
Abstract
Background:
High-flow oxygen therapy (HFOT) is increasingly used for acute respiratory failure. Few data support its use at home for the treatment of chronic respiratory failure. Our aim was to report the pattern of the use of long-term HFOT in our center and the outcome of patients setup on long-term HFOT.
Methods:
A retrospective monocentric study including all patients setup on long-term HFOT between January 2011 and April 2018 in Rouen University Hospital was carried out. Patients were divided into two groups, patients with hypoxemic respiratory failure treated with nasal HFOT (nHFOT) and tracheotomized patients treated with tracheal HFOT (tHFOT).
Results:
A total of 71 patients were established on long-term HFOT. Out of these 43 (61%) were included in the nHFOT group and 28 (39%) were included in the tHFOT group. In the nHFOT group, underlying respiratory diseases were interstitial lung disease (n = 15, 35%), pulmonary hypertension (n = 12, 28%), lung cancer (n = 9, 21%), and chronic airway disease (n = 7, 16%). In the tHFOT group, the number of admissions for exacerbation decreased by −0.78 per year (–2 to 0) (p = 0.045). In total, 51 (72%) patients were discharged to their homes and 20 (28%) went to a post-acute re-enablement facility. Median survival following HFOT was 7.5 months. Survival was significantly lower in the nHFOT group with a median survival of 3.6 months whereas median survival was not reached in the tHFOT group (p < 0.001). Monthly costs associated with home delivery of HFOT were €476 (296–533) with significant differences in costs between the nHFOT group of €520 (408–628) and costs in the tHFOT group of €296 (261–475) (p < 0.001).
Conclusions:
The use of long-term HFOT allows very severe patients to be discharged at a reasonable cost from acute care facilities.
The reviews of this paper are available via the supplementary material section.
Keywords
Introduction
Long-term oxygen therapy (LTOT) is the main treatment for severe hypoxemic chronic respiratory failure. It has been demonstrated that LTOT improves survival in chronic obstructive pulmonary disease (COPD) patients.1,2 Its use has been extended to other etiologies of chronic respiratory failure, associated or not with home mechanical ventilation. At home, LTOT is delivered using continuous or pulse flow through an oxygen concentrator or a liquid oxygen reservoir.3–5
High-flow oxygen therapy (HFOT) is a recent approach that aims to optimize oxygen delivery using specific devices. These devices can generate up to 60 l/min of heated and humidified air enriched with oxygen. The inspired fraction of oxygen (FiO2) varies from 21–100% through a blender linked to an active humidifier. HFOT is now widely used in intensive care units for the management of acute hypoxemic respiratory failure because it reduces intubation rates. 6
To date, trials supporting the use of HFOT at home only included patients with obstructive lung disease.7,8 Their results suggested a benefit that needs to be confirmed by larger randomized controlled trials (RCTs). However, for some patients, low flow LTOT is not sufficient to allow a safe return to their homes. In these cases, HFOT could be an interesting option. In addition to a better oxygenation, HFOT decreases the work of breathing.9–11 and improves dyspnea. 12 Therefore, in our center, it has been used for patients with end-stage hypoxemic respiratory disease as part of palliative management and in order to allow discharge to home.
In our center, HFOT has also been proposed for tracheostomized patients that are frequently admitted for low respiratory tract infections and that have secretion management issues. For these patients, HFOT was offered because it improves ciliary clearance, 13 reduces the number of tracheal aspiration, 14 generates a positive expiratory pressure, 15 increases end-expiratory lung volumes, 16 and reduces the number of exacerbations in patients with bronchiectatic diseases. 17
The primary aim of our study was to describe the pattern of use of long-term HFOT in our center. The secondary aims were to describe the outcome of patients initiated on home HFOT and the costs associated with home delivery of HFOT.
Methods
We conducted a retrospective single-center study that included all patients initiated on HFOT between January 2011 and April 2018 at Rouen University Hospital. The study was approved by the Rouen University Hospital ethical committee for retrospective studies (E2018-61). Given the retrospective design of the study and the use of data already available in the patient’s medical records, the need for consent was waived by the ethics committee.
