
Abstract
Objective
We explored the relationship between enuresis and obstructive sleep apnea–hypopnea syndrome (OSAHS) in children and influencing factors of enuresis with OSAHS.
Methods
We recruited 196 children ≥5 years old from the otolaryngology outpatient department, who experienced snoring and underwent nasopharynx lateral radiography and in-laboratory polysomnography. We analyzed correlations between the apnea–hypopnea index (AHI) and lowest oxygen saturation (L-SaO2) with age, body mass index (BMI), tonsil size, and adenoidal–nasopharyngeal (A/N) ratio using the Pearson correlation test. Differences in severe OSAHS prevalence, age, AHI, L-SaO2, tonsil size, and A/N ratio between children with and without enuresis were assessed using the chi-square test and t-test. Risk factors of enuresis were analyzed using logistic regression. Follow-up was conducted to assess remission in children with enuresis after adenotonsillectomy.
Results
BMI, tonsil size, and A/N ratio were correlated with AHI and L-SaO2. Severe OSAHS prevalence, AHI, tonsil size, and A/N ratio were higher and L-SaO2 were lower in children with enuresis. Logistic regression showed that BMI, AHI, tonsil size, and sleep apnea were risk factors for enuresis.
Conclusions
Our study findings showed that enuresis was associated with OSAHS in children. Adenotonsillectomy may improve the symptoms of enuresis.
Introduction
Sleep is an essential part of human life. In childhood, good quality sleep accelerates the healthy development of various systems, especially the central nervous system. Therefore, sleep quality is important for children's healthy development. Obstructive sleep apnea–hypopnea syndrome (OSAHS) accounts for about one-quarter of diseases encountered among pediatric otolaryngology (ENT) outpatients, with an incidence of 1% to 3%. 1 However, according to our experience in daily outpatient care, many children with OSAHS have nocturnal enuresis, including older children. However, the correlation between enuresis and OSAHS in children remains unclear.
At present, studies have shown that approximately 10% to 40% of children with OSAHS have enuresis at the same time.2,3 Some scholars also believe that enuresis is a manifestation of OSAHS in children. 4 Alexopoulos et al. 4 showed that people who snore regularly have a higher risk of primary enuresis than those who do not snore. Although OSAHS has been associated with enuresis in population-based studies, the underlying mechanism of enuresis and OSAHS has not been elucidated. Some scholars believe that allergens may cause an allergic reaction, which is mediated by inflammatory cytokines, leading to bladder smooth muscle contraction and a decline of bladder function. 5 Other scholars report that the mechanism is owing to an increased awakening threshold during sleep among children with OSAHS, and that neural stimulation from bladder filling does not wake the child, causing enuresis. 6
In this study, we aimed to analyze the correlation between enuresis and several indicators that are directly related to OSAHS, to explore the relationship between enuresis and OSAHS in children. We discuss potential mechanisms according to the correlation of these indicators.
Methods
Clinical data
In this retrospective study, we enrolled children ≥5 years old who presented with snoring as the chief complaint in the ENT outpatient department of Children’s Hospital, Nanjing Medical University, and who underwent nasopharynx lateral radiography and in-laboratory polysomnography (PSG) between January 2018 and June 2019. Patients were divided into a group with enuresis (n = 45) and a non-enuresis group (n = 151).
We excluded children with craniofacial abnormalities, neuromuscular or genetic diseases, spina bifida, lower urinary tract symptoms other than enuresis (such as daytime incontinence, urgent urination, frequent urination, and endless urination), and bladder dysfunction, diabetes, or diabetes insipidus.
Study procedure
All children in our study underwent in-laboratory PSG (Somté PSG; Compumedic, Victoria, Australia). Children spent the night in the sleep medicine center of our hospital. A sleep monitoring physician in our ENT department was responsible for monitoring children’s sleep.
Parents completed the registration information of their child, including age, height, weight, whether the child was a mouth breather, whether the child experienced apnea during sleep, whether the child had enuresis, as well as other basic information. After collecting participants’ basic information, we calculated body mass index (BMI), based on each child’s reported height and weight. We reviewed the data of nasopharyngeal lateral radiography and PSG in children and conducted telephone follow-up to assess whether adenotonsillectomy had been performed after PSG monitoring in children with enuresis group and whether enuresis had improved after the operation. We then performed statistical analysis on the collected data.
Our study was approved in writing by the institutional ethics committee of Children's Hospital of Nanjing Medical University (approval number 202008077-1). We obtained verbal consent from the parents of children to participate in this study.
Diagnostic criteria
The diagnostic criteria for enuresis was enuresis that occurred twice or more per month in children age 5 to 6 years, and once or more per month in children age 7 years or older and lasting for more than 3 months. 7 The criterion for improved enuresis was no enuresis symptoms for more than 3 months.
