
Abstract
Stage III non-small cell lung cancer (NSCLC) has a dismal prognosis, with only 15–20% of patients alive at 5 years after concomitant chemo–radiotherapy, which represents the standard treatment. Targeting immune-checkpoint inhibitors represents a standard option for advanced NSCLC. Improvements in understanding of the immune profile of NSCLC has led to the development of immunotherapeutic strategies, including inhibitory molecules responsible for abrogating an anticancer immune response such as programmed cell-death 1 and programmed cell-death ligand 1. A recently published phase III trial (PACIFIC) showed for the first time an improved overall survival in stage III NSCLC patients with consolidative durvalumab.
The aim of this review is to summarize and discuss the clinical evidence for the use of durvalumab in stage III NSCLC, with a brief overview on future perspectives in this setting.
Introduction
Lung cancer represents the leading cause of cancer death worldwide. 1 Despite advances in diagnostic techniques over recent years, one third of patients are still diagnosed with locally advanced disease, 2 for which platinum-based doublet concurrent chemo–radiotherapy (CRT) has become the first-choice treatment over the past decade.3–5 However, prognosis is still dismal, as median overall survival (OS) ranges between 17 and 28.7 months3,6 and only about 15–20% of patients are alive at 5 years.3,4 These survival data remain approximately the same with the addition of surgery. 4
In recently published phase III trials with modern radiotherapy (RT) and positron emission tomography–computed tomography (PET-CT) for staging, the local tumour progression rates were about 30–40% and distant progression was detected in half of the patients.6,7
New approaches that preferentially tackle both local and distant disease sites are needed to improve long-term survival and cure rates.
Attempts to improve the long-term survival include RT dose escalation, 6 different chemotherapy combinations 8 and adding biological agents to standard regimens. 6 At present, none of these have demonstrated solid improved outcomes.
Targeting immune-checkpoint inhibitors (ICIs) represents a standard option for advanced non-small cell lung cancer (NSCLC).9,10
Improved understanding of the immune profile of NSCLC has led to immunotherapeutic strategies, including inhibitory molecules responsible for abrogating an anticancer immune response such as programmed cell-death 1 (PD-1) and programmed cell-death ligand 1 (PD-L1).
To date, nivolumab, pembrolizumab and atezolizumab have been approved by the US Food and Drug Administration (FDA) 11 and European Medicines Agency (EMA) 12 as a treatment option for pretreated patients with advanced NSCLC. Pembrolizumab is also licensed as first-line treatment for treatment-naïve metastatic NSCLC patients with PD-L1 expression ⩾ 50% and for metastatic NSCLC with ⩾1% PDL1 expression after progression following first-line platinum-based doublet chemotherapy. 9 In addition and more recently, pembrolizumab has received the authorization by both agencies, in combination with platinum-based chemotherapy, in previously untreated advanced NSCLC regardless of the PD-L1 status, becoming the standard of care in this setting. 10
These results might address the current poor prognosis of stage III NSCLC by providing newer treatment paradigms that incorporate immunotherapy.
Durvalumab (MEDI4736), a novel ICI, particularly as an anti-PD-L1 antibody, inhibits binding of PD-L1 to PD-1 and B7-1, thus promoting the ability of T cells to recognize and eliminate tumour cells. Antonia and colleagues reported a longer progression-free survival (PFS) with durvalumab as consolidation therapy compared with placebo in stage III NSCLC patients who did not have disease progression after two or more cycles of platinum-based CRT. 13
On the basis of these data, durvalumab received FDA approval as consolidation chemotherapy in stage III disease after CRT in February 2018, the first such case in the use of ICIs. 11 In September 2018, the EMA approved durvalumab as consolidation therapy in stage III disease after CRT, only if PD-L1 is expressed in ⩾1% of tumour cells. 12
The aim of this review is to summarize and discuss the clinical evidence for the use of durvalumab in stage III NSCLC, with a brief overview on future perspectives in this setting.
