
Abstract
Background:
Despite the frequency and negative impact of low physical activity among patients with chronic obstructive pulmonary disease (COPD), little is known about how it persists and remits over time or the factors predicting new states of low physical activity. The aim of the study was to determine the probability of a transition between states of low and nonlow physical activity in a cohort of patients with stable COPD followed for 2 years. We also investigated different potentially modifiable factors to determine whether they can predict new states of low physical activity.
Methods:
We prospectively included 137 patients with stable COPD (mean age 66.9 ± 8.3 years). Physical activity was measured at baseline and at 1 and 2 years of follow up. Low physical activity was defined according to energy expenditure by cut-off points from the Fried frailty model. The likelihood of annual transition towards new states and recovery was calculated. We evaluated demographic, frailty, nonrespiratory, and respiratory variables as potential predictors, using generalized estimating equations.
Results:
At baseline, 37 patients (27%) presented with low physical activity. During the study period, a total of 179 annual transitions were identified with nonlow physical activity at the beginning of the year; 17.5% transitioned to low physical activity. In contrast, 34.3% of the 67 transitions that started with low physical activity recovered. Predictors of transition to new states of low physical activity were dyspnea ⩾2 (odds ratio = 3.21; 95% confidence interval: 1.20–8.61) and poor performance on the five sit-to-stand test (odds ratio = 4.75; 95% confidence interval: 1.30–17.47).
Conclusions:
The change between levels of low and nonlow physical activity is dynamic, especially for recovery. Annual transitions toward new states of low physical activity are likely among patients with dyspnea or poor performance on the five sit-to-stand test.
The reviews of this paper are available via the supplemental material section.
Introduction
Physical activity is defined as any body movement performed by the skeletal muscles that requires an expenditure of energy. 1 Patients with chronic obstructive pulmonary disease (COPD) usually have reduced daily physical activity,2,3 and approximately 36% achieve low levels of physical activity. 4
Self-reported low physical activity, generally evaluated in terms of overall activity or estimated time devoted to select activities (e.g. minutes of physical activity or sport), is a strong risk factor of hospitalization and mortality among patients with COPD.5,6 In addition, low physical activity is a determinant of frailty status,7–9 and recovery from low physical activity can increase the general health status in patients with COPD. 6
Despite the frequency and negative impact of low physical activity among patients with COPD, little is known about how a low physical activity state persists and remits over time or what factors predict new states of low physical activity. The current literature related to COPD has identified a cross-transversal association between low physical activity and both respiratory and nonrespiratory factors, such as dyspnea, the COPD assessment test (CAT), the number of exacerbations, 6 and cardiac dysfunction or muscle weakness, 10 among others. However, these determinants of low physical activity may differ from those that could predict low physical activity over time.
The objective of this study was to determine the probability of a transition between states of low and nonlow physical activity in a cohort of patients with stable COPD followed for 2 years. We also investigated different potentially modifiable factors to determine whether they can predict new states of low physical activity. The result of this study could contribute to an appreciation of the processes and dynamics that underlie the development of low physical activity over time. 11
Material and methods
Study design and participants
This was a longitudinal study. Patients with stable COPD were prospectively recruited from an outpatient pulmonary service at Morales Meseguer Hospital, Murcia, Spain. All study participants provided written informed consent, and the study protocol was approved by the institutional review board of the hospital, the Ethical Committee of Clinical Research of the General University Hospital (approval number: EST-35/13). Patients were included in this study if they fulfilled the following criteria: diagnosis of COPD according to the Global Initiative for COPD (GOLD) recommendations (forced expiratory volume in 1s (FEV1) to forced vital capacity post-bronchodilator ratio <70%), 12 stable stage without exacerbations in the previous 6 weeks, and age between 40 and 80 years. Patients with an unstable cardiac condition within 4 months of the start of the study were excluded, as were those with cognitive deterioration or unable to walk. Over a 1-year period, a consecutive sample of eligible patients was identified on a rolling basis from patient health examinations. A pulmonary physician assessed their eligibility for inclusion among all patients with stable COPD that attended their follow-up visits. Patients underwent examinations at baseline and annually for 2 years. The initial cohort included 137 patients. All of them participated in an annual follow-up program consisting of medical consultations including update of their medical treatments; none of the participants was involved in rehabilitation programs.
