
Abstract
Background:
Although the six-minute-walk test (6MWT) has been used to predict chronic obstructive pulmonary disease (COPD) exacerbations, additional research is necessary to identify more rapid, simpler tests that are directly associated with exacerbations, such as the five-repetition sit-to-stand (5STS) test and 4-m gait speed (4MGS) test.
Aims:
To determine the ability of the 5STS and 4MGS tests in predicting severe exacerbations in stable COPD over the following year, and to assess the ability of the best prognostic test to identify patients at high risk of hospital admission correctly.
Methods:
This prospective study included 137 patients with stable COPD. Multiple logistic regression models were constructed to assess whether the 6MWT, 5STS, and 4MGS tests were associated with severe exacerbations in the year following the test. Receiver-operating characteristic curves and the area under the curve (AUC) were evaluated to determine the accuracy of each test for identifying patients with severe exacerbations.
Results:
Scores of <350 m for the 6WMT and ⩽2 for the 5STS test were associated with severe exacerbations in the model adjusted for age and the number of exacerbations in the previous year. The 5STS test and the 6MWT had very similar predictive and discriminative abilities. Odds ratios were 3.20 (95% confidence interval [CI] 1.14–8.96) and 3.84 (95% CI 1.14–12.94) and AUCs were 0.793 (95% CI 0.704–0.882) and 0.783 (95% CI 0.686–0.879), respectively.
Conclusions:
The 5STS test predicted the risk of severe exacerbation within the following year among patients with COPD. The 5STS test could replace the 6MWT for identifying patients at high risk of hospital admission.
Introduction
Exacerbations are frequent in chronic obstructive pulmonary disease (COPD). Patients with this disease experience between one and four exacerbations per year. 1 Exacerbations are characterized by persistent worsening of respiratory symptoms, which accelerate the decline of pulmonary function. 2 Often, this decline does not completely resolve,1,3 and it lowers the quality of life. 4 Consequently, COPD exacerbations are responsible for a large proportion of healthcare costs, particularly severe exacerbations that result in hospital admission. 5
Due to the frequency and impact of COPD exacerbations, a key objective in managing COPD in clinical practice is to identify factors associated with a high risk of exacerbations.1,6,7 The most reliable predictor of moderate to severe exacerbations is the history of exacerbations in previous years.3,8 Other predictors include advanced age and clinical characteristics, such as a reduced forced expiratory volume in 1 s (FEV1), dyspnea, the number of comorbidities, and exercise capacity.9–12
The six-minute-walk test (6MWT) has been widely used to assess exercise capacity and predict COPD exacerbations.10,13–15 A recent systematic review suggested that, in the 6MWT, shorter walking distances indicated a high risk of severe and moderate COPD exacerbations, in which a severe exacerbation resulted in hospital admission. 10 Some studies found that a walking distance <350 m (or proxy) was an effective cut-off point for predicting exacerbations.13,14
Despite the relevance of the 6MWT, pulmonologists do not typically employ this test in the clinic, due to time, equipment, and space constraints.10,16 Consequently, over the past few years, researchers have developed and validated faster, simpler tests, such as the five-repetition sit-to-stand (5STS) test and the 4-m gait-speed (4MGS) test for determining exercise capacity.17–19 Nevertheless, few studies have directly associated simple exercise tests with COPD exacerbations.10,20,21 Further research is necessary to validate the predictive properties of these simple tests and to compare these properties to those of the 6MWT.10,20
We previously explored associations between the 5STS and 4MGS tests and the 6MWT. We identified specific cut-off points for these tests that could identify patients with COPD that were likely to perform poorly in the 6MWT (<350 m). 17 However, the validity of these cut-off points for predicting exacerbation has not been reported. The present study aimed to determine the ability of the 5STS and 4MGS tests to predict severe exacerbations among patients with stable COPD over the following year. We also compared these tests to the 6MWT in their predictive abilities and their accuracy in identifying patients at high risk of hospital admission.
