. This systematic review and meta-analysis aims to explore the clinical role of suPAR as an emerging biomarker in the diagnosis and prediction of COPD.
Materials and methods
All methods of this systematic review and meta-analysis analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.14,15
Data sources and searches
The review authors searched for medical literature before October 2019. The research was conducted in electronic databases including the Cochrane Library, PubMed, the Excerpt Medica Database (Embase), the Web of Science (WOS), and the reference lists from review articles, irrespective of publication date, status or language. The search was conducted with the following keywords: suPAR and COPD or AECOPD. Search strategies used in the Cochrane Library, PubMed, Embase, and WOS can be found in the Supplemental material.
This meta-analysis included studies that met the following criteria:
Adult patients with confirmed or suspected COPD or AECOPD (over 18 years of age).
The studies included the results of suPAR levels in patients with COPD or AECOPD, the diagnosis value of suPAR, the prediction value of suPAR for AECOPD, or the prediction value in COPD treatment effect. COPD or AECOPD was diagnosed based on the latest reference standard during the study, such as the GOLD criteria.
No publication date, status, or language restrictions were applied. Clinical original articles were included, whereas secondary studies, conference abstracts, editorials, and animal experiments were excluded.
Study selection
Two review authors (QH and HX) independently assessed the studies to be included based on the titles, abstracts, and keywords. If a study was found relevant to our topic, at least two reviewers further evaluated its full text to see if it met the inclusion criteria. In case of inconsistencies between the reviewers, a third reviewer (J Liu) was consulted. The authors consulted the original authors to further ensure the eligibility of a study, when additional information on the details of the results and methods or allocation concealment was needed. A study diagram was prepared to illustrate the entire literature research process and the selection of the studies.
Data extraction and quality assessment
The data were independently extracted by two review authors (TS and CZ) and the resulting differences were resolved by a third reviewer (J Liu). The extracted data included the lead author, publication year, country of origin, participant characteristics [age, sex, hospitalization, predicted forced expiratory volume in 1 s (FEV1%), FEV1/forced vital capacity (FVC%), smokers number, and pack-years for ever-smokers], the measurement of suPAR levels and the suPAR levels of COPD patients and control group for studies including the results related to the diagnosis value of suPAR for COPD. The extracted data included the optimal cut-off threshold, values for sensitivity, specificity, true-positive, true-negative, false-positive, false-negative, and the area under the receiver operating characteristic (ROC) curve (AUC). If data were missing, a letter was written to the authors to request the data. If there was no response to the letter after 4 weeks, an email was sent. If there was no response to the email, estimates were made based on available data and used. The outcomes that cannot be pooled or analyzed are described in the literature.
Two review authors (MZ and J Lu) independently applied the guidelines of PRISMA statement 16 to evaluate each involved study. The quality and bias of the included studies were assessed by two independent authors (MZ and J Lu). The Newcastle-Ottawa Scale (NOS) was used to assess the quality and bias of case control and cohort studies (Supplemental Table S1). 17 As for the cross-sectional design, the Agency for Healthcare Research and Quality (AHRQ) was used for the quality and bias assessment (Table S2). 18 If the included study contained the results of the diagnostic value of suPAR for COPD and the 2×2 contingency table, the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) was conducted to further assess the quality and bias (Table S3). 19 In the case of any inconsistencies, an agreement was reached through discussion between all of the authors. The summary tables showed in supplemental material showed the assessment of the risk of bias.
Data synthesis and analysis
Extracted data were analyzed using Stata SE 14.0 (Stata Corp; College Station, TX, USA). Based on the outcomes, forest plots were made to demonstrate the cumulative effect of suPAR. Continuous variables were expressed as weighted mean difference (WMD) with a 95% confidence interval (CI). The pooled effect size was calculated by the fixed effect model. When significant heterogeneity (p < 0.05, I2 ⩾ 50%) was observed, a randomized effect model was applied. Subgroup analysis and sensitivity analysis were conducted to explore the source of heterogeneity.