Measurements
The study data were obtained through interviews with patients at baseline (T0), 1 year (T1), and 2 years (T2) after the start of the study. At baseline, data on sociodemographic, nonpulmonary, pulmonary, and frailty variables were obtained for analysis as possible predictors of transitions between different states of physical activity (low and nonlow physical activity). The patient interviews were conducted by a pulmonologist. For follow-up visits, research staff contacted patients 1–2 weeks before each follow-up time point to schedule an interview if they were in a stable stage without exacerbations during the previous 6 weeks. The interview was conducted within a period of 4 weeks from the follow-up time point. The participants who were not interviewed within this time interval were removed from the study.
Outcome measure
Physical activity was assessed using a reduced version of the Minnesota Leisure Time Physical Activity Questionnaire (VREM) designed to assess the amount and quality of physical activity performed in free time (i.e. leisure and moderately strenuous activities at home), such as working in the garden, walking, sports or dancing, climbing stairs, or going shopping on foot. From these activities, the energy expended during 14 days was calculated and the outputs were categorized in four different grades of physical activity: sedentary (energy expenditure <1250 metabolic equivalent of task (METS)-min/14 days), moderate (energy expenditure between 1250 and 2999 METS-min/14 days), high (energy expenditure between 3000 and 4999 METS-min/14 days) and very high (energy expenditure >5000 METS-min/14 days). 13 Moreover, the average kilocalorie expenditure per week was obtained using standardized algorithms and the results were also categorized into two levels: low and nonlow physical activity. For this last classification, we used the criteria from the model of frailty proposed by Fried to define low physical activity. 14 This model defined low physical activity as an energy expenditure of <383 Kcals per week for men and <270 Kcal per week for women.
Baseline measures
We selected several variables from the literature as covariates based on their potential association with physical activity related to COPD. These can be classified into four domains: sociodemographic, nonpulmonary, pulmonary, and frailty variables. Sociodemographic variables were age (years), sex, and education level (no formal education, primary school, secondary school, and university). The nonpulmonary variables were body mass index (BMI), number of comorbidities, presence of heart disease, diabetes, and symptoms of depression, physical activity level, quadriceps strength, 6-minute walk test (6MWT), and five sit-to-stand (5STS) test. Pulmonary variables were smoking pack-years, current smoker, dyspnea associated with activity, health status, total number of moderate and severe exacerbations in previous year, and percent of predicted FEV1. Frailty variables were unintentional weight loss, exhaustion, slow walking speed, and low handgrip strength.
These variables were obtained through different methods. Patients were measured and weighed to obtain the BMI (kg/m2). We reviewed the patient’s medical history to obtain the smoking pack-years, current smoker, number of comorbidities, total number of moderate (use of corticosteroids or antibiotics) and severe exacerbations (with hospitalization) in the previous year, and presence of heart disease and diabetes. Using questionnaires, we measured the level of dyspnea based on the modified British Medical Research Council (mMRC), 15 health status assessed by the CAT, 16 physical activity level by the VREM, 13 and depression was assessed by the depression subscale of the Hospital Anxiety and Depression Scale (HADS), with probable depression considered when the total score was ⩾11. 17 To assess pulmonary function, each patient underwent spirometry with a Master Scope Spirometer (version 4.6; Jaeger, Würzburg, Germany) according to the American Thoracic Society guidelines. 18 Quadriceps strength was assessed on the dominant side using a hand-held dynamometer (KERN MAP 80K1). 19 The 6MWT was performed indoors along a straight, flat, 30-m walking course supervised by two well-trained nurses (mean experience 19 years) according to American Thoracic Society guidelines. 20 The 5STS required participants to rise from a chair with their arms across their chest five times. 21 Scores ranged from 1 to 4 with a score <2 points considered a poor performance. 22 Frailty variables were obtained according to the Fried phenotype model.14,23
Statistical analysis
Descriptive statistics were used to characterize the cohort at baseline. Physical activity level was calculated annually. Among the participants with nonlow physical activity at baseline, we calculated the percentage presenting with low physical activity during at least one of the two subsequent measurements. Similarly, we calculated the percentage of participants who presented low physical activity at baseline and nonlow physical activity in subsequent measurements.