Materials and methods
Study design and participants
This prospective observational study included a consecutive sample of eligible patients with stable COPD that visited the Meseguer Hospital, Murcia, Spain, between January and December 2015. All study participants provided written informed consent. The study protocol was approved by the institutional review board of the hospital, called the Ethical Committee of Clinical Research of the General University Hospital (approval number: EST-35/13). Patients were included in this study when they fulfilled the following criteria: a diagnosis of COPD, according to the global initiative for chronic obstructive pulmonary disease (GOLD) 22 recommendations; a ratio <0.7 of FEV1/forced vital capacity, post-bronchodilator; 23 a stable disease stage, with no exacerbations in the prior 3 months; and aged between 40 and 80 years. Patients were excluded when they had an unstable cardiac condition within 4 months of the start of the study; cognitive deterioration; or were unable to walk. A pulmonary physician assessed eligibility for inclusion. The included patients were measured at baseline (T0) and at one year after the tests (T1).
Data collection
Outcome measure
The primary outcome measurement was a severe COPD exacerbation during the year following the baseline measurements. A severe exacerbation was defined as an increase in at least two of three specified symptoms: breathlessness, sputum volume, and sputum purulence, which required an urgent emergency department visit and hospital admission. 22 Severe exacerbations were self-reported by participants at T1.
Potential predictive factors
We selected 13 sociodemographic and clinical variables from the literature, based on their potential association with COPD exacerbations. In addition, we evaluated three physical performance tests, including the 6MWT, the 5STS test, and the 4MGS test. All tests were conducted at T0.
Sociodemographic characteristics included age (years) and sex. The clinical measures were: current smoking status (yes/no); body mass index (kg/m2); the number of comorbidities (measured with a functional comorbidity index); 24 the number of moderate or severe exacerbations in the prior year; the grade of dyspnea [measured with the modified British Medical Research Council (mMRC) scale]; 25 a COPD assessment test (CATTM); 26 two symptoms of chronic bronchitis (bronchial mucus hypersecretion and a daily cough); the resting oxygen saturation (SpO2), measured with a pulse oximeter; the FEV1 (L), measured with post-bronchodilator spirometry (MasterScope Spirometer, version 4.6; Jaeger, Würzburg, Germany), according to the American Thoracic Society guidelines; 27 and finally, an index GOLD stage. 22
To test physical performance, we administered three tests. The order of performance was based on randomization to avoid measurement bias. The 6MWT (measured in meters) was conducted indoors, along a flat, straight, 30-m walking course. The test was supervised by two well-trained nurses, and each patient received standard encouragement during the test, according to American Thoracic Society guidelines. 28 The results were categorized into two groups (<350 m or ⩾350 m); this cut-off score was established previously, 13 and <350 m was considered poor physical performance. The 5STS test measured the time (seconds) taken to stand five times from a sitting position, as rapidly as possible. The 4MGS test measured the time (seconds) taken to cross a 4-m line at a typical walking speed. The latter tests were performed according to the National Institute on Aging protocol for the short physical performance battery (SPPB). 29 All data were rated to obtain an ordinal variable (score 0–4), in which a higher score indicated greater functional status, based on Guralnick et al. 30 In addition, for each test, we classified patients into two groups, based on specific cut-off scores established in a previous study for identifying patients with a poor 6MWT. The cut-off scores were ⩽2 for the 5STS test, and ⩽3 for the 4MGS test. 17
Statistical analysis
Descriptive data are expressed as the mean ± standard deviation (SD) or the percentage, as appropriate. Comparisons between groups for descriptive summaries were performed with an analysis of variance.
Multiple logistic regression models were constructed, and the results are expressed as the odds ratio (OR) and 95% confidence interval (CI). In the first stage, we examined associations between sociodemographic or clinical characteristics and severe COPD exacerbations in univariate logistic regression analyses (unadjusted and adjusted for the total number of exacerbations in the prior year). Then, the factors that showed significance (p < 0.05) in the univariate adjusted models were combined in a multivariate model with the enter method. The goodness of fit of the models was assessed with the methods described by Hosmer and Lemeshow. 31 In the second stage, we examined the association between each physical performance test (6MWT, 5STS, and 4MGS) and the occurrence of severe exacerbations in the year after T0. These logistic regression models were either unadjusted or adjusted with the significant factors identified in the previous multivariate analysis.