Spearman’s correlation coefficient was used to evaluate the threshold of the diagnosis value of suPAR. The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) were calculated. The accuracy of the diagnostic effects was evaluated by constructing a summary receiver operating characteristic (SROC) curve (AUC).
Heterogeneity was assessed by the Q test (significant heterogeneity was indicated by p < 0.05) and the I2 test (significant heterogeneity was indicated by I2 > 50%). Funnel plots were generated to investigate the effects of smaller studies (the trend of intervention effects estimated in smaller studies may differ from that estimated in larger studies, which may be due to reporting biases, methodological or clinical heterogeneity, or other factors).
20
If more than 10 studies are included, Egger’s test was prepared for publication bias.
21
The
Results
A total of 136 records were identified from the four electronic databases and the reference lists of review articles, with 70 remaining after the duplicates were removed. After screening the titles and abstracts, 34 articles were excluded. Of the 36 articles retrieved, 25 studies were excluded after full-text review because they did not meet the selection criteria. In summary, this systematic review and meta-analysis included 11 studies involving 4520 patients12,22–31 (Figure 1).

PRISMA flow diagram and exclusion criteria.
The characteristics of the included trials are presented in Table 1. Three of the included studies were case-control studies,12,22,23 six prospective cohort studies,25–29,31 one retrospective cohort studies, 24 and one cross-sectional study. 30 Most trials diagnosed COPD based on the GOLD criteria. Five studies included participants from the outpatient department,12,22,25,27,28 and four included participants from the respiratory medicine.23,26,29,31 In terms of pulmonary function, six studies included patients with predicted FEV1% ⩾80%,12,22,23,26–28 and another five studies reported patients with the predicted FEV1% < 80%.12,25,29–31 The studies reported that the smoking status of patients ranged from 28 to 53 packs per year.
Characteristics of included studies.

AECOPD, acute exacerbation of chronic obstructive lung disease; CC, case control study; COPD, chronic obstructive lung disease; CS, cross-sectional study; ED, emergency department; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GOLD, the Global Initiative for Chronic Obstructive Lung Disease; ICD-10, the International Classification of Diseases, 10th edition; NA, not available; OD, the Outpatient Department; PC, prospective cohort study; RC, retrospective cohort study; RM, Division of Respiratory Medicine; SCOPD, stable chronic obstructive lung disease.
①suPAR levels; ②diagnosis value of suPAR for COPD; ③value of suPAR for predicting COPD treatment effect; ④value of suPAR for predicting AECOPD.
The diagnosis value of suPAR in patients with COPD
In all, 10 studies used suPAR levels as the primary outcome.12,22,23,25–28,30,31 These studies provided the mean ± standard deviation (SD) of suPAR level and the number of subjects for the COPD patient group and the healthy control group. Among them, six studies included patients with predicted FEV1% ⩾ 80%, and five reported patients with predicted FEV1% < 80%. The randomized effect model presented that compared with the healthy group, the suPAR level of COPD patients was significantly increased (WMD = 1527.73; 95% CI: 763.78–2291.68; p < 0.001) (Figure 2). It was demonstrated that the elevated suPAR levels were effectively associated with a high risk of COPD.
