
Abstract
Background:
We aimed to evaluate whether the severity of obstructive sleep apnea syndrome (OSAS) per se affects the prevalence of left ventricular (LV) diastolic dysfunction in patients without comorbidities.
Methods:
A total of 42 patients with first-diagnosed severe OSAS [apnea–hypopnea index (AHI) > 30] and 25 controls (AHI < 5), having been referred for snoring to the Sleep Laboratory Department of our tertiary Hospital, were enrolled in the study. Inclusion criteria were absence of any cardiovascular or oxidative stress-related comorbidities, and age between 20 and 70 years. Clinical, laboratory, echocardiographic, and polysomnographic data were recorded prospectively. Diastolic dysfunction diagnosis and grading was based on 2016 ASE/EACVI recommendations.
Results:
Severe OSAS was associated with significantly increased prevalence and degree of diastolic dysfunction (26/42; 61.9%) compared with controls (7/25; 28%) (p = 0.007). AHI ⩾ 55 (dichotomous value of severe OSAS subset) was also characterized by greater prevalence and degree of diastolic dysfunction compared with 30 < AHI < 55 patients (p = 0.015). In the severe OSAS subset, age >45 years-old, height <1.745 m, body-mass index (BMI) >27.76 kg m−2, OSAS severity (AHI > 57.35), oxidative stress (overnight reduction of reduced to oxidized glutathione ratio < 18.44%), and BMI/height ratio > 16.155 kg m−3 (an index describing ‘dense’, short-heavy patients) presented significant diagnostic utility in identifying diastolic dysfunction in ROC-curve analysis (0.697 ⩾ AUC ⩾ 0.855, 0.001 ⩽ p ⩽ 0.018). In binary logistic regression model, advanced age (OR 1.23, 95% CI 1.025–1.477; p = 0.026) and AHI (OR 1.123, 95% CI 1.007–1.253; p = 0.036) showed independent association with diastolic dysfunction in severe OSAS.
Conclusions:
The present prospective study may suggest that severe OSAS is significantly associated with LV diastolic dysfunction; OSAS clinical severity exerts a positive influence on (and possibly constitutes an independent risk factor of) LV diastolic dysfunction.
The reviews of this paper are available via the supplementary material section.
Introduction
Obstructive sleep apnea syndrome (OSAS) is a chronic respiratory sleep disorder characterized by repetitive apnea or hypopnea episodes induced by narrowing of the upper airways during sleep. OSAS has emerged as an important risk factor for cardiovascular diseases, including coronary artery disease and myocardial infarction, heart failure, arterial hypertension, cardiac arrhythmia, pulmonary hypertension, and stroke.1–3 The pathogenesis underlying this relationship may be multifactorial, including hemodynamic alterations, sympathetic hyperactivity, endothelial dysfunction, systemic inflammation, and oxidative stress. 4
Left ventricular (LV) diastolic dysfunction is also an established independent risk factor for cardiovascular morbidity and mortality. 5 The possible effect of OSAS on the development of LV diastolic dysfunction [as well as on right ventricular (RV) diastolic performance] has been increasingly emphasized in recent times.6–8 However, data on this relationship are still conflicting,9,10 since several co-existing disorders in OSAS may also affect LV myocardial diastolic properties (i.e. arterial hypertension, diabetes mellitus).
Oxidative stress is significantly associated with the severity of OSAS. 11 We have previously shown that oxidative stress due to OSAS per se (in a population free of comorbidities known to also affect oxidative/antioxidative balance) may be associated with OSAS severity as well. 12 However, the possible impact of ‘sleep-induced’ oxidative stress on LV diastolic function in the setting of severe OSAS still remains undetermined (henceforth, the term ‘sleep-induced’ is used to describe oxidative stress due to OSAS per se, in patients free of oxidative stress-associated comorbidities).