In order to identify patients established on HFOT following an acute respiratory failure, we retrieved all HFOT prescriptions made to the main local home care provider (ADIR assistance, Asten, Isneauville, France). We then identified patients that had their follow up in our center. We performed a medical review of all electronic medical records and included all patients that had HFOT prescribed at home or in a post-acute re-enablement unit. We excluded patients for whom HFOT was prescribed but who died before discharge and those who did not have any follow up in our hospital. For patients included in the study, we collected the following data using electronic medical records: gender, age, height, weight, underlying respiratory disease, smoking history, smoking status at HFOT setup, and treatments. We retrieved the last available lung function tests and echocardiography before HFOT initiation. We collected results of arterial blood gas prior to initiation of HFOT and arterial blood gas on HFOT at discharge. Previous admissions were collected from electronic medical admission registers, as well as those that followed HFOT initiation. HFOT discharge settings were established by the medical team in charge of the patient. HFOT was chosen in order to ensure sufficient oxygenation and adapted to the patient’s tolerance. There was no specific protocol to determine home settings. For all following admissions, we reviewed the discharge summary to ascertain that admission was related to acute exacerbation. Acute exacerbation was defined by a worsening of respiratory symptoms associated with a change or increase in sputum color or production, and fever, abnormal chest X-Ray, or both. For all patients, all causes of acute dyspnea were overruled by the in charge physician. For patients where survival or follow up was shorter than 1 year, the number of exacerbations at 1 year follow up was calculated as follows, (number of admission during follow up/number of days of follow up) × 365. Survival data were obtained from the home care provider.
Patients were divided into two groups: patients with HFOT delivered through a nasal cannula (nHFOT) and patients with HFOT delivered through a tracheostomy cannula or a tracheal mask positioned in front of a tracheostomy cannula (tHFOT). In the nHFOT group, HFOT was initiated for oxygenation purposes. A subgroup survival analysis was performed according to the underlying pulmonary disease, interstitial lung disease, pulmonary hypertension, lung cancer, and chronic airway disease (including COPD, COPD associated with pulmonary hypertension and diffuse bronchiectasis). Only one patient had a rapidly progressive neuromuscular disease and was included in the cancer subgroup. In the tHFOT group, HFOT was initiated for humidification purposes. In this group, we assessed the number of hospitalizations related to a chest infection in the year prior to the admission and in the year following HFOT initiation. Survival was assessed in September 2018. Health costs were assessed from the home healthcare provider’s point of view because there is no reimbursement scheme for HFOT in France. The home healthcare provider does not charge patients for HFOT delivery. HFOT costs were evaluated using the daily amortization costs, a monthly rate for consumables, and home visits performed by technicians. Oxygen costs were calculated according to the French National LTOT tariff. We were not able to include data regarding electricity costs.
Continuous data are presented as mean and standard deviation when normally distributed or median and interquartile when nonnormally distributed. Categorical data are presented as frequency counts and percentages. Comparisons were performed using the Kruskal–Wallis test, chi-squared test, and the Mann–Whitney test, as appropriate. Survival data were analyzed using the Kaplan–Meier method and log-rank test. For all tests, the significance level was set at 0.05. Analyses were performed using Prism v6.0(h) (GraphPad Software, La Jolla, CA).
Results
We retrieved 121 HFOT consecutive prescriptions. Out of those, 71 (59%) were included in our study (Figure 1). In total 43 (61%) patients were included in the nHFOT group. The underlying respiratory diseases were interstitial lung disease (n = 15, 35%), pulmonary hypertension (n = 12, 26%), lung cancer (n = 9, 21%), and chronic airway disease (n = 7, 19%). A total of 28 patients were included in the tHFOT group. The reasons for tracheostomy were neuromuscular disease (n = 12, 40%), chest-wall disease (n = 8, 30%), cancer (n = 4, 15%), and chronic airway disease (n = 4, 15%). Patients characteristics at the initiation of HFOT are summarized in Table 1. Since 2011, the number of prescriptions of home HFOT increased annually by 96%. The HFOT devices were Airvo® (Fisher & Paykel®, Auckland, New Zealand) for 19 (27%) patients and Airvo2® (Fisher & Paykel®) for 52 (73%) patients. Patients characteristics and HFOT settings at discharge are summarized in Table 1. Arterial blood gas prior to and after home HFOT initiation are reported in Table 2. When considering only patients who had a baseline PaCO2 > 6 kPa, PaCO2 decreased significantly on HFOT with a median reduction of −0.51 kPa (–1.44–0.1) (p = 0.034). Similarly, HFOT did not improve PaO2 significantly: 0.00 kPa (–0.60–1.56) (p = 0.397) in the overall population. In a subgroup analysis of patients that required oxygen supplementation on their HFOT, PaO2 improvement on HFOT was: +0.43 kPa (–0.48–1.81) (p = 0.782).