Mechanism of action
The PD-1 receptor is an immune-checkpoint protein expressed on activated T cells (after antigen exposure) with two corresponding ligands, PD-L1 and PD-L2. PD-L1 (also named B7-H1 and CD274) is a transmembrane protein, expressed in haematopoietic cells, tumour cells and tumour stroma. 13 PD-L1 can bind to either the PD-1 receptor or to CD80 (also named B7-1, expressed on activated T cells and on antigen-presenting cells (APCs). Interactions between PD-L1 and PD-1/CD-80 can lead to inhibition of cytotoxic T-cell activation.14,15
The expression of PD-L2 is less common in cancer, and regulates the priming and the polarization of T cells. 16 To date, there is no evidence indicating that antibodies against PD-1, which block binding to both PD-L1 and PD-L2, are more effective when compared with antibodies against PD-L1 only. 14
Durvalumab (MEDI4736) is fully human high-affinity immunoglobulin G1-kappa (IgG1κ) monoclonal antibody that blocks PD-L1 by binding to PD-1 (IC50 0.1 nmol/l) and CD-80 (IC50 0.04 nmol/l). 15 Durvalumab binds with a high affinity to PD-L1 but not to PD-L2, the latter playing a role in controlling inflammation in normal tissue; this mechanism of action potentially decreases the immune-related toxicity associated with the PD-L2 interaction.
Efficacy
Durvalumab in the metastatic disease
Durvalumab was first evaluated in a large phase I/II study on patients with an advanced solid tumour, including refractory advanced NSCLC patients [ClinicalTrials.gov identifier: NCT01693562]. 16 Patients received durvalumab intravenously (IV) from 0.1 to 10 mg/kg every 2 weeks (Q2W) or 15 mg/kg every 3 weeks for up to 12 months or until unacceptable toxicity or disease progression. A total of 304 patients received durvalumab 10 mg/kg Q2W, 16 with an overall response rate (ORR) of 17.5%. Higher response rates were reported in treatment-naïve patients (ORR of 27.1% versus 13.0% in heavily pretreated patients) and when PD-L1 expression was high (⩾25% PD-L), with ORR of 25.3% versus 6.1% in PD-L1 < 25% (low).
A subsequent study from Antonia and colleagues 17 reported results from 59 treatment-naïve NSCLC patients, showing an ORR of 29% in patients with high PD-L1 expression versus 11% in low PD-L1 patients.
Similar results were shown in the ATLANTIC trial [ClinicalTrials.gov identifier: NCT02087423], 18 where the patients with higher PD-L1 expression had better OS. The 1-year OS rate was 50.8% for very high PD-L1 (⩾90% PD-L1), 47.7% for high PD-L1 and 34.5% in low PD-L1 populations.
However, AstraZeneca has reported an update of the large randomized phase III MYSTIC study on 16 November 2018, where durvalumab as monotherapy and in combination with tremelimumab (an ICI anti-CTL-4) did not meet the primary endpoints of improving OS and PFS compared with chemotherapy in patients with ⩾25% PD-L1 (determined by Ventana assay, SP263). Few phase III trials, such as the PEARL, POSEIDON and NEPTUNE studies [ClinicalTrials.gov identifiers: NCT03003962, NCT03164616 and NCT02542293, respectively], evaluating the role of durvalumab in monotherapy or in combination with tremelimumab as first-line treatment in advanced NSCLC patients, are currently ongoing.
Durvalumab in stage III NSCLC
Durvalumab and radiotherapy: preclinical evidence
Preclinical data consistently show a clear beneficial and possibly synergistic effect when radiotherapy is combined with anti-PD-1.17,19,20
During the development of cancer, the relationship between the tumour and the host immune system evolves from one in which the tumour cells are recognized and destroyed by the immune system (immune elimination) to immune equilibrium, where tumour cells and immune system coexist, and finally to immune escape. 21 The immune-escape stage is characterized by upregulated inhibitory ligands and cytokines and reduced major histocompatibility complex (MHC) class I expression, which ultimately causes poor antigen presentation and masks the tumour from immune surveillance and elimination. 21 Radiation may ‘unmask’ the tumour and make it more visible to both the innate and adaptive immune systems through the activation of downstream immune responses and priming of T cells, 22 and the upregulation of the expression of MHC-I on the tumour surface to enable better presentation of tumour-specific peptides (which enhances the visibility of the tumour to cytotoxic T cells). 23
By inducing the antigen recognition, radiation might also induce the T-cell-mediated inhibition of untreated distant tumours (known as the abscopal effect). 24 Moreover, radiation-induced deoxyribonucleic acid damage may generate neoantigen and trigger the immune surveillance. 25
Since different types of ICIs target different pathways, the timing of the ICI–RT combination should be designed to maximize the potential synergistic effect.