In this prospective study we aimed to evaluate the possible ‘direct’ relationship between the clinical severity of OSAS and the prevalence of LV diastolic dysfunction in a highly selected population of OSAS patients free of comorbidities associated with diastolic dysfunction. Furthermore, we aimed to examine the possible effect of ‘sleep-induced’ oxidative stress on the development of diastolic dysfunction; hence comorbidities/factors known to significantly affect oxidative stress through pathways not related with OSAS per se were also excluded. Finally, the possible role of several pathways on prevalence of LV diastolic dysfunction was also assessed, by examining several biomarkers of systemic inflammation (C-reactive protein, CRP),13–15 LV wall stress (B-type natriuretic peptide, BNP) 16 and hypoxia-induced angiogenesis (vascular endothelial growth factor, VEGF-B).17,18
Methods
In this 3-year observational study (January 2012–2014), patients were enrolled prospectively by consecutive sampling from the sleep laboratory of Pneumonology of the University Hospital of Larissa, Greece. Inclusion criteria for OSAS patients included: (1) first diagnosed severe OSAS, as indicated by an apnea–hypopnea index (AHI) >30 in full polysomnography, (2) male gender, (3) no treatment for OSAS, (4) normal sinus rhythm on electrocardiography, (5) no history of coronary artery or other cardiovascular disease (congenital heart disease, cardiomyopathy, valvular or pericardial disease), (6) no history of arterial hypertension or antihypertensive medications, (7) systolic and diastolic blood pressure <140 mmHg and <90 mmHg respectively (measurements on 3 consecutive days), (8) medical history free of disease known to be related with increased oxidative stress (i.e. smoking, renal failure, chronic obstructive pulmonary disease, asthma, rhinitis, diabetes mellitus, cerebrovascular disease, dyslipidemia), and (9) left ventricular ejection fraction (LVEF) >50% on echocardiography, without any regional wall motion abnormality. Controls were recruited among patients referred to our sleep laboratory for snoring, if they had AHI <5 and fulfilled the above-mentioned inclusion criteria 2–9. Exclusion criteria included: age <20 and >70 and presence of mild-to-moderate OSAS (5 ⩽ AHI ⩽ 30).
The sample size of our study was based on previously reported data in patients without cardiovascular disease, 7 which suggested an increase of 175% in the prevalence of diastolic dysfunction in OSAS patients (55%) compared with controls (where the prevalence was 20%). In this respect, in order to depict a similar increase in the frequency of diastolic dysfunction in OSAS compared with control patients in our study, with a probability of a type I error of 5% and a power of 80%, at least 60 patients would be required for analysis.
Written informed consent for inclusion in the present study was obtained from all subjects, and the study was conducted according to the World Medical Association Declaration of Helsinki and approved by the Internal Review Board and Ethics Committee of the University of Thessaly (UT), ID: 455629/October/2011.
Clinical assessment
At baseline, patients were assessed clinically, were evaluated by the Epworth Sleepiness Scale questionnaire and underwent echocardiography. Subsequently, all patients were evaluated by a full polysomnographic study.
Pulmonary function tests were performed 1 day before polysomnography, by using a spirometer (Dräger, Lübeck, Germany), as described previously. 12
Blood samples were collected the night before and the morning after polysomnography for evaluation of several biomarkers of oxidative stress, hypoxia-induced angiogenesis (VEGF-B), inflammatory process (CRP), and LV wall stress (BNP). Morning blood sample analysis was also used for evaluation of the patients’ metabolic profile (total, HDL, and LDL cholesterol, triglycerides, glucose, urea, creatinine). Blood pressure (BP) measurements were obtained by using a mercury sphygmomanometer, after 5 min resting in a sitting position.
Echocardiography
Conventional transthoracic two-dimensional (2D) echocardiographic (System Vivid 3/1.5–3.6 MHz transducer, GE Medical Systems, Milwaukee, WI, USA) examination was performed to assess LV internal dimensions, LV wall thickness, and global LV/RV function, according to the recommendations of the American Society of Echocardiography. 19
LV end-diastolic and end-systolic volumes were measured by planimetry. LVEF was estimated by using the two-dimensional Simpson’s method of disks. RV end-diastolic area (EDA) and end-systolic area (ESA) were measured for calculating right ventricular fractional area change [RVFAC (%) = 100 × (RVEDA–RVESA)/RVEDA].
Atrial volumes were calculated using the biplane area-length method: Atrial volume = (Area4–chamber) × (Area2–chamber) × 0.85/atrial length. 20 The shorter atrial length from either the four- or two-chamber view was used as recommended for this formula. Atrial volumes were calculated at the end of ventricular systole (VOLmax), just before atrial contraction (VOLbac), and at the end of ventricular diastole (VOLmin). Atrial volume indexes were calculated by dividing each of VOLmax, VOLmin, and VOLbac by the patient’s body surface area calculated by the DuBois formula. Atrial passive emptying fraction [(VOLmax – VOLbac) × 100%/VOLmax], atrial active emptying fraction [(VOLbac – VOLmin) × 100%/VOLbac], and reservoir emptying fraction [(VOLmax – VOLmin) × 100%/VOLmax] were also calculated.