Adenoid hypertrophy
The degree of adenoid hypertrophy was evaluated according to the adenoidal-nasopharyngeal (A/N) ratio in nasopharyngeal lateral radiographs. In the A/N ratio, A refers to the vertical distance between the most concave point of the anterior lower margin of the adenoid body and the tangent of the basilar clivus; N refers to the distance between the posterior upper end of the hard jaw and the posterior upper margin of the root of the pterygoid muscles. The higher the A/N ratio, the larger the adenoid size.
Tonsil hypertrophy
According to the traditional tonsil classification method, tonsils that do not exceed the bilateral pharyngopalatine arch are considered grade I tonsillar hypertrophy. If the tonsils exceed the pharyngopalatine arch but do not exceed the uvula, this is considered grade II tonsillar hypertrophy. Tonsils exceeding the uvula are considered grade III tonsillar hypertrophy.
Diagnostic criteria for OSAHS
OSAHS refers to diseases characterized by apnea and hypopnea during sleep, which are caused by the collapse of the upper airway and are accompanied by snoring and decreased blood oxygen saturation (SaO2). OSAHS is usually diagnosed according to the apnea–hypopnea index (AHI), measured using PSG. The AHI refers to the average number of apneas and hypopneas per hour of sleep. Unlike adults, OSAHS in children is diagnosed as AHI >1. OSAHS severity is divided into three degrees, according to the AHI: AHI 1 to ≤5 is considered mild OSAHS, AHI >5 to ≤10 moderate OSAHS, and AHI >10 is considered severe OSAHS. 8
Apnea and hypopnea
Apnea is divided into obstructive apnea, central apnea, and mixed apnea. In obstructive apnea, the oral and nasal airflow is decreased ≥90% lasting ≥2 breath cycles, and there is chest and abdomen movement during the entire apnea event. In central apnea, oral and nasal airflow is decreased ≥90% for 20 s, or ≥2 breath cycles with event-related arousal or ≥3% oxygen desaturation, or ≥2 breath cycles with heart rate reduction to <50 beats/minute lasting at least 5 s, or heart rate <60 beats/minute lasting 15 s in infants under age 1 year only; there is a lack of chest and abdomen movement throughout the event. In mixed apnea, the oral and nasal airflow is decreased ≥90% and lasts ≥2 breath cycles; chest and abdominal movements are both present and absent during the whole event. Hypopnea refers to decreased oral and nasal airflow ≥30% from baseline, lasting ≥2 breath cycles and accompanied by event-related arousal or ≥3% oxygen desaturation. Because an absence of chest and abdominal movement during sleep was very rare among children in our study, the study participants mostly had OSA.
Open-mouth breathing
Open-mouth breathing in sleep refers to breathing through the mouth rather than through the nose during sleep.
Statistical analysis
IBM SPSS, version 22.0 was used to analyze the data (IBM Corp., Armonk, NY, USA). We used the Shapiro–Wilk test to assess the normality of the measured data. Data with a normal distribution were expressed as mean±standard deviation, and the t-test was used for comparisons between groups. The chi-square test was used to determine the significance of count data. Pearson's correlation test was used to assess the correlations between dependent and independent variables, and we performed correlation analysis of risk factors using binary logistic regression. The test level was α = 0.05.
Results
Correlation analysis
Among the 196 children included in the study, the mean age was 7.12±2.03 years; mean BMI was 16.95±3.28 kg/m2, mean tonsil size was 2.09±0.69, and the mean A/N ratio was 0.76±0.08. Pearson's correlation test revealed no significant correlation between age and AHI, L-SaO2; the r value was 0.100 and −0.064, respectively. BMI, tonsil size, and A/N ratio were significantly correlated with both AHI and L-SaO2, as evident in Table 1.
Correlation of age, BMI, tonsil size, and A/N ratio with AHI and L-SaO2.

BMI, body mass index; A/N, adenoidal–nasopharyngeal; AHI, apnea–hypopnea index; L-SaO2, lowest oxygen saturation; SD, standard deviation.
Comparison of severe OSAHS prevalence between children with and without enuresis
Among the 196 enrolled children, 45 had enuresis and 151 did not have enuresis. According to the diagnostic criteria for severe OSAHS, 13 of 45 children with enuresis were diagnosed with severe OSAHS, resulting in a prevalence of 28.9%. Moreover, 1 of the 151 children without enuresis was diagnosed with severe OSAHS, a prevalence of 0.6%. The prevalence of severe OSAHS in children with enuresis was significantly higher than that in the non-enuresis group (P < 0.05).