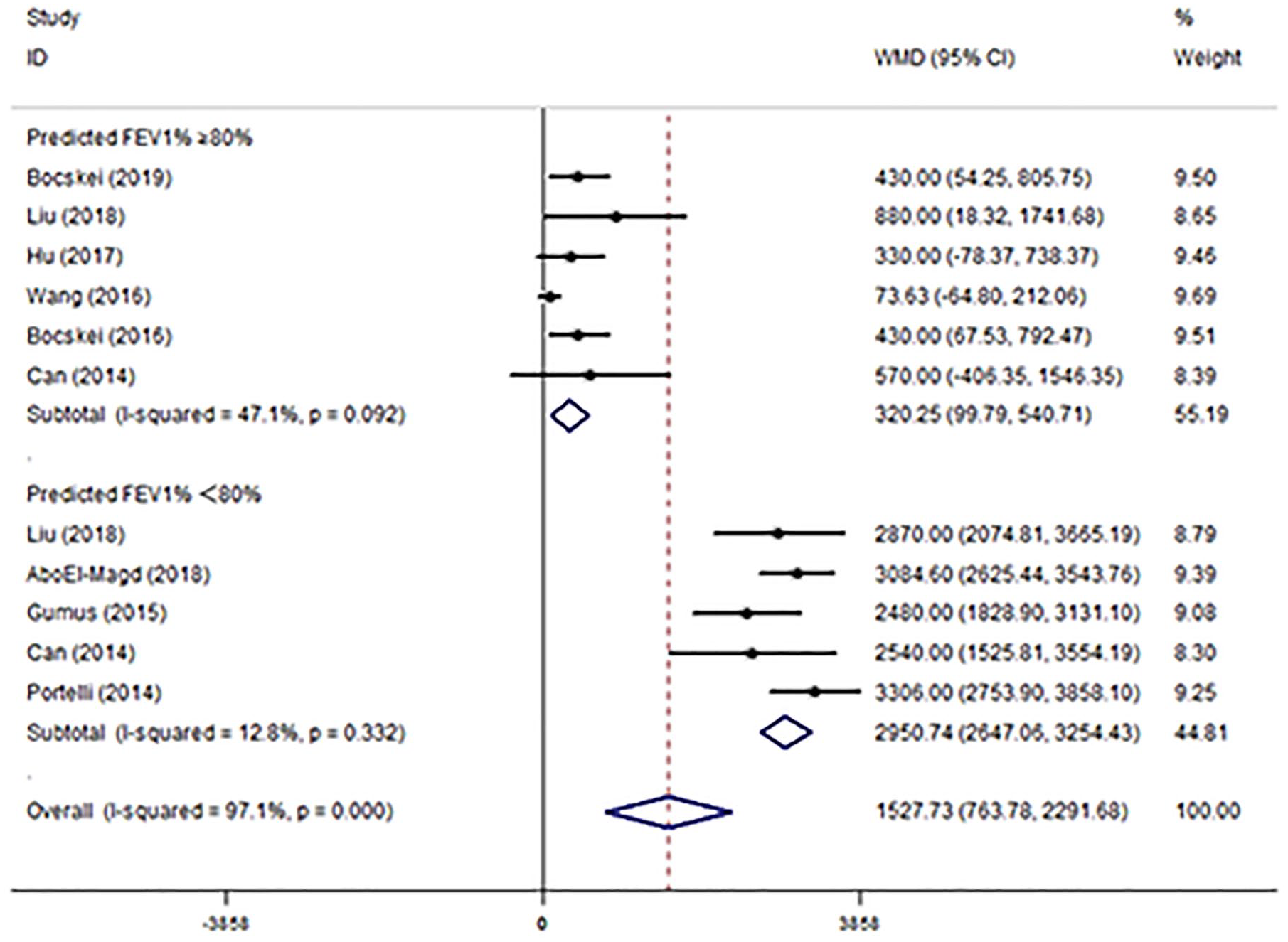
Forest plot of the suPAR level between COPD patients and healthy control.
In terms of the heterogeneity of the results (I2 = 97.1%; p < 0.001), we conducted a subgroup analysis based on the state of COPD. Compared with the healthy group, the suPAR level increased by 320.25 pg/ml in COPD patients with predicted FEV1% ⩾80% (WMD = 320.25; 95% CI: 99.79–540.71; p < 0.001), and the heterogeneity was I2 = 47.1% (p = 0.092). As for the patients with predicted FEV1% < 80%, the suPAR level increased by 2950.74 pg/ml (WMD = 2950.74; 95% CI: 2647.06–3254.43; p < 0.001), and the heterogeneity was insubstantial (I2 = 12.8%; p = 0.332) (Figure 2). Due to the different sample sizes of included studies, we generated funnel plots to investigate the effects of smaller studies. The result did not reveal evidence of statistical differences between the smaller trials and the larger trials (Figure S1). Egger’s test showed that the included studies were statistically unbiased (p = 0.060; Figure S2).