We analyzed data for all 1-year transitions available during the 2 years of the study. A 1-year transition was defined as a change in the level of physical activity between a given year and the following year. The data were not available when a participant was lost due to abandonment or death before the subsequent year. Next, we applied generalized estimating equations and grouped multiple observations in the same individuals to determine the effects of potential predictor variables on the 1-year likelihood of transitioning from the state of nonlow physical activity to low physical activity. For these analyses, we constructed several models: model 1 included only the sociodemographic variables and BMI; model 2 included the nonpulmonary, pulmomary, and frailty variables after adjusting for age, sex, education level, and BMI; and model 3 was simultaneously adjusted for all significant (p < 0.10) sociodemographic, nonpulmonary, pulmonary, and frailty variables. All of these models provided odds ratios for low physical activity. All analyses were performed using Statistical Package for the Social Sciences (SPSS) version 19.0 (IBM SPSS, Chicago, IL, USA).
Results
Participants
At baseline, a total of 137 patients were included. Overall, 37 (27.0%) patients had a low physical activity level; 36 (97.3%) of them were sedentary and 1 (2.7%) showed a moderate level of physical activity. Patients with low and nonlow physical activity levels had similar pulmonary and nonpulmonary characteristics except for the level of physical activity (Table 1).
Characteristics of the study population by physical activity group at baseline (n = 137).

Values are given as n (%) or mean (±standard deviation).
5STS, five sit-to-stand test; BMI, body mass index; CAT, COPD assessment test; FEV 1 , forced expiratory volume in 1 s; HAD-D, Hospital Anxiety and Depression Scale; mMRC, modified British Medical Research.
During follow up, 127 (92.7%) patients remained in the study at T1, and 119 (86.9%) remained at T2. Of those lost to follow up at T2, 6 (4.3%) died, 8 (5.8%) dropped out because of lung cancer, and 4 (2.9%) chose not to continue. No patients were removed due to unstable stage or exacerbation close to any follow-up visit. The patients lost during follow up were not significantly different in most characteristics from those who continued throughout the study (age, p = 0.843; sex, p = 0.858; heart disease, p = 0.697; and %FEV1, p = 0.137). However, patients lost to follow up had more depression (p = 0.004), more severe dyspnea (p = 0.016), and higher CAT scores (p = 0.003).
Rates and probabilities of a transition at 1 year
Of the 100 patients who presented nonlow physical activity at baseline, 25 (25.0%) experienced at least one episode of low physical activity during the follow-up period. Of the 37 patients who had low physical activity at baseline, 17 (45.9%) had nonlow physical activity at least once during the follow-up period and 20 (54.1%) had low physical activity during the 2 years of study. Considering all of these trajectories, low physical activity occurred in 17 (45.9%) and 20 (54.1%) patients at T1 and T2, respectively.
During the 2 years of follow up, a total of 246 annual transitions occurred between low or nonlow physical activity (179 of them started from nonlow physical activity). A total of 92 and 87 transitions of 179 from nonlow physical activity ocurred in the first and second years, respectively. For each year there was a similar percentage of transitions to low physical activity (17.6% and 17.4%). Based on these available transitions (n = 246), we calculated the 1-year probability of a transition between low and nonlow physical activity (Figure 1). Of the transitions with initial nonlow physical activity at baseline, 17.5% transitioned to low physical activity the following year. In contrast, 34.3% of transitions with low physical activity at the beginning ended with nonlow physical activity level the next year and 65.7% remained with low physical activity.