Comparison of age, AHI, L-SaO2, tonsil size, and A/N ratio between children with and without enuresis
We used the independent-samples t-test to analyze the differences in age, AHI, L-SaO2, tonsil size, and A/N ratio between children with and without enuresis. The results showed that compared with the non-enuresis group, AHI, tonsil size, and A/N ratio were significantly higher, and L-SaO2 significantly lower in the enuresis group (P < 0.05). There was no statistically significant difference in age between the two groups, as shown in Table 2.
Comparison of age, AHI, L-SAO2, tonsil size, and A/N ratio between children with and without enuresis.
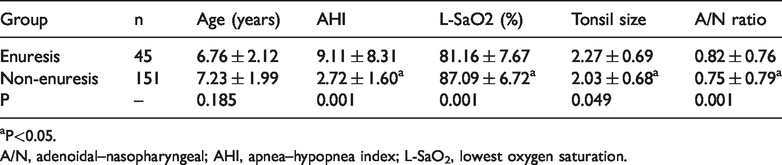
aP<0.05.
A/N, adenoidal–nasopharyngeal; AHI, apnea–hypopnea index; L-SaO2, lowest oxygen saturation.
Results of binary logistic regression
In binary logistic regression analysis, BMI, AHI, tonsil size, and sleep apnea were revealed to be risk factors for enuresis in children (P < 0.05), as shown in Table 3.
Binary logistic regression of enuresis with AHI, L-SaO2, BMI, tonsil size, A/N ratio, open-mouth breathing, and sleep apnea.

aP<0.05.
BMI, body mass index; A/N, adenoidal–nasopharyngeal; AHI, apnea–hypopnea index; L-SaO2, lowest oxygen saturation; SE, standard error; OR, odds ratio; CI, confidence interval.
Effect of adenotonsillectomy in enuresis
In the present study, improvement in enuresis was defined as no enuresis symptoms for more than 3 consecutive months. In telephone follow-up of 45 children with enuresis within 1 year after undergoing PSG, we determined that 30 had adenotonsillectomy after PSG, and 25 had improved enuresis 3 months after surgery. The remaining 15 children who had not undergone adenotonsillectomy still had enuresis (Table 4). The chi-square test showed that the surgical approach could significantly improve enuresis symptoms in children who underwent adenotonsillectomy compared with those who did not. To avoid the influence of other factors on the results, we compared the differences in age, BMI, AHI, L-SaO2, tonsil size, and A/N ratio between the surgery group and non-surgery group; the results showed no statistically significant differences.
Improvement of enuresis in children after adenotonsillectomy.

aP<0.05.
Discussion
OSAHS in children refers to the repeated occurrence of upper airway obstruction during sleep, which leads to blocked ventilation and disturbs the normal sleep structure, thereby causing a series of pathological and physiological changes. 9 At present, the incidence of OSAHS in children (1%–3%) 1 is considered relatively high; OSAHS has become a common problem affecting children's growth and development. The main clinical manifestations of OSAHS in children are snoring, and also include open-mouth breathing, sleep apnea, restless sleep, memory deterioration, inattention, hyperactivity, and daytime sleepiness. Severe OSAHS can affect the growth and development of children, leading to short stature, weakness, or related cardiovascular diseases. 10 Parents of children with OSAHS tend to be most worried about maxillofacial deformity caused by prolonged open-mouth breathing, which is sometimes referred to as “adenoid face”.
The common causes of OSAHS in children include compliance changes caused by increased upper airway resistance, such as allergic rhinitis, nasosinusitis, laryngeal cartilaginous softening, airway stenosis caused by obesity, craniofacial deformity, and similar causes; 11 the most common causes are tonsil hypertrophy and adenoid hypertrophy. According to the Pearson's correlation test and chi-square test, age had no obvious correlation with OSAHS among children in our study. In contrast, BMI, tonsil size, and A/N ratio showed a certain correlation with OSAHS in these children. BMI was positively correlated with OSAHS. Higher BMI indicates that body weight and height are not in harmony; thus, OSAHS is more likely to occur. Tonsil size and A/N ratio were also positively correlated with OSAHS and the A/N ratio had a strong correlation. With larger tonsils and adenoids, we observed higher AHI, lower L-SAO2, and more severe OSAHS. This suggests that tonsil and adenoid hypertrophy seriously affect upper airway ventilation during sleep. These results indicate that BMI and tonsil and adenoid hypertrophy are important factors causing OSAHS in children.