Four studies reported the results of the diagnosis value of suPAR.25,26,29,30 The pooled sensitivity of suPAR in the diagnosis of COPD was 0.87 [95% CI, 0.77–0.93; I2 = 66.01%, Q = 8.83 (p = 0.03)] and the specificity was 0.79 [95% CI, 0.71–0.85; I2 = 28.23%, Q = 4.18 (p = 0.24); Figure 3]. The PLR and NLR were 4.1 (95% CI, 3.0–5.6) and 0.17 (95% CI, 0.10–0.29), respectively, and the DOR was 24 (95% CI, 12–48). The AUC was 0.84 (95% CI, 0.81–0.87; Figure 4), indicating that suPAR has moderate diagnostic accuracy in COPD. In addition, there was no significant difference in threshold effect (Spearman correlation coefficient = 0.32; p = 0.68).
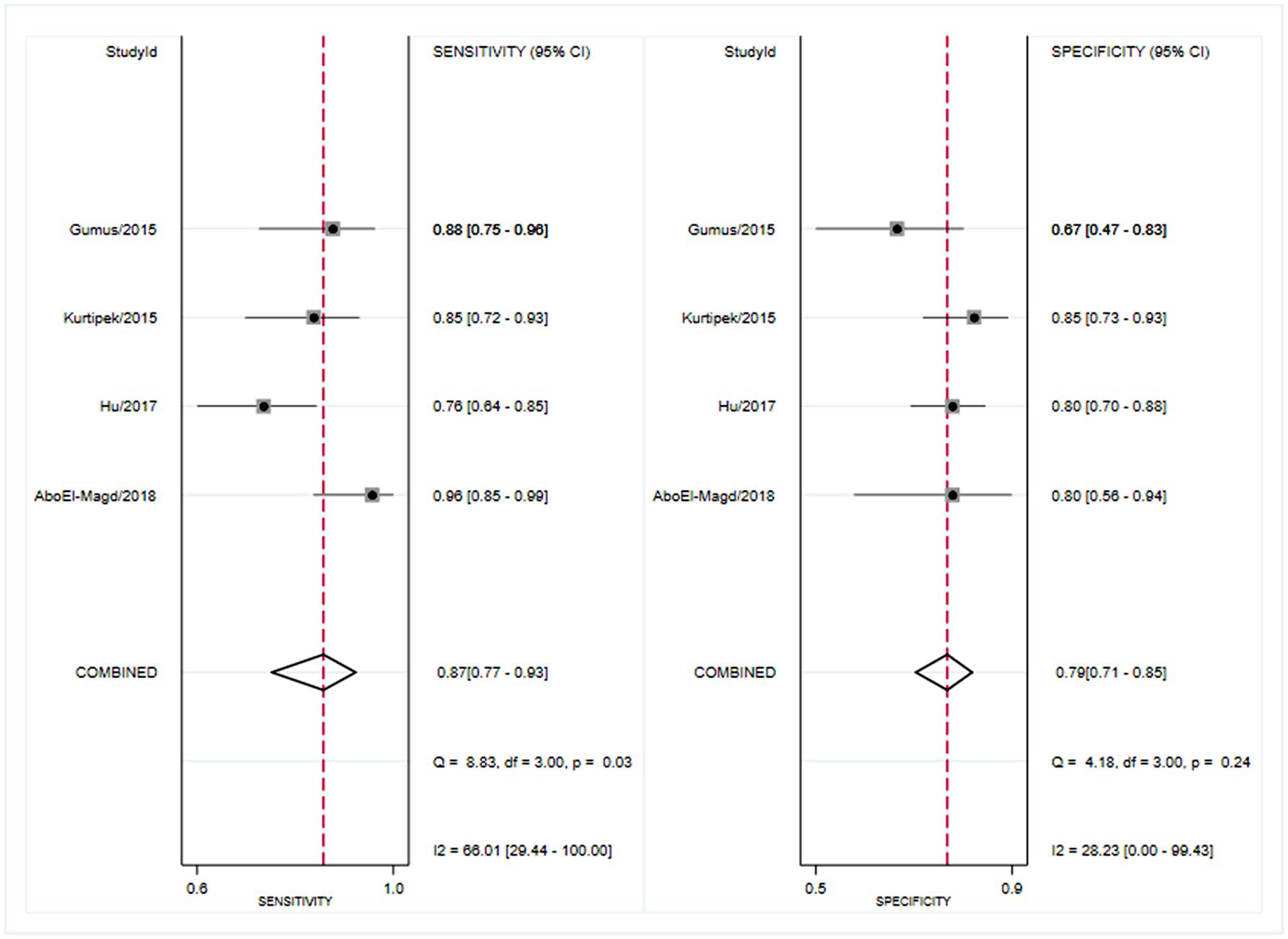
Forest plot of the sensitivity and specificity of suPAR for the diagnosis of COPD.