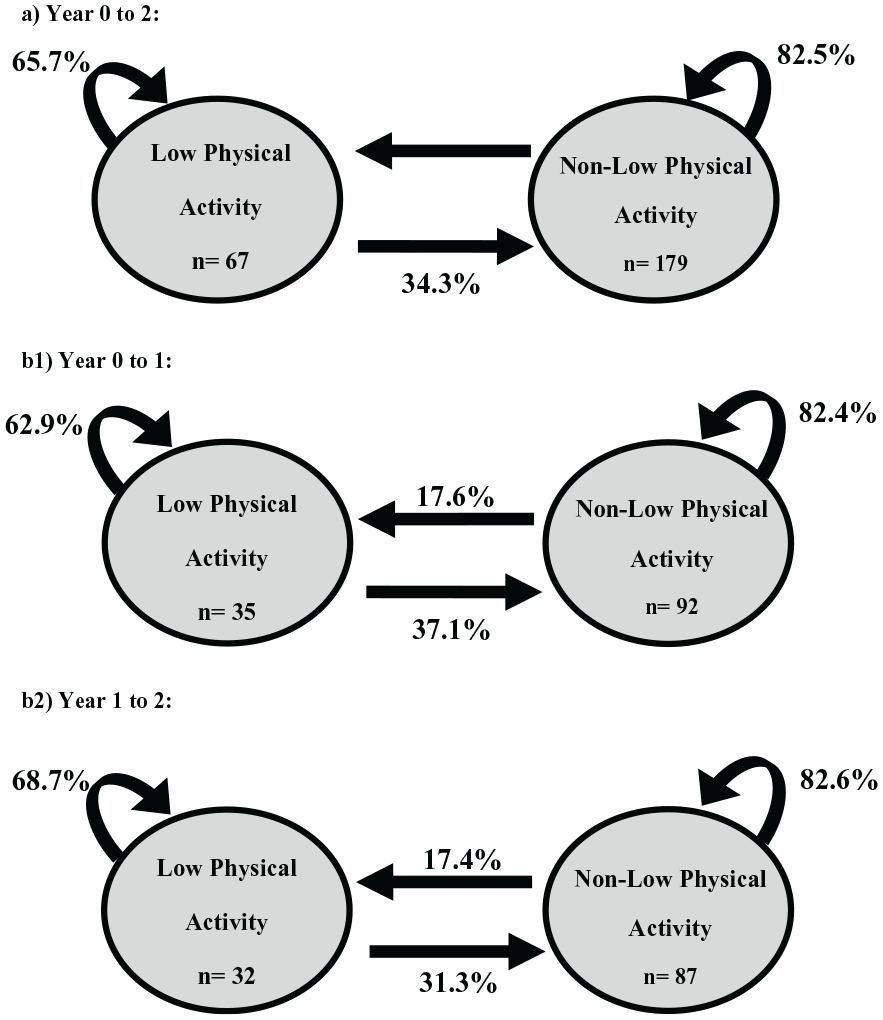
The 1-year probabilities of transition between the states of low or nonlow physical activity levels during 2 years of follow up (a), 0–1 years (b1), and 1–2 years (b2).
Predictors of the transition to low physical activity
We identified 179 1-year transitions in which the participant presented nonlow physical activity at the beginning of the annual transition. Table 2 shows the results of the three multivariate models testing factors that may be associated with the transition to low physical activity compared with maintaining a state of nonlow physical activity. Model 1, which included sociodemographic variables and BMI, suggested that higher age increased the likelihood of having a new episode of low physical activity the following year. Model 2, which included each of the pulmonary, nonpulmonary, and frailty predictors, adjusted by the variables of model 1, showed that new states of low physical activity were positively associated with being a current smoker, having depressive symptoms, higher CAT scores, number of exacerbations, dyspnea ⩾ 2, and 5STS ⩽ 2, and negatively associated with weak handgrip strength. Nevertheless, in model 3, which was adjusted for all significant variables from models 1 and 2, only one pulmonary variable (dyspnea ⩾ 2) and one nonpulmonary (5STS < 2) variable were identified as independent predictors of a new states (i.e. transition) of low physical activity.