Flow chart for inclusion.
Patient’s characteristics at baseline, according to the study group.
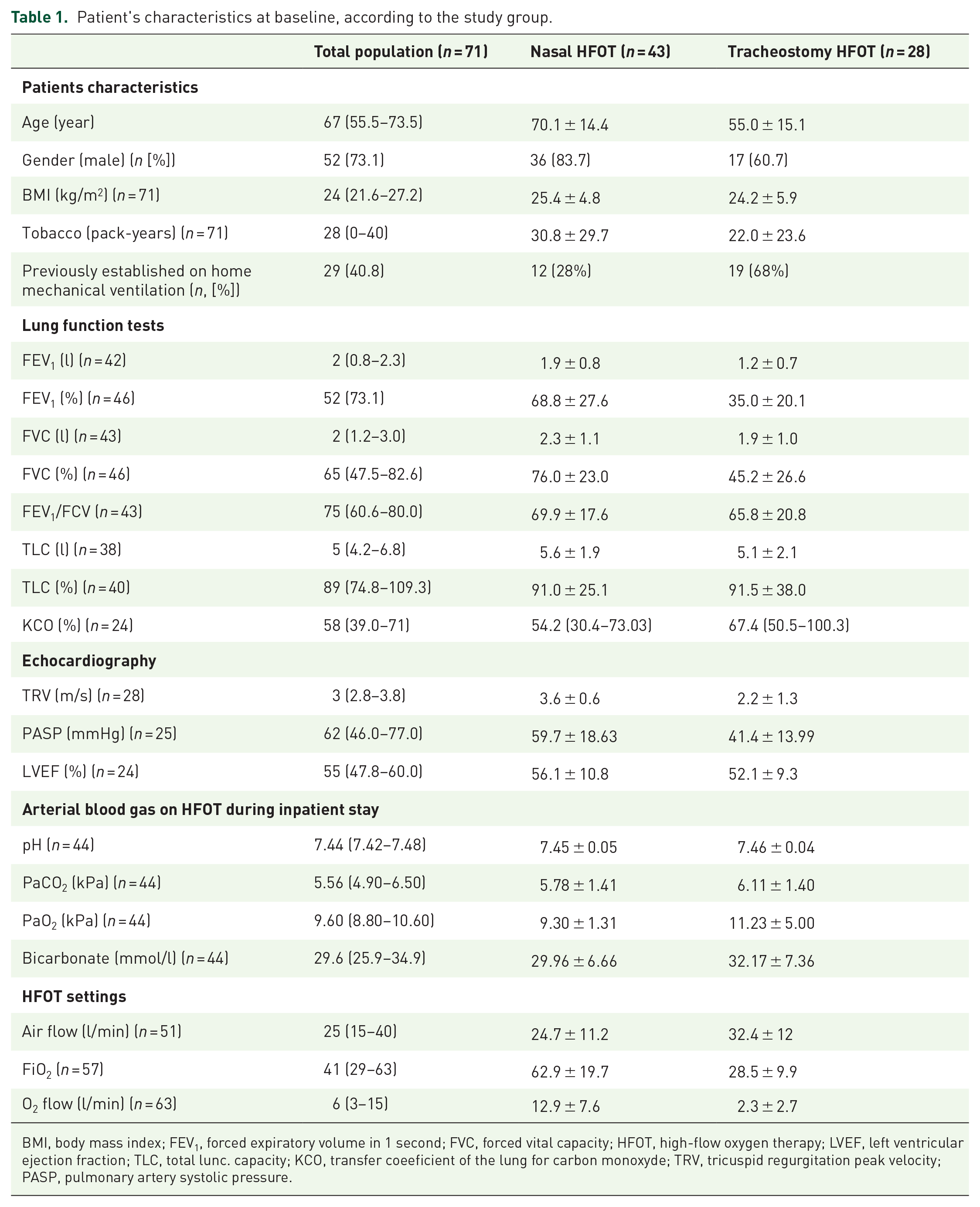
BMI, body mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; HFOT, high-flow oxygen therapy; LVEF, left ventricular ejection fraction; TLC, total lunc. capacity; KCO, transfer coeeficient of the lung for carbon monoxyde; TRV, tricuspid regurgitation peak velocity; PASP, pulmonary artery systolic pressure.