We constructed receiver-operating characteristic (ROC) curves to assess whether the physical performance tests could improve the accuracy of identifying patients most likely to experience severe COPD exacerbations. ROC curves were constructed with the predicted probabilities from the 6MWT and 5STS test. The ROC curves were adjusted, respectively, with the significant factors identified in the previous multivariate analysis. We then calculated the area under the ROC curve (AUC).
We considered that a minimal required sample size of 137 was sufficient for a maximum of four factors in the model, with the recommended 10 events (exacerbations) per variable, and an estimated 25% of severe exacerbations. All analyses were performed with the SPSS statistical software program (SPSS version 23.0; IBM SPSS, Chicago, IL, USA).
Results
Participants
Of the 147 patients with COPD initially enrolled, 10 failed to meet our study inclusion criteria. Therefore, 137 patients were finally included in our patient cohort at baseline (Table 1).
Baseline characteristics of the study population (n = 137 patients with COPD).

Data are reported as the mean (±standard deviation), unless otherwise stated.
Moderate or severe exacerbations.
4MGS, 4-m gait speed; 5STS, five-repetition sit-to-stand; 6MWT, six-minute walk test; CAT; chronic obstructive pulmonary disease assessment test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; GOLD, global initiative for chronic obstructive lung disease; mMRC, modified British Medical Research Council scale; s, seconds; SpO2, resting oxygen saturation.
At this time, the entire cohort had a mean age of 67 years; most subjects were men (87.6%); and 29.9% were current smokers. The majority of subjects were GOLD stage D (57.7%).
At the T1 follow-up, 127 (92.7%) patients remained in the study. Of these, 24 patients (23.30%) experienced severe exacerbation in the year following T0: 12 in the first semester and 12 in the second semester. Another 10 patients were lost to follow-up: three died, one had lung cancer, one had vasculitis, and five did not attend the second visit. At T0, these 10 patients had characteristics similar to the patients that completed the study.
Factors associated with severe exacerbations
Table 2 shows the results of the unadjusted and adjusted logistic regression models performed to examine whether sociodemographic and clinical characteristics could predict the likelihood of exacerbations in the following year. In the unadjusted models, seven variables were associated with severe exacerbations in the following year: age, the number of exacerbations in the prior year, the presence of severe dyspnea, the CAT score, SpO2, FEV1, and the GOLD stage.
Summary of logistic regression analyses for identifying sociodemographic and clinical characteristics that might predict severe COPD exacerbations.

aAdjusted for the total number of exacerbations in the previous year.
p < 0.05.
CAT, chronic obstructive pulmonary disease assessment test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; GOLD, global initiative for chronic obstructive lung disease; mMRC, modified British Medical Research Council scale; SpO2, resting oxygen saturation.
However, in the adjusted models, only age and the number of exacerbations in the previous year could predict severe exacerbations in the following year. The multivariate model (not shown), which included significant sociodemographic and clinical characteristic variables from the adjusted models, suggested that age and the number of exacerbations in the prior year remained the strongest determinants (OR 1.10, 95% CI 1.02–1.19, p = 0.012; and OR 1.49, 95% CI 1.08–2.06, p = 0.016, respectively).
Table 3 shows the results of the unadjusted and adjusted logistic regression models performed to examine whether physical performance tests (6MWT, 5STS, and 4MGS) were associated with severe exacerbations in the following year. All physical performance tests were associated with severe exacerbations in the following year in the unadjusted models. However, the 4MGS test did not remain a significant factor, when the model was adjusted for age and the number of exacerbations in the previous year. The 6MWT and 5STS test showed similar ORs in the adjusted models.
Summary of logistic regression analysis for identifying physical performance tests that might predict severe COPD exacerbations.