Summary receiver operating characteristics curve for studies evaluating the value of suPAR for the diagnosis of COPD.
The predictive role of suPAR in COPD patients
In terms of the prediction value of suPAR for AECOPD, six studies reported relevant results.22,24–26,29,30 Among them, four studies reported the value of suPAR in distinguishing AECOPD from stable COPD,22,24,26,29 and three reported the value in distinguishing AECOPD from healthy population.25,26,30 Compared with the stable COPD group, the level of suPAR increased by 351.40 pg/ml in AECOPD (WMD = 351.40; 95% CI: 215.88–486.93; p < 0.001), and no heterogeneity was found (I2 = 0.0%; p = 0.427). For the healthy population, suPAR levels increased notably, by 3114.77 pg/ml (WMD = 3114.77; 95% CI: 2814.66–3414.88; p < 0.001), and the heterogeneity was negligible (I2 = 0.0%; p = 0.825) (Figure 5). The results demonstrated that further increase in suPAR levels effectively indicates high risk of AECOPD and reflects the state of COPD.

Forest plot of the prediction value of suPAR level for AECOPD.
In terms of the prediction value of suPAR for treatment response, four studies reported suPAR levels in COPD patients before and after treatment.22,25,29,30 Compared with the pre-treatment suPAR level, there was a significant decrease after treatment [WMD = –1226.97; 95% CI: –1380.91– (–1073.03); p < 0.001], and no heterogeneity was obtained (I2 = 0.0%, p = 0.635). This suggests that monitoring suPAR levels can be helpful in evaluating COPD treatment response (Table 2).
The clinical role of suPAR for COPD patients.

AECOPD, Acute exacerbation of chronic obstructive pulmonary disease; CI, confidence interval; COPD, chronic obstructive lung disease; FEV1, forced expiratory volume in 1 s; sCOPD, stable chronic obstructive lung disease; suPAR, soluble urokinase-type plasminogen activator receptor; WMD, weighted mean difference.
Discussion
This meta-analysis found that suPAR, as a notable biomarker, has the potential to help diagnose and predict COPD patients. Elevated levels of suPAR were effectively associated with a high risk of COPD (WMD = 1527.73; 95% CI: 763.78–2291.68; p<0.001). And suPAR can also help diagnosis in the early stages of COPD. Compared with the healthy group, suPAR levels increased by 320.25 pg/ml in COPD patients with predicted FEV1% ⩾ 80%. Further investigation on the accuracy of suPAR in the diagnosis of COPD found that suPAR has a promising diagnostic value in COPD (SEN: 0.87, SPE: 0.79 and AUC: 0.84). As for the clinical value of AECOPD prediction, suPAR can not only effectively identify AECOPD from healthy population, but also has the potential to distinguish AECOPD from stable COPD. In addition, the results showed that suPAR can assess the treatment response of COPD, and the levels of suPAR decreased by 1226.97 pg/ml approximately after effective treatment.