Patients arterial blood gas prior to and following home HFOT therapy initiation.

HFOT, high-flow oxygen therapy; FiO2, fraction of inspired oxygen.
In the tHFOT group, the number of exacerbations decreased significantly, –0.79 per year (−2 −0) (p = 0.045) following HFOT initiation.
In the overall population, median survival under HFOT was 7.5 months. Survival was significantly lower in the nHFOT group with a median survival of 3.6 months after HFOT initiation when median survival was not reached in the tHFOT group (p < 0.001) (Figure 2). Subgroup analysis in the nHFOT group showed that median survival was 1 month for lung cancer patients, 2.7 months for patients with interstitial lung disease patients, and 30.2 months for patients with pulmonary hypertension.
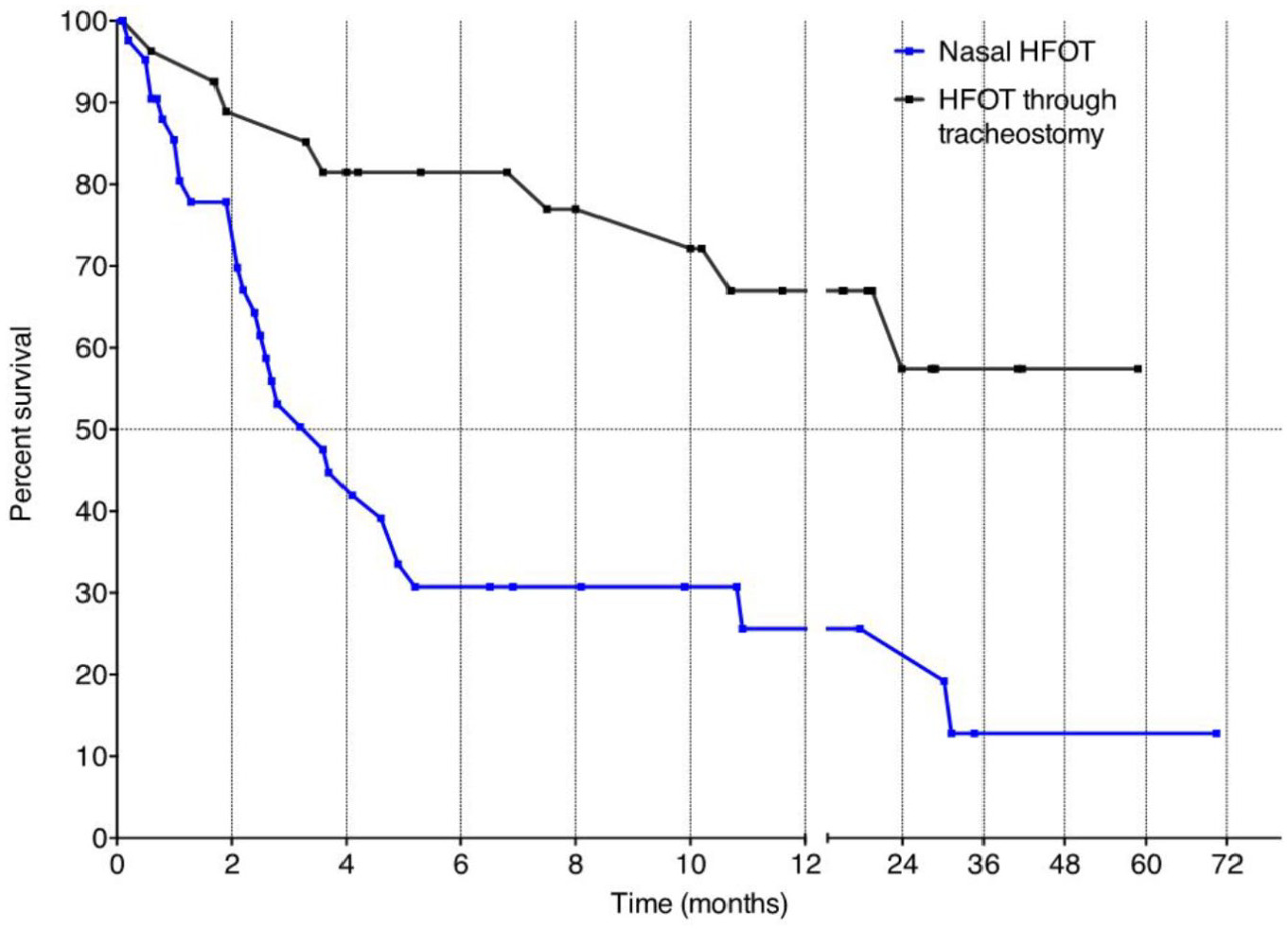
Probability of survival in months according to the use of HFOT through the nose or the tracheostomy (p < 0.001, log-rank).