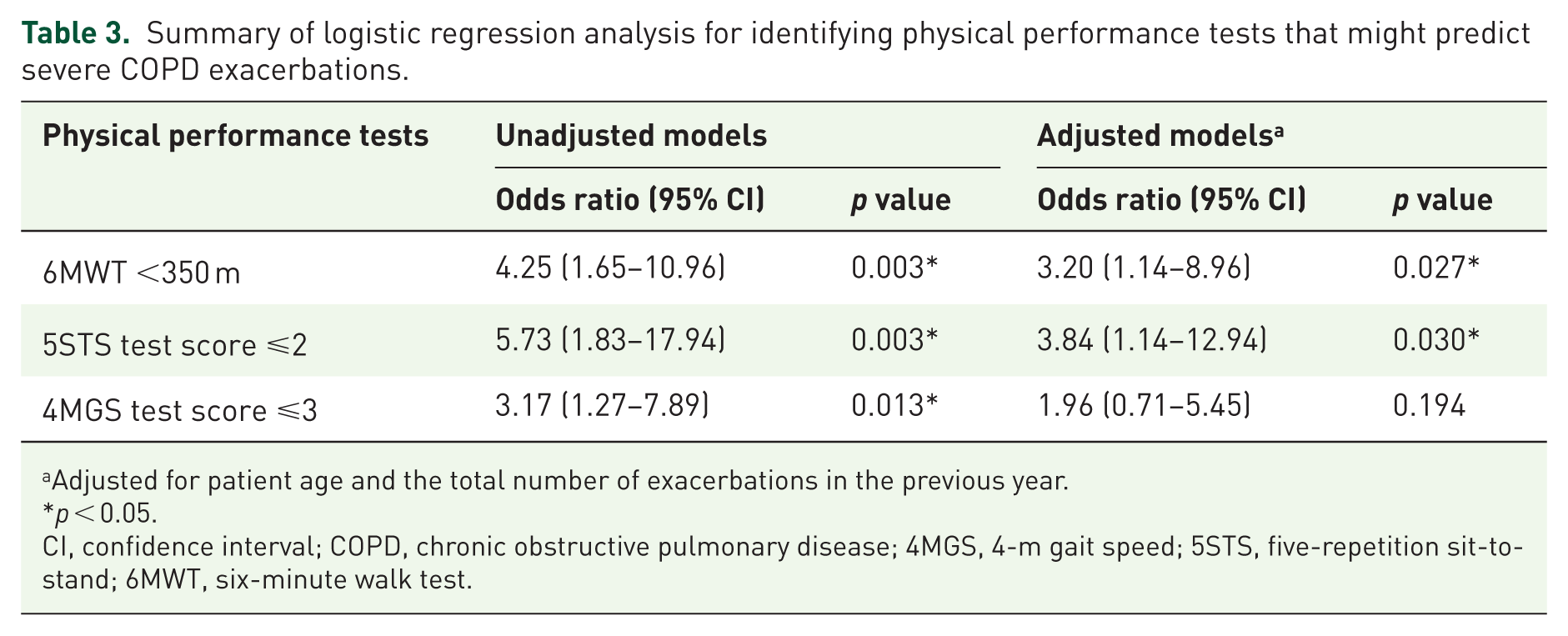
aAdjusted for patient age and the total number of exacerbations in the previous year.
p < 0.05.
CI, confidence interval; COPD, chronic obstructive pulmonary disease; 4MGS, 4-m gait speed; 5STS, five-repetition sit-to-stand; 6MWT, six-minute walk test.
Figure 1 shows the ROC plots of the 6MWT and 5STS test (combined with age and the number of exacerbations in the previous year) for discriminating between patients with COPD that experienced and did not experience severe exacerbations in the following year. The AUC for the 6MWT was 0.783 (95% CI 0.686–0.879) and the AUC for the 5STS test was 0.793 (95% CI 0.704–0.882).