Unfortunately, the paucity of data does not allow drawing of firm conclusions.
The secondary analysis of the KEYNOTE-001 trial [ClinicalTrials.gov identifier: NCT01295827] showed the NSCLC patients who received radiotherapy before pembrolizumab had better OS and PFS rates compared with the patients who did not receive radiotherapy, suggesting radiation may enhance the efficacy of immunotherapy. 26
Qian and colleagues showed that, in a cohort of 75 melanoma patients with 566 brain metastases treated with stereotactic radiosurgery (SRS) and ICI (anti-CTL-4 and anti-PD-1/PDL-1), the concomitant use of ICI and SRS resulted in a higher median volume reduction 45 days (63.1% versus −43.2%, p < 0.0001), 3 months (−83.0% versus −52.8%, p < 0.0001), and 6 months (−94.9% versus −66.2%, p < 0.0001) when compared with nonconcurrent therapy. 27
A recent retrospective analysis of 758 patients treated with ICI (anti-CTLA4 with or without anti-PD1/anti-PDL1) and RT suggested that OS was better for patients who received concurrent ICI and RT, especially when ICIs were started within 30 days before RT [median OS: 20 months (<30 days) versus 11 months (>30 days)]. 28
Moreover, the post hoc analysis of the PACIFIC trial suggests that starting the durvalumab within 14 days after CRT (rather than ⩾14 days) is associated with a higher benefit to OS and PFS. 29
Clinical evidence: durvalumab efficacy
This preclinical evidence and the abovementioned trials on durvalumab in advanced NSCLC form the core of the hypothesis behind the multicentre, randomized double-blind phase III PACIFIC trial [ClinicalTrials.gov identifier: NCT02125461] (Figure 1), which compared durvalumab as consolidation therapy with placebo in patients with stage III, locally advanced, unresectable NSCLC that had not progressed after platinum-based CRT. 10

PACIFIC phase III trial scheme.
Eligible patients had received two or more cycles of platinum-based chemotherapy concurrently with definitive RT (54–66 Gy), had no disease progression after this treatment and had completed the last radiation dose within 1–14 days before randomization. However, due to a protocol amendment, the delay between the end of RT and the randomization was augmented to 1–42 days.
A total of 713 patients were randomized in a 2:1 ratio, 1–42 days after CRT to receive durvalumab IV at a dose of 10 mg/kg of body weight (n = 473) or placebo (n = 236) Q2W for up to 12 months. Randomization was stratified according to patient’s age (<65 years versus ⩾65 years), sex and smoking history (current or former smoker versus never smoked). OS and PFS were the coprimary endpoints, assessed by blinded independent central review. Secondary endpoints were PFS at 12 and 18 months, ORR, duration of response, the time to death/distant metastasis, OS at 24 months, time to second progression, safety/tolerability, quality of life, immunogenicity and pharmacokinetics. PFS was defined from randomization (which occurred up to 6 weeks after CRT).
Patients provided archived tumour tissue samples, obtained before chemoradiotherapy, for PD-L1 testing (determined by Ventana assay, SP263). However, PD-L1 expression status was not mandatory for the inclusion.
The main results of the PACIFIC trial are summarized in Table 1.
Overview of the results (clinical efficacy) of the PACIFIC study.

Antonia et al. 13
Antonia et al. 30
Faivre-Finn et al. 29
CI, confidence interval; CRT, chemo–radiotherapy; ORR, overall response rate; OS: overall survival; PD-L1, programmed cell-death ligand 1; PFS, progression-free survival; NR, not reached; Q2W, once every 2 weeks.