Urokinase-type plasminogen activator (uPA) system is composed mainly of uPA, urokinase-type plasminogen activator receptor (uPAR) and urokinase-type plasminogen activator inhibitor (PAI-1). The latter play a major role in activating the immune system and inflammation.6,32 SuPAR is released by uPAR (the membrane-bound receptor for uPA). The researchers underlined that suPAR has an important impact on lung disease. Wang et al. demonstrated that uPAR levels in small airway epithelium of COPD patients were significantly higher than that of healthy controls, and also found that uPAR was significantly associated with the expression of vimentin. 33 The increase of uPAR level in COPD patients contributes to the activity of the epithelial-mesenchymal transition process, and uPAR is also associated with airflow limitation. The uPA system plays a critical role in the development and pathogenesis of COPD by inducing inflammation and tissue remodeling, including parenchymal destruction and small airway fibrosis.34–36 This indicates that suPAR has the potential to assist the clinical management of COPD patients.
Form the results of this meta-analysis, we found that suPAR was significantly correlated with the status and severity of COPD. Previous original studies have shown that serum suPAR may reflect the inflammatory process of COPD, and this increase is particularly effective in patients with stages GOLD III and IV.12,13 This is consistent with our results, and we found that patients with predicted FEV1% < 80% had a significant increase in suPAR levels, at 2950.74 pg/ml. However, in existing studies, the potential value of suPAR in early-stage diagnosis is unclear. We found that patients with stage GOLD I (predicted FEV1% ⩾ 80%) had a higher suPAR level of 320.25 pg/ml compared with the healthy population, which was statistically significant. Considering the importance of early prediction and diagnosis in improving the clinical course and outcome of COPD, 37 and the effective value of suPAR in predicting the severity of COPD, we suggest that suPAR can be a promising biomarker for patients with COPD.
Currently, biomarkers, including serum C-reaction protein (CRP), IL-6 and fibrinogen, are used routinely to assist the diagnosis of COPD. CRP is the first acute phase reactant discovered, and can be detected in serum as early as 4 h after injury.12,38 The study performed by Mahsuk Taylan et al. Indicated that CRP is a promising diagnostic biomarker for COPD. 39 The corresponding sensitivity and specificity were 82.3% and 72.6%, respectively, and the AUC was 80%. In our study, the AUC of suPAR used to diagnose COPD was 84%, showing better accuracy than CRP. In addition, suPAR also exhibited higher sensitivity and specificity (SEN = 87%, SPE = 79%) than CRP. This indicates that suPAR has an effective diagnostic value in COPD. Although suPAR has potential as an early biomarker and has a superior diagnostic tendency, considering that only four studies have reported the diagnostic accuracy of suPAR in COPD patients, more high-quality original studies are needed to prove it.25,29
COPD patients with acute exacerbation require longer hospital stays, higher costs, ICU admission, and even mechanical ventilation. In the worst case, a small number of patients may eventually die without remission. Previous studies have shown that early prediction and intervention of these COPD patients can reduce poor outcomes and mortality. 40 Therefore, it is important to assess and predict the severity of acute exacerbations in COPD patients.41,42 However, there is currently no consensus on the assessment and prediction of the severity of acute exacerbation. In this meta-analysis, we found that suPAR has the potential to predict acute exacerbation of COPD patients. As an early and effective biomarker, suPAR can not only distinguish AECOPD patients from healthy population, but also distinguish acute exacerbations from stable COPD. When the suPAR level of COPD patients is further elevated, the risk of acute exacerbation increased and should be highly valued. By comparing the suPAR level in the healthy control, COPD patients with early stage (predicted FEV1%⩾80%), patients with predicted FEV1% < 80% and AECOPD patients, we found that suPAR levels increased with the severity of COPD. This further indicates that suPAR levels are closely associated with the state of COPD.