LV mass was calculated as suggested by Devereux and colleagues, 21 and indexed to body surface area. Relative wall thickness (RWT) was measured at end-diastole, as septal wall thickness + posterior wall thickness divided by LV diastolic diameter. 22
Assessment of LV diastolic function
Left ventricular diastolic function was assessed by performing Doppler echocardiography from the apical four-chamber view. Doppler signals were recorded along with the electrocardiogram at a sweep speed of 100 mm/s, and were stored digitally in the hardware for later analysis. Off-line analysis was carried out by an experienced cardiologist (EZ) blinded to patients’ identity and clinical status. The average of three consecutive cycles was used.
Mitral inflow pulsed-wave Doppler signals [peak velocities of early (E) and late (A) LV diastolic filling, the E/A ratio, isovolumic LV relaxation time (IVRT) and E-wave deceleration time (DTE)], tissue Doppler imaging (TDI)-derived peak systolic (Sm), early diastolic (Em), and late diastolic (Am) velocities at the lateral/septal mitral annulus, as well as pulmonary vein flow velocities whenever a satisfactory acoustic window was feasible (peak systolic S, peak diastolic D, S/D ratio, and pulmonary-atrial reversal signal) were recorded in each patient. Trans-tricuspid RV inflow velocities E and A, tricuspid regurgitation (TR) velocity, and TDI-derived velocities Sm, Em, and Am at the lateral tricuspid annulus were also analyzed. TDI-derived LV/RV Tei (myocardial performance) indices were calculated as markers of global LV/RV function, respectively. 23 Analysis was also performed for ‘advanced’ indices of LV filling pressures (lateral, septal, and average E/Em ratios) and biventricular diastolic dysfunction (Em/Am ratio at lateral/septal mitral annulus and lateral tricuspid annulus). 24
Left ventricular diastolic dysfunction was diagnosed according to recently proposed 2016 ASE/EACVI recommendations, 24 on the basis of four echocardiographic variables: Em velocity (septal Em <7 cm/s, lateral Em <10 cm/s), average E/Em ratio > 14, left atrial maximum volume index >34 ml/m2, and peak TR velocity >2.8 m/s (algorithm for evaluation of DD in subjects with normal LVEF). 24 Subsequently, the subset of diastolic dysfunction was further evaluated and graded as grade I (mild) diastolic dysfunction, grade II (moderate) diastolic dysfunction, and severe diastolic dysfunction. 24
Polysomnography
Fully attended nocturnal polysomnography (from 9 p.m. to 6 a.m. the next morning) was performed as previously described for our department (Alice 4 Diagnostic Device OBS/G7829, Respironics, Marietta, GA, USA). 12
Apnea was defined as cessation of airflow for at least 10 s. Hypopnea was defined as any reduction of airflow lasting >10 s and resulting in arousal or oxygen desaturation. 25 Desaturation was considered as a decrease in oxygen saturation (SaO2) of >4%. The apnea index (AI) was defined as the number of apnea events per hour of total sleeping time. The AHI was calculated as the number of apnea and hypopnea events per hour of total sleeping time. Arousals and arousal index were defined as also described in our previous report. 12
Oxidative stress assessment and biomarker measurements
Blood samples were analyzed for evaluation of markers of lipid peroxidation [thiobarbituric acid-reactive substances (TBARS)], protein peroxidation [reduced (GSH) and oxidized (GSSG) glutathione, GSH/GSSG ratio as a measure of cellular toxicity], oxygen peroxide production [Cu–Zn superoxide dismutase (SOD)], and total antioxidant capacity (TAC).26–28 Blood samples were collected, centrifuged, stored, and analyzed according to the technique we described previously. 12
Plasma BNP concentration was measured using a Biosite Triage immunoassay (Biosite Diagnostics, San Diego, CA, USA). Primary antibodies for human VEGF-B were used to detect the protein expression. VEGF-B levels (pg/ml) were measured in serum by using an immunoenzymatic assay (Biosource Europe SA, Nivelles, Belgium). The mean difference (±2SD) was 1.80 (−45.18 to 48.78).
Statistical analysis
Categorical variables were expressed as numbers (n) and percentages (%), and continuous variables as mean ± standard deviation (SD) of the mean. Kolmogorov–Smirnov test was used for normality assessment. Chi-squared or Fisher’s exact test were used to compare categorical variables and t test or Mann–Whitney U test to compare continuous variables as appropriate. Pearson’s correlation was used to test the statistical relationship between continuous variables. Overnight changes of blood pressure measurements and several biomarkers examined between severe OSAS patients with and without diastolic dysfunction were examined by repeated measures of ANOVA. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic performance of several clinical parameters/biomarkers in identifying LV diastolic dysfunction in severe OSAS patients. Binary logistic regression analysis was used to examine the effect of several risk factors in the development of LV diastolic dysfunction. The statistical package SPSS 17.0 (Chicago, IL, USA) was used. The statistical tests were two-sided. A p value < 0.05 was considered statistically significant.