In our pediatric otolaryngology clinic, parents commonly report enuresis symptoms in their children with OSAHS. Nonetheless, it remains unclear why enuresis occurs in these children. According to the International Classification of Diseases, 10th Revision (ICD-10), 7 enuresis is a condition that occurs twice or more per month in children 5 to 6 years old, and once or more per month in children age 7 years and older and that lasts for more than 3 months. In Western countries, 12 approximately 16% of children age 5 years, 10% of children age 7 years, and 5% of children age 11 to 12 years have enuresis. In China, 13 approximately 11.8% of children age 5 years and 4.07% of children age 5 to 18 years have enuresis. Studies also have shown that approximately 10% to 40% of children with OSAHS have enuresis at the same time. The urination process in humans is completed via coordination of the bladder and urethra, under joint regulation by the brain, spinal cord, and peripheral nerves. 14 When the bladder is not completely filled, it stores urine by relaxing the detrusor muscle and contracting the pelvic floor muscles and urethral sphincter. When the bladder is filled, the bladder tension receptors are excited and induce bladder detrusor muscle contraction and urethral sphincter relaxation by stimulating the sacral parasympathetic pathway and somatic nerve pathway, thus promoting urine output.
There are many reasons for enuresis in children, including wakefulness disorder, delayed development, changes in bladder function or pathology, changes in nighttime hormone secretion, psychological disorders, and genetic predisposition, among others. 15 However, it remains unclear why some children with OSAHS have enuresis symptoms. According to our analysis, the prevalence of severe OSAHS in the enuresis group was significantly higher than that in the non-enuresis group. The independent-samples t-test also revealed that AHI, tonsil size, A/N ratio were significantly higher, and L-SaO2 significantly lower, in the enuresis group. According to the degree of severity of OSAHS, the higher AHI, the greater the OSAHS severity. Furthermore, our analysis revealed that more severe OSAHS was associated with a greater likelihood of enuresis. We also found no significant differences in age between the enuresis and non-enuresis groups. In logistic regression analysis, we identified BMI, AHI, tonsil size, and sleep apnea as risk factors for enuresis in children. Although not identified as a risk factor for enuresis in children, the A/N ratio was significantly correlated with AHI; therefore, adenoid size also has a certain impact on enuresis in children.
Considering etiology, a known common cause of enuresis is arousal disorder, which refers to a higher threshold of arousal during sleep and difficulty in awakening. 6 , 15 Our study identified a greater number of apneas during sleep in children with enuresis, and the degree of tonsil adenoid hypertrophy and BMI were also greater. We speculate that this might be owing to upper airway obstruction caused by tonsil and adenoid hypertrophy, obesity, and repeated apnea, which lead to repeated arousal during sleep, and long-term repeated arousal during sleep leads to an increase in children's arousal threshold. A high arousal threshold results in low sensitivity to bladder filling or detrusor contraction, which stimulate the urge to urinate. However, children with OSAHS cannot awaken in time through the usual wake-up mechanism, which eventually leads to enuresis. Endocrine and metabolic disorders are also common causes of enuresis, and an important hormone involved is brain natriuretic peptide. 16 Brain natriuretic peptide is secreted by myocardial cells and promotes the excretion of sodium, thus inhibiting the renal angiotensin aldosterone system, reducing the release of antidiuretic hormone, and promoting urination. 16 We observed that the degree of upper airway obstruction in children with enuresis was more serious. We speculated that repeated upper airway obstruction leads to sleep apnea. At the end of an apnea event, the negative pressure in the chest is increased, systemic venous reflux is increased, left and right ventricular load are increased, acute ventricular load is increased, and atrial wall dilation caused by increased intrathoracic negative pressure—which promotes brain natriuretic peptide release from ventricular myocytes—eventually leads to enuresis.
For children with OSAHS, it has been reported that adenotonsillectomy is a simple and effective method that may alleviate enuresis in this population. 17 In telephone follow-up, we found that the symptoms of enuresis were improved in 83.3% of children who underwent adenotonsillectomy. It is possible that by removing the tonsils and adenoids, upper airway obstruction during sleep is relieved and the occurrence of night apnea is reduced, which in turn leads to a normal arousal threshold and reduced release of brain natriuretic peptide, thereby effectively alleviating enuresis.
The current research has some limitations. First, our study participants were selected from the ENT outpatient department, which would result in a greater proportion of OSAHS among the included children. Additionally, the number of children with enuresis was relatively small; thus, a selection bias is present. Second, the follow-up of children with enuresis was relatively short, and there was no formal evaluation of the effect of treatment for enuresis; further research is needed in this regard. Third, the pathogenesis of enuresis in children with OSAHS must be further verified in animal experiments.
Conclusion
OSAHS is one of the most common diseases observed in pediatric otolaryngology, and enuresis is often overlooked by doctors in children with OSAHS. Our results revealed that enuresis was closely linked to OSAHS in children. BMI, AHI, tonsil size, and sleep apnea were indicators of OSAHS severity, as risk factors for enuresis in children. Adenotonsillectomy may improve the symptoms of enuresis.
Footnotes
Acknowledgements
We wish to thank all patients involved in the study and their families.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.