After HFOT initiation, 51 (72%) patients returned home and 20 (28%) were admitted to a post-acute re-enablement unit and then a long-term care facility. For the 51 patients discharged to their homes, 31 (61%) were in the nHFOT group and 20 (39%) in the tHFOT group. For the 51 patients discharged to their homes, 28 (55%) required a liquid oxygen installation, 15 required (30%) oxygen concentrators and 7 (15%) did not require any oxygen. For those who required liquid oxygen, the median number of liquid oxygen tanks installed was 4 (3–4). The median FiO2 was 63% (47–76) in the nHFOT group and 23% (21–30) in the tHFOT group (p < 0.001). The length of stay at home was 29.3 weeks (11.6–73.3) in the overall population with the difference between groups, 15.7 weeks (0.3–35.1) in the nHFOT group and 65.9 weeks (30.7–122) in the tHFOT group (p < 0.001).
The cost of HFOT setup without any oxygen supplementation was estimated at €231 for the first month of use. In the overall population, including costs associated with oxygen delivery, the total cost of HFOT setup was €2455 (1337–4995) with significant differences between groups, €1712 (1174–3177) in the nHFOT group and €4005 (2291–9931) in the tHFOT group (p = 0.009). Monthly costs for HFOT were €476 (296–533) in the overall population with significant differences between groups, €520 (408–628) in the nHFOT group and €296 (261–475) in the tHFOT group (p < 0.001). HFOT contributed to 59 ± 25% of the total cost for the home care provider in the overall population with significant differences between groups, 48 ± 20% in the nHFOT group and 75 ± 22% in the tHFOT group (p < 0.001).
In total, four patients were discontinued from nHFOT and one patient with interstitial lung disease did not tolerate HFOT because of warmness. Overall, three patients improved after the acute episode, one with lung cancer who had been established on HFOT following complete lung atelectasis that resolved after PD-L1 immunotherapy with complete oxygen weaning and two with pulmonary hypertension who improved sufficiently to be switched to standard LTOT.
Discussion
Our study reports the largest cohort of patients treated with HFOT at home or in a post-acute re-enablement facility. In patients with end-stage respiratory failure and high oxygen requirements, survival was poor but HFOT allowed patients to return home. In tracheostomized patients admitted for lower respiratory tract infections, the use of HFOT may have lowered exacerbation rate after HFOT initiation.
In our cohort, HFOT was used to treat end-stage hypoxemic respiratory failure in severe patients. Given the retrospective design of our study, we were not able to assess the quality of life of these patients. However, as part of our clinical practice, we only offered discharge with home HFOT for patients who wanted to return home. All but one patient tolerated HFOT well enough to use it at home. In the nHFOT group patients that were discharged to their homes (n = 31) the median FiO2 was 63%. This highlights the severity of their respiratory diseases and they would not have been able to be discharged on low flow LTOT. With a median length of stay at home of 15.7 weeks, we believe that HFOT allowed these 31 patients to spend a meaningful length of time at home. This result needs to be supported by prospective trials focused on patient-centered outcomes.
To the best of our knowledge, our cohort is the first to report the use of such a high FiO2 in the home settings. The technical and organizational challenges need to be overcome to achieve such levels of oxygenation in the home setting. Usually, LTOT is provided through a concentrator or a tank to store liquid oxygen. In our cohort, patients had a median number of four liquid oxygen tanks. Each tank requires 1 m2 of room space to be stored safely in the patient’s homes. As patients with chronic respiratory failure often have limited income, such devices may not be installed in every household. As HFOT devices are not provided with a built-in battery, electrical back-up also needs to be installed in patient’s houses.