Results
Severe OSAS (n = 42) versus controls (n = 25) subgroup analysis
A total of 42 patients with severe OSAS (AHI > 30) fulfilled the eligibility criteria and were enrolled in the study, and 25 controls (AHI < 5) were also examined. Baseline characteristics in the two groups are presented in Table 1. There were no significant differences within groups concerning age; yet, patients with severe OSAS demonstrated higher bodyweight and increased BMI and BSA values compared with controls.
Participants’ baseline somatometric characteristics.

Continuous data are presented as means ± standard deviation, categorical data as n (%).
BSA, body surface area; BMI, body mass index; OSAS, obstructive sleep apnea syndrome.
Baseline echocardiographic characteristics in severe OSAS and controls are demonstrated in Supplementary Table 1. There were no differences between the two groups concerning LV mass, dimensions and wall thickness; however, there was a tendency for concentric LV remodelling (as assessed by significantly increased RWT, p = 0.017) in the OSAS group. In addition, LV ejection fraction, right ventricular parameters, structural, and functional biatrial measurements showed no differences within groups.
According to strict echocardiographic criteria utilized, 24 the prevalence of diastolic dysfunction was significantly increased in severe OSAS (26/42; 61.9%) compared with the control group (7/25; 28%) (p = 0.007). Figure 1 illustrates severe OSAS versus control subgroup analysis with respect to the type of diastolic function; Grade I diastolic dysfunction was noted in 5 control and 24 severe-OSAS patients, while Grade II diastolic dysfunction in 2 patients in each subgroup (Fisher’s exact test, p = 0.007). Neither severe OSAS patients nor controls demonstrated Grade III diastolic dysfunction.

Incidence and grading of diastolic dysfunction in our severe OSAS patients (n = 42) compared with controls (n = 25).
Analysis confined into severe OSAS group (n = 42)
The subset of severe OSAS was further dichotomized into two equal subgroups of 21 subjects each, by using an AHI value of 55 as dichotomous cut-off (Figure 2). AHI ⩾ 55 was characterized by a more severe degree of diastolic dysfunction compared with patients with 30 ⩽ AHI < 55 (Fisher’s exact test, p = 0.015) (Figure 2).

Incidence and grading of diastolic dysfunction in patients with more critical severe OSAS (AHI ⩾ 55; n = 21) compared with those with less critical severe OSAS (30 < AHI < 55; n = 21).
Baseline echocardiographic parameters in patients with diastolic dysfunction (n = 26) and normal diastolic function (n = 16) are demonstrated in Table 2. Pulsed-wave Doppler transmitral inflow analysis and mitral annular TDI evaluation demonstrated significantly lower E-wave velocities, decreased E/A ratios, increased lateral Am velocities and depressed lateral Em/Am ratios in LV diastolic dysfunction subgroup. Left ventricular diastolic dysfunction was also associated with RV diastolic dysfunction indices, 8 including decreased tricuspid E/A ratio, increased Am, and decreased Em/Am on tricuspid annular TDI (p ⩽ 0.019; Table 2). LV and RV diastolic indices E/A ratio, Am and Em/Am ratio were significantly interrelated (r = 0.509; 0.552; 0.402, p = 0.001; <0.001; 0.008, respectively).
Echocardiographic measurements in our severe OSAS subset (n = 42) with (n = 26) and without (n = 16) left ventricular diastolic dysfunction.

Continuous data are presented as means±standard deviations. BSA, body surface area; DF, diastolic function; E,A, transmitral inflow early and late peak diastolic velocity, respectively; FAC, fractional area change; IVC, inferior vena cava; IVSd, interventricular septum thickness at end-diastole; LA, left atrial; LAV, LA volume; LAEF, LA emptying fraction; LV, left ventricular; LVEF, LV ejection fraction; LVIDd, LV internal diameter at end-diastole; OSAS, obstructive sleep apnea syndrome; PV, pulmonary vein; PWd, posterior wall thickness at end-diastole; RAEF, right atrial emptying fraction; RAV, right atrial volume; RV, right ventricular; RWT, relative wall thickness; S,D, systolic, diastolic flow respectively; Sm,Em,Am, peak systolic, early and late diastolic TDI-derived mitral and tricuspid annular tissue velocities, respectively; TV, tricuspid valve.