The first planned interim analysis showed that median PFS was 16.8 months [95% confidence interval (CI) 13.0–18.1] with durvalumab versus 5.6 months (95% CI 4.6–7.8) with placebo [hazard ratio (HR) 0.52; 95% CI 0.42–0.65; p < 0.001]. 13 The ORR was 28.4% with durvalumab versus 16% with placebo (p < 0.001). In this primary analysis, the time to second progression or death was longer in the durvalumab group (median 28.3 months versus 17.1 months).
The recently published analysis for the second primary endpoint of OS 30 showed a 12-month OS rate of 83.1% (95% CI 79.4–86.2) in the durvalumab group, as compared with 75.3% (95% CI 69.2–80.4) in the placebo group. The 24-month OS rate was 66.3% (95% CI 61.7–70.4) in the durvalumab group, as compared with 55.6% (95% CI 48.9–61.8) in the placebo group (two-sided p = 0.005). Durvalumab significantly prolonged median OS, as compared with placebo (stratified HR 0.68; 99.73% CI 0.47–0.997; p = 0.0025). Median OS was not reached [95% CI 34.7 to not reached (NR)] with durvalumab versus 5.6 months (95% CI 22.9 to NR) with placebo. The updated frequency of new lesions was 22.5% in the durvalumab group and 33.8% in the placebo group, with a lower incidence of new brain metastases in the durvalumab group than in the placebo group (6.3% versus 11.8%). No differences in OS were detected, on the basis of the PD-L1 expression.
On the basis of those results, the FDA (on 16 February 2018) and the EMA (24 September 2018) approved durvalumab for the treatment of unresectable stage III NSCLC without progression after treatment with concurrent CRT.
A post hoc (not preplanned) exploratory analysis based on PD-L1 expression and components of the concurrent CRT was presented at the European Society of Medical Oncology Congress 2018. 29 In the group PD-L1 ⩾ 1%, a median PFS of 17.8 months (95% CI 16.9 to NR) was observed with durvalumab versus 5.6 months (95% CI 3.6–11) with placebo (HR 0.46; 95% CI 0.33–0.64). The analysis in the group PD-L1⩽1% showed that median PFS was 10.7 months (95% CI 7.3 to NR) with durvalumab versus 5.6 months (95% CI 3.7–10.6) with placebo (HR 0.73; 95% CI 0.48–1.1).
With regard to OS, the group of PD-L1 ⩾ 1% showed that median OS was NR (95% CI NR to NR) versus 29.1 (95% CI 17.7 to NR) with placebo (HR 0.53; 95% CI 0.36–0.77). This analysis of the group PD-L1 < 1% showed that median OS was NR (95% CI 20.8 to NR) with durvalumab versus NR (95% CI 27.3 to NR) with placebo (HR 1.36; 95% CI 0.79–2.34).
Globally, this post hoc analysis showed a survival advantage in the group PD-L1 ⩾ 1% (consistently with the PFS). However, in the group PD-L1 < 1%, the placebo arm behaved differently (number of events/number of patients (%): 19/58 (32.8%) when compared with the placebo arm in the PD-L1 ⩾ 1%: 45/91 (49.5%). The difference in restricted mean survival time was not significant (−0.6 months; 95% CI −3.4 to 2.3).
The subgroup analyses confirmed the improved PFS and OS with durvalumab regardless of type of chemotherapy, radiation dose used or time from radiation to randomization.
The 3-year OS rates were presented at the American Society of Clinical Oncology (ASCO) meeting 2019. 31 Updated OS remained consistent with that previously reported, with the median OS NR (95% CI 38.4 months to NR) with durvalumab versus 29.1 months (95% CI 22.1–35.1) with placebo. The 12-, 24- and 36-month OS rates with durvalumab and placebo were 83.1% versus 74.6%, 66.3% versus 55.3%, and 57.0% versus 43.5%, respectively.
Caution must be used when drawing definitive conclusions on outcomes by PD-L1 status on the basis of post hoc exploratory subgroup analyses. Moreover, the PACIFIC trial was designed to evaluate durvalumab in the intention-to-treat (all comers) population, and PD-L1 testing was not mandatory and status was unknown for 37% of patients. Nevertheless, the EMA decided to approve durvalumab as consolidation treatment exclusively in the positive PD-L1 population.