Multivariate regression models showing the predictive strengths of factors associated with a transition to low physical activity from nonlow physical activity in the subsequent year (n = 179 1-year transitions) a .
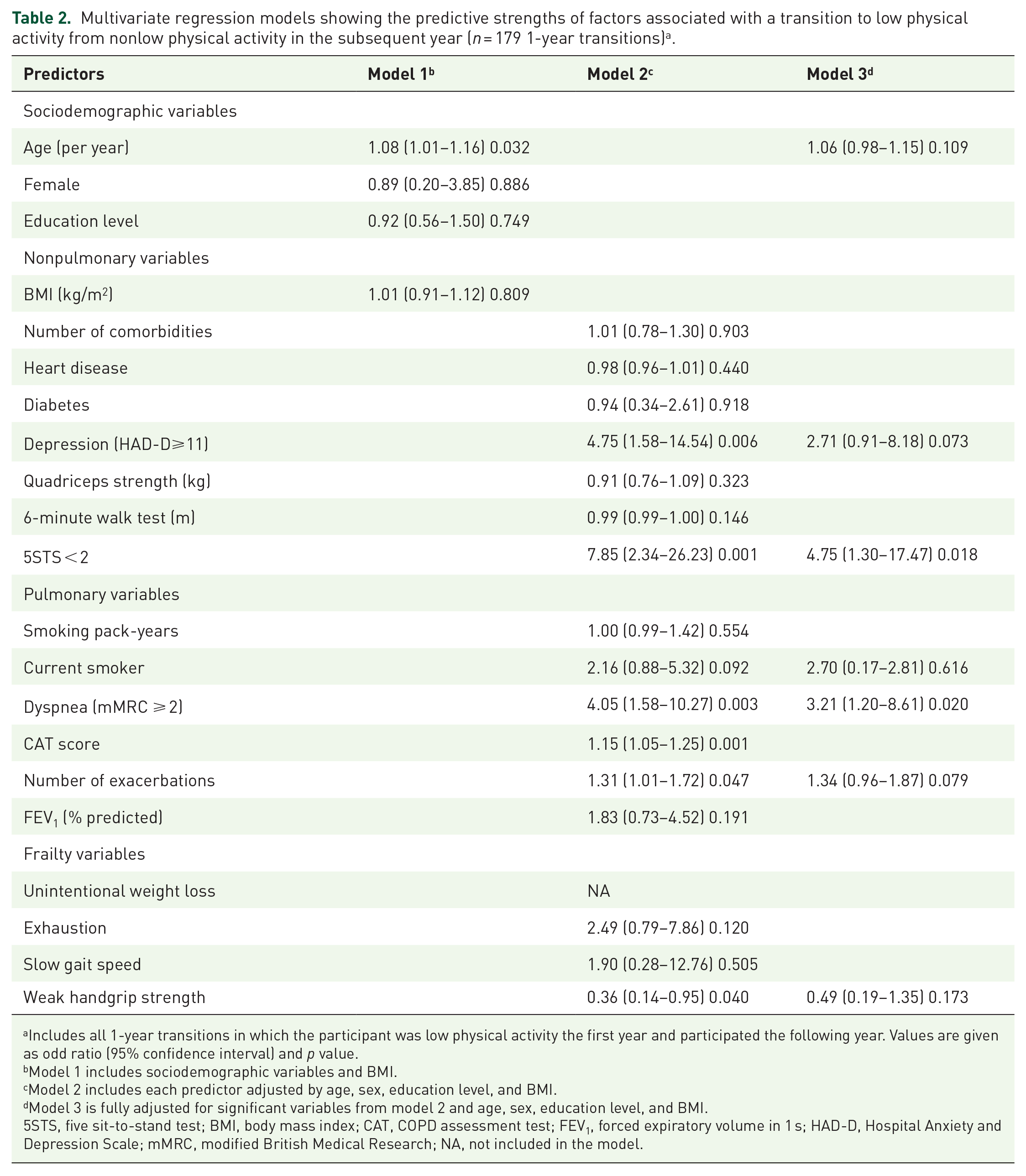
Includes all 1-year transitions in which the participant was low physical activity the first year and participated the following year. Values are given as odd ratio (95% confidence interval) and p value.