Table 3 and Figure 3 demonstrates polysomnographic data in severe OSAS patients with and without diastolic dysfunction; baseline values and % overnight (night–morning) changes of blood pressure measurements and several examined biomarkers are also presented. Age >45 years-old, height <1.745 m, BMI >27.76 kg m−2, OSAS severity (as indicted by AHI > 57.35) and oxidative stress (as assessed by overnight reduction of reduced to oxidized glutathione ratio < 18.44%) presented remarkable diagnostic performance in predicting underlying diastolic dysfunction (Table 4). BMI/height ratio > 16.155 kg m−3, an index we introduced to describe ‘dense’, short-heavy patients, also predicted diastolic dysfunction in ROC-curve analysis (Table 4). Instead, other somatometric variables (such as increased weight, BSA), laboratory data (blood glucose levels, lipidemic profile), inflammatory or hypoxic indices failed to be related with diastolic dysfunction (all Ps > 0.05).
Polysomnographic data and biomarker/biochemical measurements in our severe OSAS subset (n = 42) with (n = 26) and without (n = 16) left ventricular diastolic dysfunction.
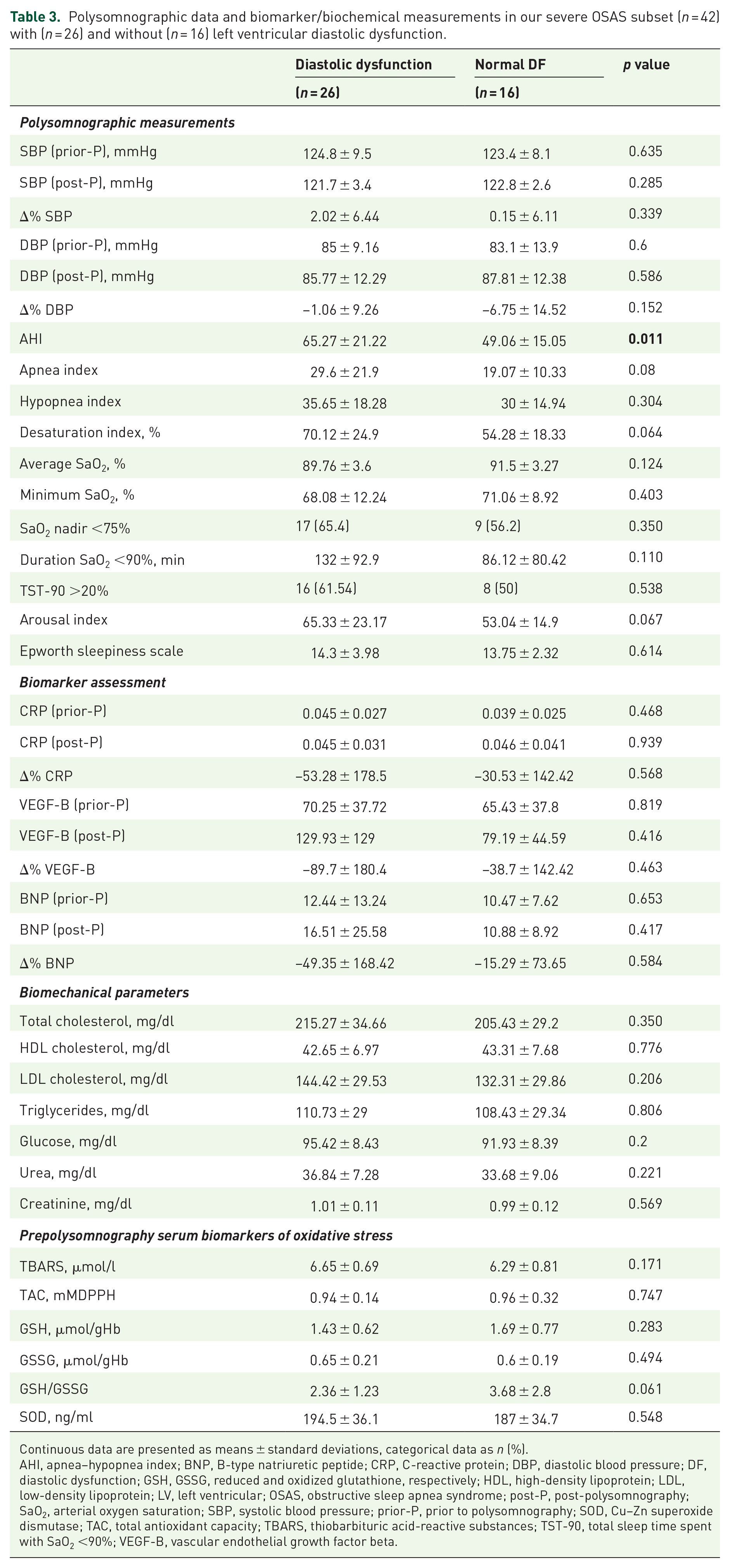
Continuous data are presented as means ± standard deviations, categorical data as n (%).