In our cohort, HFOT associated total cost was €1712 per patient in the nHFOT group. Our study was not designed to assess cost-effectiveness. However, the individual cost appears to be significantly lower than the cost that would have been associated to an inpatient stay until the patients died. For patients with tHFOT, monthly costs were lower given the lower oxygen requirements. In the tHFOT group, the total cost per patient was higher given the longer period of use of HFOT. In patients with nHFOT, the costs are driven by oxygen delivery costs. Costs of HFOT without any oxygen delivery are acceptable at €261 per month.
Our study was not designed to assess the efficacy of HFOT in an exacerbation. The pre and post-analysis suggested a reduction in the number of admissions for low respiratory tract infection following initiation of tHFOT. Therefore, the cost of HFOT may be counterbalanced by a lower readmission rate. The reality of the reduction of exacerbation, as well as the cost-effectiveness of such an approach, needs to be assessed more thoroughly. This reduction in the number of admissions has been achieved with a higher delivered airflow than the one reported in most clinical trials.16,18,19 Given the design of our study, we were not able to assess any correlation between the level of flow and the number of exacerbations.
Patients included in our cohort were all characterized by severe pulmonary disease or respiratory muscle weakness. Therefore, our patients were more severe than those included in RCTs evaluating the benefit of home HFOT. Of interest, the subgroup of patients with hypercapnia at baseline had a similar PaCO2 improvement on HFOT to that seen in published trials.7,20 In our hypercapnic subgroup, PaCO2 improved by 0.51 kPa. This improvement corresponds to the cutoff usually used to assess the clinical effectiveness of noninvasive ventilation.21,22 However, appropriately titrated noninvasive ventilation achieved a larger decrease in PaCO2 level in COPD patients.23,24
Our study has limitations given its retrospective design and the heterogeneity of our cohort that included patients with severe respiratory disease of variable etiology and patients with muscular weakness. However, it provides real-life data on the management and the outcome associated with the use of HFOT outside a hospital. Unfortunately, the heating temperature of the HFOT was not recorded. Given its retrospective design, we were not able to do any sample size calculation. Our findings provide preliminary data on the use of HFOT at home that will be useful to perform sample size calculations in future prospective trials.
Our use of HFOT depicts two distinct clinical situations, patients with severe hypoxemia and tracheostomized patients. In the first group, we would suggest assessing the benefit of HFOT on symptoms and quality of life. In the first group, the main challenge is to provide at home quantity of oxygen and requires expert home healthcare providers. In the second group, we included patients with recurrent admissions for severe exacerbation and with secretion management issues. We would, therefore, suggest targeting readmission rates in further studies. In that group, the technical challenges are limited.
Conclusion
HFOT is a feasible technology at home and in post-acute re-enablement facilities for patients with end-stage hypoxemic lung disease and for tracheostomized patients with severe exacerbations. Associated costs with its use are reasonable. However, further prospective clinical trials are required to assess the efficacy and the cost-efficiency of such management as well as its effect on health-related quality of life.
Supplemental Material
Author_Response_1 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Author_Response_1 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_2 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Author_Response_2 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_3 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Author_Response_3 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Reviewer_1_v.1 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Reviewer_2_v.1 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.2 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Reviewer_2_v.2 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.3 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Reviewer_3_v.3 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.4 – Supplemental material for Characteristics and outcome of patients set up on high-flow oxygen therapy at home
Supplemental material, Reviewer_3_v.4 for Characteristics and outcome of patients set up on high-flow oxygen therapy at home by Samuel Dolidon, Johann Dupuis, Luis-Carlos Molano Valencia, Mathieu Salaün, Luc Thiberville, Jean-François Muir, Antoine Cuvelier and Maxime Patout in Therapeutic Advances in Respiratory Disease
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
Dr Dolidon reports non-financial support from Asten and LVL outside the submitted work.
Johan Dupuis is an employee from ADIR Assistance, Asten. Drs Molano Valencia, Salaün, Muir, and Cuvelier have no conflicts of interest to disclose. Dr Patout reports personal fees from Resmed, grants and nonfinancial support from Fisher & Paykel, nonfinancial support from MSD, nonfinancial support from Asten, grants from ADIR Association, grants from B&D Electromedical, personal fees from Philips Respironics, personal fees and nonfinancial support from Chiesi outside the submitted work. Jean-François Muir is the president of ADIR Association.
Supplemental material
The reviews of this paper are available via the supplementary material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.