Clinical evidence: durvalumab tolerability
In the first phase I/II study on durvalumab in metastatic disease, Antonia and colleagues showed that 57% of patients experienced treatment-related adverse events, mostly fatigue (17%), hyporexya (9%) and diarrhoea (9%), with a grade ⩾3 rate of 10% patients that led to discontinuation in 5% of patients. 16 Similar results were reported in the ATLANTIC study. 17
As expected, the phase III PACIFIC study confirmed the favourable tolerability profile of the durvalumab, even in association with the CRT (Table 2). The authors reported a maximum G3–4 adverse event (AE) rate of 30.5% of the patients in the durvalumab group and 26.1% in the placebo group. The most frequent AEs leading to the discontinuation of the regimen were pneumonitis (in 4.8% of the patients in the durvalumab group and in 2.6% of those in the placebo group), radiation pneumonitis (1.3% in both groups), and pneumonia (in 1.1% and 1.3%, respectively). 30
Overview of the results (tolerability) of the PACIFIC study.
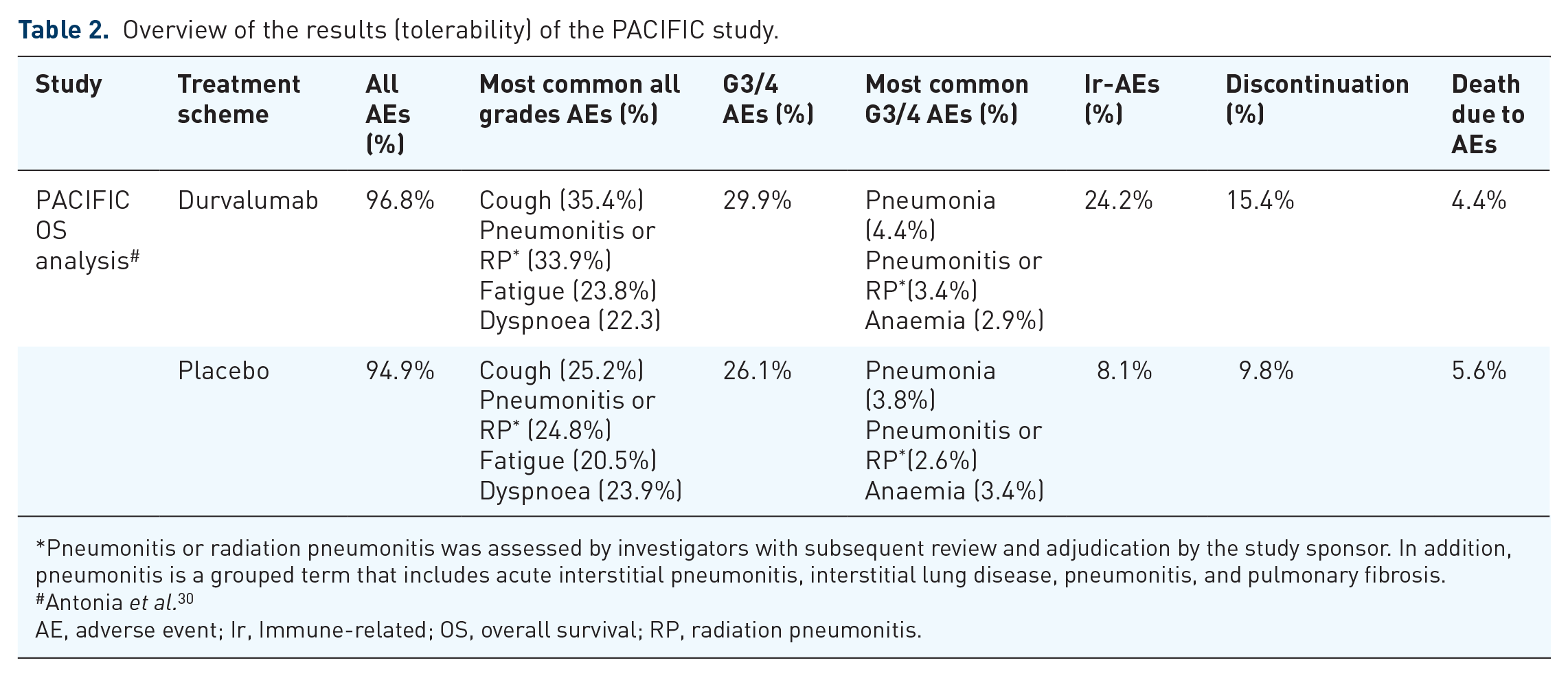
Pneumonitis or radiation pneumonitis was assessed by investigators with subsequent review and adjudication by the study sponsor. In addition, pneumonitis is a grouped term that includes acute interstitial pneumonitis, interstitial lung disease, pneumonitis, and pulmonary fibrosis.