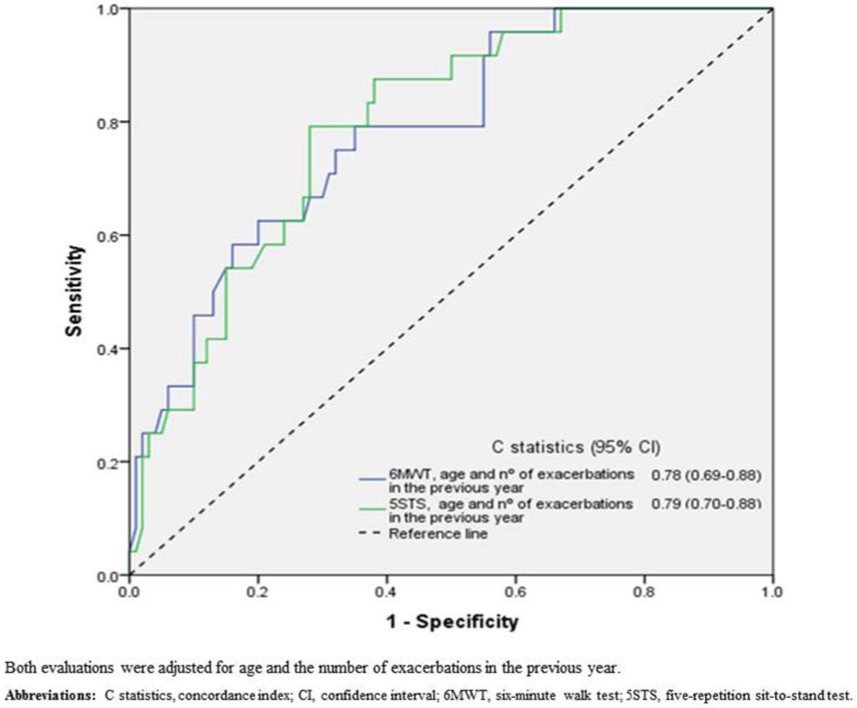
Receiver operating characteristics curves show the ability of physical performance tests to predict severe exacerbations in the following year.
Discussion
In this study, we assessed associations between physical performance tests and severe exacerbations in the following year among patients with stable COPD. The 5STS test represented a relevant, independent factor for predicting the likelihood of severe exacerbations in the following year among patients with COPD. In addition, the 5STS test and the 6MWT had similar predictive abilities and discriminatory accuracies for identifying patients at high risk of hospital admission.
We found that patients with 6MWT scores <350 m were more likely to experience exacerbations in following year, based on our results from the unadjusted model and the model adjusted for age and the number of exacerbations in the previous year. These findings were consistent with previous studies. For example, Zanoria and ZuWallack 13 also showed that patients with 6MWT scores <350 m were more likely to experience COPD exacerbations over a 1-year period, even after adjusting for relevant covariates. Andrianopoulos et al. 14 also predicted an increased risk of COPD exacerbations, when they used a similar cut-off point (<357 m). Finally, Morakami et al. 15 reached the same conclusion, but with a different cut-off point, one more appropriate for their population.
Our results showed that patients with 5STS test scores ⩽2 (less functional) were more likely to experience COPD exacerbations in the following year, both before and after adjusting the model for age and the number of exacerbations in the previous year. To our knowledge, this study was the first to explore and identify the relationship between the 5STS test and severe COPD exacerbations in the following year, for patients with stable disease. Only one previous study explored the predictive ability of a similar test, 20 the 1-min sit-to-stand (STS) test, which measured the maximum number of sit-to-stand actions completed in a given time. However, that study did not find a relationship between the test and COPD exacerbations in the following year. 32 A potential explanation for this discrepancy between the 5STS and the STS tests could be that they required different physiological demands. Although each test required identical movements, it has been argued that the 5STS test might reflect lower limb power, and the STS test might reflect lower limb endurance. 33 In fact, patients with COPD typically perceive more exertion and fatigue in the quadriceps muscles after the STS test than they do after the 5STS test. 34
In addition, this study showed that the 5STS test model, adjusted for age and the number of exacerbations in the previous year, could accurately (i.e. a good AUC) discriminate between patients likely and those unlikely to experience COPD exacerbations within the following year. Moreover, we found that the 5STS test and 6MWT had similar AUCs; consequently, the 5STS test was not substantially better than the 6MWT as a prognostic tool. This finding was valuable, because it suggested that the 5STS test could substitute the 6MWT for predicting COPD exacerbations within 1 year.