Model 1 includes sociodemographic variables and BMI.
Model 2 includes each predictor adjusted by age, sex, education level, and BMI.
Model 3 is fully adjusted for significant variables from model 2 and age, sex, education level, and BMI.
5STS, five sit-to-stand test; BMI, body mass index; CAT, COPD assessment test; FEV1, forced expiratory volume in 1 s; HAD-D, Hospital Anxiety and Depression Scale; mMRC, modified British Medical Research; NA, not included in the model.
Discussion
In our study, we analyzed the likelihood that patients with COPD experience annual transitions between states of low and nonlow physical activity, as well as which factors could predict a new states of low physical activity. Our results showed that transitions to new states of low physical activity occurred annually in almost a fifth of patients, and the most relevant independent predictors were dyspnea ⩾ 2 and poor performance on the 5STS test. In addition, a third of the annual transitions with low physical activity at the beginning of the year finished with recovery from that state. All of these results suggest that the nature of the physical activity level is dynamic in patients with COPD, especially for recovery from a low level of physical activity.
The results of our study suggest that the transition to a state of low physical activity is more likely in patients with dyspnea ⩾ 2 or a poor performance on the 5STS test. A possible explanation for this result is that the perception of dyspnea ⩾2 could serve as a self-protective function in patients with COPD, leading to deconditioning of the musculature, and thus further inactivity and a subsequent low level of physical activity.24–26 On the other hand, the relevance of the 5STS test could be that the performance of this test is determined by the muscle strength in the lower limbs,27,28 which is relevant for the realization of physical activity. In this sense, the weakness of the peripheral musculature in patients with COPD has been recognized to also contribute to the reduction in the level of physical activity.28,29 Along this line of reasoning, other authors have found that handgrip strength, which is a recognized indicator of the general strength of patients with COPD, is also related to a low level of physical activity. 30 For this reason, it was unexpected that the handgrip strength was not significant in our final model. This relevant relationship could have been obscured by categoritzation of handgrip strength according to cut-off points from the fragility model 14 and by adjusting for other variables that were more important in the final model.
Our results regarding dyspnea are consistent with those reported in previous studies. Esteban and colleagues found that COPD patients with lower levels of physical activity had more dyspnea than those who had a higher level of physical activity after a 5-year follow up. 31 Similarly, Hegendörfer and colleagues found a strong association between low physical activity and dyspnea, regardless of lung function. 32 Regarding the 5STS test, our results are consistent with those of Yu and colleagues, who found a similar relationship between a lower 5STS measured in 30 s and low physical activity in the population with COPD. 33
Despite the importance and impact of physical activity measured as part of the frailty index in patients with COPD, to the best of our knowledge, this is the first study that describes the longitudinal evolution and annual transience between the different states of physical activity (low versus nonlow level) in adults with COPD. Previous studies found significant changes in physical activity in patients with COPD after 3 years of follow up. 10 However, our study adds that changes in physical activity levels are frequent in shorter periods of time and the evolution dynamic. Nevertheless, more studies are needed, for example, comparing patients with COPD and patients without COPD in relation to the transience of physical activity.