AHI, apnea–hypopnea index; BNP, B-type natriuretic peptide; CRP, C-reactive protein; DBP, diastolic blood pressure; DF, diastolic dysfunction; GSH, GSSG, reduced and oxidized glutathione, respectively; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LV, left ventricular; OSAS, obstructive sleep apnea syndrome; post-P, post-polysomnography; SaO2, arterial oxygen saturation; SBP, systolic blood pressure; prior-P, prior to polysomnography; SOD, Cu–Zn superoxide dismutase; TAC, total antioxidant capacity; TBARS, thiobarbituric acid-reactive substances; TST-90, total sleep time spent with SaO2 <90%; VEGF-B, vascular endothelial growth factor beta.

Overnight changes (%) in oxidative stress biomarkers in the subset of severe OSAS patients (n = 42), divided into patients without (open bars, n = 16) and with (closed bars, n = 26) diastolic dysfunction. Bars and vertical lines represent mean and standard deviation values, respectively.
Diagnostic performance of several clinical, polysomnographic and oxidative-stress parameters in identifying underlying left ventricular diastolic dysfunction in our severe OSAS patients (n = 42).

% (Δ)GSH/GSSG, % reduced to oxidized glutathione ratio overnight change; AHI, apnea hypopnea index; AUC, are under the curve; BMI, body mass index; CI, confidence interval; OSAS, obstructive sleep apnea syndrome; Se (%), sensitivity; Sp (%), specificity.
The above univariate determinants of diastolic dysfunction in severe OSAS were further analyzed in a multivariate binary regression model (Table 5). Advanced age (OR 1.23, 95% CI 1.025–1.477; p = 0.026) and OSAS clinical severity as assessed by AHI (OR 1.123, 95% CI 1.007–1.253; p = 0.036), but neither specific body-type characteristics nor oxidative stress indices, showed independent association with diastolic dysfunction in this specific subgroup.
Multivariate binary regression model examining the effect of several univariate determinants of left ventricular diastolic dysfunction in our severe OSAS (n = 42) subset.

AHI, apnea–hypopnea index; BMI, body mass index; CI, confidence interval; DD, diastolic dysfunction; DF, diastolic function; GSH/GSSG, reduced to oxidized glutathione ratio; OR, odds ratio; OSAS, obstructive sleep apnea syndrome.
Discussion
In the present study, we evaluated LV diastolic dysfunction in a highly selected OSAS population free of cardiovascular and oxidative stress-associated comorbidities. The main findings are as follows: the prevalence of diastolic dysfunction in severe OSAS (AHI > 30) is significantly higher than in patients with snoring and AHI < 5; in the subset of severe OSAS, OSAS clinical severity exerts a positive effect on the prevalence of diastolic dysfunction; and, among several univariate determinants, OSAS severity showed independent association with LV diastolic dysfunction in severe OSAS.
Both OSAS and LV diastolic dysfunction are established risk factors for cardiovascular morbidity and mortality.2,5 Although the possible impact of OSAS on LV diastolic dysfunction is increasingly emphasized,6,7 data regarding the potential causal relationship between the two entities is still controversial.9,10 A plausible explanation is that, in most studies, mixed OSAS population (with several co-existing disorders that also predispose to the development of LV diastolic dysfunction) was included. In our series, patients without cardiac or other disease known to be related with LV diastolic dysfunction in both severe OSAS and control groups were enrolled. In addition, oxidative-stress associated diseases (e.g. hyperlipidemia, diabetes mellitus), which may adversely affect diastolic myocardial properties through several pathways, were also excluded.29,30 In this respect, we aimed at recruiting a highly selected homogenous OSAS population in order to arrive in valid and meaningful results on the relationship between OSAS severity per se and LV diastolic dysfunction.