As for the clinical value of suPAR in predicting treatment response, we found significant differences in suPAR levels before and after treatment in COPD patients. This suggests that suPAR has potential as a biological indicator of effective treatment. After treatment, the content of suPAR in COPD patients decreased by approximately 1226.97 pg/ml. This is consistent with the conclusion of the review conducted by Can et al., 43 which demonstrated that suPAR has the potential in the follow-up of COPD treatment. Indicating inflammation in COPD and assessing suPAR levels can play a key role in the evaluation of the inflammatory process in COPD. 43
For significant degree of heterogeneity, subgroup analyses revealed that the pulmonary function of COPD patients substantially affected the heterogeneity due to the association between suPAR and COPD. In the subgroup analysis, the heterogeneity in both of the predicted FEV1% ⩾80% subgroup and predicted FEV1% < 80% subgroup were insubstantial (I2 = 47.1%, p = 0.092 and I2 = 12.8%, p = 0.332, respectively). As the heterogeneity of the predicted FEV1% ⩾80% subgroup was I2 = 47.1%, we further conducted a sensitivity analysis to explore the source of heterogeneity. From the result of sensitivity analysis, it showed that the main source of heterogeneity derived from the study by Wang et al. (Figure S3). 27 When the study by Wang et al. was excluded from the analysis, I2 decreased to 0%. Compared with other included studies, Wang’s study further divided COPD population and healthy population into smokers and non-smokers subgroups. However, they did not clearly indicate the inclusion criteria for the subgroup, so the inclusion population of this study may be potentially different from other studies, which may lead to the increasing heterogeneity. As for the analysis of diagnosis value in COPD, only four studies reported relevant results. There are no significant threshold effects in diagnostic studies (Spearman correlation coefficient = 0.32; p = 0.68), but the cut-off value of suPAR can also account for the heterogeneity. High quality original research is still needed to prove this.
There are several limitations in the current meta-analysis. First, the level of suPAR is associated with a variety of diseases, including COPD and malignant tumors, kidney damage, and inflammatory bowel disease. This can lead to confounding factors that are difficult to evaluate in the included studies. Because the population included in this meta-analysis was COPD patients, combining the clinical symptoms of this population with suPAR levels to reduce the effects of confounding factors can still indicate the clinical value of suPAR for COPD patients. Second, because it is difficult to obtain original data for each study, we are unable to determine the optimal cut-off point for suPAR for the diagnosis of COPD. Third, only four studies reported the accuracy of suPAR in the diagnosis of COPD. Although this can also indicate the trend of suPAR diagnosis superiority, more original research is still needed. In addition, future studies in a larger series of patients and a control group composed of healthy population may reflect the inflammatory process of COPD patients based on plasma suPAR levels. Therefore, before being used in clinic, further study including more patients are needed to assess the suPAR level of COPD and AECOPD patients.
Conclusion
From the results of this systematic review and meta-analysis, suPAR as a novel biomarker has potential in early diagnosis of COPD and prediction of AECOPD. There is a potential correlation between the level of suPAR and the state of COPD, which may also indicate the early state of COPD. With further clinical research, the application of suPAR will contribute to clinical decision-making. When the suPAR level of COPD patients is further increased, the risk of acute exacerbation increases and should be highly valued. In addition, suPAR shows potential to measure the response of COPD therapy. Considering that there is currently no consensus on the assessment and prediction of COPD severity, and the importance of early diagnosis and prediction for treatment, suPAR should be considered for COPD.
Supplemental Material
Author_Response – Supplemental material for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, Author_Response for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Qiangru Huang, Huaiyu Xiong, Tiankui Shuai, Yalei Wang, Chuchu Zhang, Meng Zhang, Lei Zhu, Jiaju Lu and Jian Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, Reviewer_1_v.1 for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Qiangru Huang, Huaiyu Xiong, Tiankui Shuai, Yalei Wang, Chuchu Zhang, Meng Zhang, Lei Zhu, Jiaju Lu and Jian Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, Reviewer_2_v.1 for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Qiangru Huang, Huaiyu Xiong, Tiankui Shuai, Yalei Wang, Chuchu Zhang, Meng Zhang, Lei Zhu, Jiaju Lu and Jian Liu in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplemental_material – Supplemental material for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis
Supplemental material, Supplemental_material for The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis by Qiangru Huang, Huaiyu Xiong, Tiankui Shuai, Yalei Wang, Chuchu Zhang, Meng Zhang, Lei Zhu, Jiaju Lu and Jian Liu in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of the First Clinical Hospital of Lanzhou University, the first clinical medical college of Lanzhou University, Evidence-based Medicine Center of Lanzhou University, and all the authors who participated in this study.
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.