Antonia et al. 30
AE, adverse event; Ir, Immune-related; OS, overall survival; RP, radiation pneumonitis.
Ongoing trials and future prospects
Durvalumab has been the first ICI approved in unresectable stage III NSCLC patients as consolidation therapy, but other ICIs are currently being investigated in this patient population.
Durm and colleagues reported at the ASCO 2018 meeting the preliminary data of a phase II, single-arm study of pembrolizumab (PD-1 inhibitor) as a consolidation treatment after concurrent CRT in patients with unresectable stage III NSCLC (Table 3). 32 The primary endpoint was time to metastatic disease or death (TMDD), and the secondary endpoints included PFS, OS and toxicity. A total of 93 patients were included. Median TMDD was NR (95% CI 18.7 to NR). The estimated 1-year and 2-year OS rates were 80.5% and 68.7%, respectively. The median PFS was 15.4 months (95% CI 10.4 to NR), which compares favourably with the PACIFIC trial results. Only 5.4% of patients developed a G3–4 pneumonitis, with one pneumonitis-related death.
Overview of the published studies of consolidation immune-checkpoint inhibitors in stage III non-small-cell lung cancer.

CI, confidence interval; CRT, chemo–radiotherapy; NR, not reached; NS, not specified; NSCLC, non-small-cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival, Q2W, once every 2 weeks; Q3W, once every 3 weeks.
The ongoing phase II NICOLAS trial [ClinicalTrials.gov identifier: NCT02434081] is currently evaluating the combination of concurrent CRT and nivolumab (PD-1 inhibitor), followed by consolidative nivolumab (12 months or until disease progression), with results expected for 2020.
The impressive results of the PACIFIC clinical trial have led to the design of several clinical trials combining RT with ICI, including a PACIFIC-2 study, where a concomitant CRT plus durvalumab arm will be studied [ClinicalTrials.gov identifier: NCT03519971] (Table 4).
Overview of the ongoing studies of consolidation immune-checkpoint inhibitors in stage III non-small cell lung cancer.

Hopefully, these ongoing studies will contribute to elucidating the role of the ICI–RT timing (concurrent versus sequential).
CRT, chemo–radiotherapy; ICI, immune-checkpoint inhibitor; NSCLC, non-small-cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; RT, radiotherapy; SoC, standard of care.
Conclusion
Durvalumab as consolidation is currently the standard of care after CRT in unresectable stage III NSCLC patients. The impressive results from the PACIFIC trial have demonstrated for the first time that ICI benefit is not limited to advanced disease and are the first practice-changing results in this setting in recent decades. Moreover, the safety profile and tolerability after CRT are favourable.
Long-term data and larger cohorts, together with mirror studies with other ICIs, are eagerly awaited, to confirm the integration of ICI in treatment strategies for unresectable stage III NSCLC patients.
Footnotes
Acknowledgements
The authors thank Sarah MacKenzie, PhD, for English editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
AB: nothing to declare.
LM: Consulting, advisory role: Roche Diagnostics. Lectures and educational activities: Bristol-Myers Squibb, Tecnofarma, Roche, AstraZeneca. Travel, accommodations, expenses: Chugai.
DP: Consulting, advisory role or lectures: AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, Roche. Honoraria: AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Celgene, Eli Lilly, Merck, Novartis, Pfizer, prIME Oncology, Peer CME, Roche. Clinical trials research: AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, Merck, Novartis, Pfizer, Roche, Medimmun, Sanofi-Aventis, Taiho Pharma, Novocure, Daiichi Sankyo. Travel, accommodations, expenses: AstraZeneca, Roche, Novartis, prIME Oncology, Pfizer.