In the present study, diastolic dysfunction was diagnosed and graded according to the stepwise approach proposed by recent 2016 ASE/EACVI recommendations. 24 This is important, since diastolic dysfunction may have been overdiagnosed in previous studies. 31 Our findings provided a higher prevalence and degree of diastolic dysfunction in patients with advanced OSAS clinical severity (Figures 1, 2). Interestingly, our study also pointed out that the majority of our patients with severe OSAS demonstrated mild, rather than more severe, degrees of diastolic dysfunction (Figure 2). This is in line with previous reported data in highly selected OSAS populations without cardiovascular comorbidities, 7 while more severe degrees of dysfunction have been described in patients with co-existing pathologies. 6 Our data also suggested that, apart from advanced age (as expected), 32 OSAS clinical severity (assessed by elevated AHI) may constitute an independent risk factor of LV diastolic dysfunction (Table 5). Certainly, several additional polysomnographic (i.e. apnea, desaturation, and arousal) indices examined in our series also tended to demonstrate an association with diastolic dysfunction (see Results section, Table 3); their role requires further investigation in larger-scale studies in the future. Instead, T90 (total sleep time spent with SaO2 < 90%) >20% and SaO2 nadir < 75% failed to demonstrate any direct association with LV diastolic dysfunction in our population (Table 3), possibly indicating a minor diagnostic performance of these indices in patients without cardiovascular or oxidative stress-related comorbitidies. 33 Consequently, our findings suggest that OSAS per se (in the absence of comorbidities) may represent a significant cardiovascular risk factor, and possibly underline the importance of OSAS therapy in patients otherwise healthy. Of course, the clinical implication of OSAS therapy in such a specific population, in terms of reversibility of LV diastolic function and favorable outcomes, remains to be evaluated in the future.
Our series provides evidence of mild reduction of LV systolic function in severe OSAS diastolic dysfunction subset, as assessed by LVEF (slightly reduced, however within normal limits) (Table 2). This is in line with our previous investigation examining LV systolic function in children with obstructive sleep-disordered breathing, 34 and could be explained through several mechanisms, for example, nocturnal increased cardiac loading conditions, hypertension, increased catecholamine release, and desaturation-induced myocardial ischemia. 35 In addition, our data may indicate left atrial functional remodeling in the diastolic dysfunction subset of severe OSAS, as assessed by reduced passive left atrial emptying fraction (Table 2); a plausible explanation might be the high percentage (24/26, 92%) of grade I diastolic dysfunction (impaired relaxation) in this subset (Figure 2). 24 Remarkably, there was no evidence of LV/RV (or atrial) structural remodeling in severe OSAS-associated diastolic dysfunction, in terms of cardiac chamber dimensions, volumes, or LV mass/wall thickness; significant interrelation between LV/RV diastolic indices (see Results section, Table 2) could imply common pathogenic pathways of diastolic dysfunction for the two ventricles or interventricular diastolic interdependence mechanisms. 8 In addition, in severe OSAS diastolic dysfunction subgroup, there were no findings suggestive of either elevated pulmonary artery systolic pressures (assessed by TR velocities), or LV filling pressures (assessed by E/Em ratios 24 and BNP values 16 analysis) (Tables 2, 3). Thus, our findings may suggest a possible reversible nature of the pathogenic mechanisms underlying LV diastolic dysfunction in severe OSAS. Given the clinical magnitude of cardiovascular disease, recognition and potential inversion of these mechanisms might be of vital importance in preventing otherwise healthy OSAS patients from developing cardiovascular disease. In this context, several pathways leading to diastolic dysfunction were investigated, by examining overnight changes of several markers of ‘sleep-induced’ oxidative stress, and biomarkers of systemic inflammation (CRP) and hypoxia-induced angiogenesis (VEGF-B).
The hypoxia–reoxygenation shifts in patients with severe OSAS may induce oxidative stress, 36 which, in turn, may result in changes in cellular signaling and gene expression, and adversely alter cardiac mechanics and myocardial diastolic properties. 37 However, the possible impact of ‘sleep-induced’ oxidative stress on diastolic dysfunction in severe OSAS remains largely unknown. For this reason, a number of biomarkers reflecting several oxidative stress pathways, as well as antioxidant defense (assessed by total antioxidant capacity) were obtained before and after a full polysomnographic study. While baseline values were similar within subgroups (Table 3), their overnight changes (Figure 3) may indicate that an ‘oxidative-type’ of sleep is likely to characterize the diastolic dysfunction subset.
In our previous investigation, 12 we demonstrated that specific overnight alterations of reduced to oxidized glutathione (GSH/GSSG) ratio are associated with severe OSAS in a population also free of comorbidities. The present study indicates that overnight decrease in GSH/GSSG ratio may also discriminate patients with diastolic dysfunction in this specific population (Figure 3). In addition, overnight alterations of GSH per se and TBARS tended to differ markedly between severe OSAS subgroups with normal and abnormal diastolic function (Figure 3). In this respect, one could argue that increased oxidative stress derived from protein oxidation and (to a lesser extent) lipid peroxidation pathways may be implicated (but not independently, Table 5) in the pathogenesis of diastolic dysfunction in severe OSAS free of comorbidities.26–28
Severe OSAS has been associated with high blood levels of VEGF-B, a marker of critical hypoxia and increased angiogenesis. 17 In addition, there is growing evidence that OSAS is characterized by elevated CRP levels, and this effect is positively influenced by OSAS severity;13,14 yet, data regarding the possible impact of key regulators of angiogenesis or CRP levels on diastolic dysfunction in severe OSAS is extremely sparse.15,18 In our series, neither baseline VEGF-B and CRP values nor their overnight alterations were linked with diastolic dysfunction. Thus, our limited data may indicate that the development of diastolic dysfunction in severe OSAS might be neither angiogenesis-dependent 38 nor inflammatory-associated (at least concerning the specific steps of hypoxic regulators of angiogenesis and inflammatory cascades studied in the present investigation).