Implications for practice and research
As the state of physical activity of patients with COPD is dynamic, it is advisable to evaluate it annually. Practices that permanently classify a subject in a specific physical activity level can give rise to false positives or negatives over time. Both severe dyspnea associated with exertion and poor performance on the 5STS test are potentially modifiable factors. Both factors can be improved by physical rehabilitation programs in patients with stable COPD34–36 and by a reduction in the number of hospital admissions 37 and mortality. 38 Therefore, the early recognition of a deficit in any of these factors in patients could benefit from these programs in order to facilitate their recovery or preserve a good state of physical activity. 35
Because all predictive factors were only measured at baseline, a more longitudinal analysis is needed to evaluate whether associations between low physical activity and dyspnea or poor performance on the 5STS test could also be observed concurrently in individual patients over time. This type of analysis could further reveal whether there is a synchronous association between changes in physical activity and changes in dyspnea and 5STS score, or alternatively whether changes in dyspnea and 5STS score can be influenced by the state of physical activity.
Strengths and limitations of the study
This study has several strengths. First, this was a longitudinal study. The main advantage of longitudinal analyses is that changes in patients can be analyzed individually. In addition, it allows measurement of the prevalence of physical activity in more than one moment in time. Our evaluation of the data from the three combined time points could also have provided a more realistic estimate of the prevalence, which could have strengthened the results. Second, our models included a variety of factors previously identified in the literature as factors related specifically to physical activity in patients with COPD. In addition, standardized and previously validated questionnaires were used, as well as objective measures that allowed comparisons with other studies.
Our study also has several limitations. First, we included a variety of possible predictive factors for physical activity, but could be other factors not included in our model that could have further improved its predictive power (e.g. the number of medications, participation in rehabilitation programs).39,40 Additionally, despite the fact that many of our predictive factors may vary over time, only baseline values were available. Therefore all covariates in our models were independent of time. Second, although measurements were made at three time points (once a year) to determine the course over time, it is likely that additional transitions occurred between these time points. However, the time points for the three measurements were chosen specifically to obtain optimal measurements of possible changes in the level of physical activity. Though little is known about the patterns of change between the different levels of physical activity, we expect that most of these changes will occur in the first year; therefore, we performed the measurements at 1-year intervals as described previously. 33 Finally, due to the small number of women in the cohort, care must be taken when generalizing the results.
Conclusion
Our study has shown that a low level of physical activity is common in patients with COPD, and that annual transitions to new states of low physical activity are more likely among patients with dyspnea or poor performance on the 5STS test. We also reported that change between levels of low and nonlow physical activity is dynamic in patients with COPD, and that a significant percentage of patients could recover from a low level of physical activity.
Supplemental Material
Author_response_1 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Author_response_1 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_2 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Author_Response_2 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study byMaría Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_3 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Author_Response_3 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Reviewer_1_v.1 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Reviewer_1_v.2 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.3 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Reviewer_1_v.3 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study
Supplemental material, Reviewer_2_v.1 for Patterns and predictors of low physical activity in patients with stable COPD: a longitudinal study by María Piedad Sánchez-Martínez, Roberto Bernabeu-Mora, Jose Antonio García-Vidal, Josep Benítez-Martínez, Silvana Loana de Oliveira-Sousa and Francesc Medina-Mirapeix in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors wish to thank their patients, and the personnel of the hospital unit, for their cooperation during the course of this study.
Authors’ contributions
The study conception and design was developed by RB-M, FM-M and MPS-M. Statistical analysis was conducted by FM-M, RB-M, and MPS-M. The manuscript was drafted and revised by RB-M, FM-M, MPS-M, JAG-V, SLO-S and JB-M.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AstraZeneca Pharmaceutical Spain, S.A. funded manuscript translation, from a first version in Spanish and had no role in study design, data collection and analysis, decision to publish or writing of the manuscript.
Conflict of interest statement
The corresponding author, on behalf of all authors, hereby declares and states the absence of any eventual or potential competing interest (neither financial nor nonfinancial).
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.