Our unadjusted model results showed that patients with 4MGS test scores ⩽3 (less functional) were more likely to experience exacerbations in the following year. However, this finding was not significant after the model was adjusted for age and the number of exacerbations in the previous year. In contrast to these results, Kon et al. 21 showed that the 4MGS test was a good predictor of exacerbations, even after adjusting for the number of exacerbations in the previous year. Nevertheless, there were several important differences between that early study and the present study, which might explain this inconsistency. First, Kon et al. 21 calculated the velocity (m/s) for completing the 4MGS test, and we examined score categories ranging from 0 to 4; 30 thus, our analysis might have had lower statistical power than their analysis. On the other hand, compared to our cohort, those authors examined a hospitalized, older cohort, with worse 4MGS test scores and worse states of health, which could have increased their discriminative ability.
Many of the other demographic and clinical factors analyzed in our study were predictive of exacerbations in following year in an unadjusted model, but not after adjusting the model for the number of exacerbations in the previous year. These results of from both the unadjusted and adjusted models were expected. First, we selected these factors, because previous studies had shown that they were predictive of COPD exacerbations.9–12,35 Moreover, in our adjusted models, we intentionally adjusted for the factor known to be the strongest predictor of exacerbations (the history of exacerbations in previous years).3,8 Therefore, many of the initially significant factors were excluded in the adjusted regression model.
Our study illustrated several practical applications from a clinical perspective. The 5STS test had predictive and discriminative abilities similar to those of the 6 MWT. Therefore, the 5STS test could be used in clinical settings where a prognostic factor of exacerbations is needed, but there may not be time to perform the 6MWT, or the patient might not be able to walk at a specific time. However, it is important to keep in mind that the ability of the 5STS test to identify patients at risk of exacerbation in the following year also depended on the patients’ age and history of exacerbations.
Strengths and limitations
This study had several strengths. First, to our knowledge, no previous study has compared the 6MWT with several alternative tests for their abilities to predict COPD exacerbations. Our study design provided the opportunity to compare all of these tests in the same study, with the same cohort. Second, we examined both the predictive and discriminative abilities of these tests to explore consistency. Most previous studies that examined associations between the 6MWT and the occurrence of COPD exacerbations explored only one of these abilities.13,15 Third, we intentionally adjusted the model for the factor known to be the strongest predictor of COPD exacerbations (the history of exacerbations in previous years). Adjusting for this factor reinforced the relevance and value of the identified performance tests (6MWT and 5STS).
This study also had several limitations. First, although we included a wide variety of possible predictors of COPD exacerbations in our population, some important factors could have been omitted. For example, if we had included participation in rehabilitation programmes, the quantity of medications, and the use of oxygen supplementation, we might have improved the predictive capacity of our models. However, we lacked data on those factors. Moreover, pulmonary rehabilitation services were not widely used for patients with COPD. Second, because this study was conducted in a single hospital, and only a small number of women were included, the generalization of our results to other clinical settings or to the female population should be carried out with caution. Third, we did not evaluate the roles of important medications in COPD exacerbations, such as anticholinergics or corticosteroids, which were evaluated in previous studies.11,35,36 For example, Paggiaro et al. 36 showed that chronic inhaled corticosteroids could reduce the severity of COPD exacerbations compared to a placebo group. Fourth, we did not consider patients lost to follow-up, which could have introduced a degree of bias. However, those patients constituted a small proportion of the total cohort, and their characteristics were significantly different from those of the included patients. Finally, we only compared the discriminative ability of the two tests, and we did not assess if they added discriminative value to age and exacerbations in the previous year. Nevertheless, our regression models allow us to see that these tests added prognostic value. These considerations should be addressed in future studies.
Conclusion
We demonstrated that, among patients with stable COPD, a 5STS score ⩽2, combined with patient age and a history of exacerbations, served as a relevant predictor of severe COPD exacerbations in the year following the test. In addition, the present study showed that the 5STS test and the 6MWT had very similar predictive abilities and both could identify patients with a high risk of hospital admission. This information suggested that the 5STS test might be a useful alternative to the 6MWT for predicting COPD exacerbations. Future research should focus on whether the 5STS test might also be associated with mortality in a COPD population. Furthermore, future studies should investigate whether appropriate care and/or preventive interventions that can improve the 5STS test score might reduce the high rate of hospital admission among patients with stable COPD.
Footnotes
Acknowledgements
The authors wish to thank the patients and personnel of the hospital unit for their cooperation during the course of this study.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by AstraZeneca pharmaceutical Spain, S.A.