A few limitations to the study deserve mention. First, a sample size of 67 patients could be considered as quite small. However, our sample selection was based on previously reported data on the prevalence of diastolic dysfunction in an OSAS population quite similar to ours (prospective power calculation was performed). 7 In addition, strict inclusion criteria were utilized for patient enrollment; it is well established that the more homogenous a population, the smaller the sample size required to obtain a given level of precision. 39 Second, our population is quite uncommon, comprising exclusively middle-aged men. Of course, male sex has dominated comorbidity-free patients with severe OSAS and LV diastolic dysfunction in previous data. 7 However, one could argue that the synthesis of our population may have interfered with our findings, including the high prevalence of mild diastolic dysfunction in our series. Nevertheless, our findings should not be generalized to women, as none were included in the sample. Finally, our OSAS subset lacks information regarding the natural history of OSAS prior to the development of clinically severe syndrome, and the time course of LV diastolic dysfunction prior to its diagnosis. Certainly, genetic differences may exert diverse influence on the clinical phenotypes of special diseases in different populations; thus, it is imperative that our findings be validated in similar comorbidity-free populations, yet in larger-scale studies in the future.
In conclusion, our results may suggest that severe OSAS (AHI > 30) is associated not only with higher prevalence and degree of LV diastolic dysfunction, but also may constitute an independent risk factor for the development of the entity. LV diastolic dysfunction in severe OSAS is mild rather than moderate/severe and is characterized by functional (but not structural) cardiac remodeling and increased oxidative stress, as assessed by the GSH/GSSG pathway. This information is important, since OSAS is associated with considerable cardiovascular morbidity and mortality, and LV diastolic dysfunction may represent an easy to recognize, and potentially modifiable, mediating phase in the relationship between OSAS and cardiovascular disease.
Supplemental Material
Author_response_to_reviewer_comments – Supplemental material for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Supplemental material, Author_response_to_reviewer_comments for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities by John Papanikolaou, Melpomeni Ntalapascha, Demosthenes Makris, Triantafyllia Koukoubani, Vasiliki Tsolaki, George Zakynthinos, Konstantinos Gourgoulianis and Epaminondas Zakynthinos in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Supplemental material, Reviewer_1_v.1 for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities by John Papanikolaou, Melpomeni Ntalapascha, Demosthenes Makris, Triantafyllia Koukoubani, Vasiliki Tsolaki, George Zakynthinos, Konstantinos Gourgoulianis and Epaminondas Zakynthinos in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Supplemental material, Reviewer_1_v.2 for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities by John Papanikolaou, Melpomeni Ntalapascha, Demosthenes Makris, Triantafyllia Koukoubani, Vasiliki Tsolaki, George Zakynthinos, Konstantinos Gourgoulianis and Epaminondas Zakynthinos in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Supplemental material, Reviewer_2_v.1 for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities by John Papanikolaou, Melpomeni Ntalapascha, Demosthenes Makris, Triantafyllia Koukoubani, Vasiliki Tsolaki, George Zakynthinos, Konstantinos Gourgoulianis and Epaminondas Zakynthinos in Therapeutic Advances in Respiratory Disease
Supplemental Material
Supplementary_files – Supplemental material for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Supplemental material, Supplementary_files for Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities by John Papanikolaou, Melpomeni Ntalapascha, Demosthenes Makris, Triantafyllia Koukoubani, Vasiliki Tsolaki, George Zakynthinos, Konstantinos Gourgoulianis and Epaminondas Zakynthinos in Therapeutic Advances in Respiratory Disease
Footnotes
Author contributions
JP, KG, DM, and EZ made a substantial contribution to the concept and design of the work; MD, JP, EZ, TK, VT, and GZ participated in the acquisition, analysis and interpretation of data; JP and MD drafted the manuscript; KG, DM, TK, VT, GZ, and EZ critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript. Each author participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
The reviews of this paper are available via the supplementary material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.