
Abstract
Objective
To evaluate the therapeutic effects of high-flow nasal cannula (HFNC) oxygen therapy in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and type II respiratory failure.
Methods
Seventy-two patients with AECOPD and type II respiratory failure were randomly allocated to an HFNC oxygen therapy trial group or a non-invasive positive-pressure ventilator therapy (NIPPV) control group. Their arterial blood gas parameters and comfort, evaluated using a questionnaire, were compared before and after the therapeutic interventions.
Results
The PaCO2 and blood
Conclusions
HFNC has a good therapeutic effect in patients with AECOPD and type II respiratory failure. It improves patient comfort and has clinical value.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is currently the most common chronic respiratory disease and has become a significant public health issue because of its high prevalence and the associated disability, morbidity, and mortality. It is characterized by airflow limitation with persistent and progressive dyspnea and is often accompanied by chronic coughing and chest tightness.1–2 Acute exacerbations of COPD (AECOPD) are more common in middle-aged and older patients, often occur in combination with type II respiratory failure, and are characterized by weak coughing, concomitant infection, and poor lung function, which have negative effects on patient health, and increase the risks of hospitalization, readmission and disease progression. As AECOPD worsens, CO2 retention and hypercapnic respiratory failure may occur.3–4 Therefore, the treatment of AECOPD in combination with type II respiratory failure requires treatment by mechanical ventilation and rational oxygen therapy, according to the physiological and pathological characteristics of the patient.
Patients with AECOPD in combination with type II respiratory failure are often treated using non-invasive positive-pressure ventilation (NIPPV), which is relatively non-invasive and significantly improves oxygenation.5–6 However, NIPPV can cause respiratory discomfort, owing to compressive skin damage and gas-related drying associated with the mask. In addition, a large amount of mask leakage may occur in some patients because of poor fit associated with certain facial shapes, necessitating an escalation of respiratory support if patients have unrelieved symptoms of hypoxia and CO2 retention.
High-flow nasal cannula (HFNC) oxygen therapy is a novel non-invasive respiratory support technique that provides patients with warm, humidified oxygen at a high flow rate through a thick nasal catheter. This method is associated with high levels of comfort and tolerance, and this mode of respiratory support has been widely used globally in recent years.7–8 However, the advantages of HFNC therapy for patients with AECOPD have not been fully elucidated. Therefore, in the present study, we evaluated the clinical efficacy and patient comfort levels associated with the use of HFNC therapy in patients with AECOPD in combination with type II respiratory failure, to provide a theoretical basis for the clinical use of this therapy.
Patients and Methods
General information
Patients with AECOPD and type II respiratory failure who were admitted to the intensive care unit of Hai'an People's Hospital between January 2018 and May 2021 were selected for the study. Using a random number table, they were allocated to experimental and control groups. The experimental group was treated with HFNC oxygen therapy, while the control group was treated with NIPPV.
We included patients who met the diagnostic criteria for AECOPD (updated 2017), 9 had Global Initiative for Chronic Obstructive Lung Disease stage I–III, were >45 years old, had an arterial partial pressure of oxygen (PaO2) <60 mmHg (or oxygenation index <300 mmHg under oxygenation) and had an arterial partial pressure of carbon dioxide (PaCO2) >50 mmHg.
We excluded patients with the following conditions: cardiac or respiratory arrest requiring emergency tracheal intubation with invasive mechanical ventilation; coma; ventilatory dysfunction; very severe type I respiratory failure (oxygenation index <60); hemodynamic instability; altered mental status or inability to cooperate; predisposition toward aspiration of foreign material; dense, voluminous secretions; craniofacial trauma or burns; fixed nasal foreign body; and recent facial or gastro-esophageal surgery.
Treatments
The control group was treated with NIPPV using a bilevel positive airway pressure ventilation model. The initial inspiratory positive airway pressure was 8 to 10 cmH2O and that of expiratory positive airway pressure was 4 to 6 cmH2O. The inhaled oxygen concentration was maintained at 30%–50%. Continuous oxygen inhalation for >16 h was administered daily. These parameters were adjusted according to the participants’ vital signs and blood gas data, which were closely monitored, and if their condition worsened, more invasive positive-pressure ventilation was performed.
The experimental group was treated by transnasal high-flow humidified oxygen therapy using an Optiflow transnasal high-flow humidified oxygen therapy system (Fisher-Paykel, Auckland, New Zealand), with parameters of 30% to 50% inhaled oxygen concentration, a flow rate of 40 to 60 L/min, a temperature of 37°C and a relative humidity of 100%. The parameters were also adjusted according to the participants’ blood gas analysis data and vital signs, and more invasive positive-pressure ventilation treatment was performed in those who deteriorated.
Measurements made
Arterial blood was collected from participants on an empty stomach before and after treatment to measure pH, PaCO2, PaO2, oxygenation index (PaO2/FiO2) and
Evaluation of patient comfort
Patient comfort was assessed using the Pulmonary Function Status and Dyspnea Questionnaire (PFSDQ), 10 which was completed once before treatment and once 3 months following treatment. The questionnaire included three domains: change in daily activity (CA), dyspnea (DA), and experience (EA), with scores of 0 to 10 for each domain. The participants awarded the scores, with 0 being the least severe, with little change in daily activities and no shortness of breath, fatigue, or discomfort, and 10 being the most severe, with particularly severe breathing problems, shortness of breath, fatigue during daily activities, and extreme discomfort during treatment.
Ethics
The study was approved by the Medical Ethics Committee of Hai'an People's Hospital on June 1, 2018 (approval number: HKL201839). The patients or their guardians provided their written informed consent. The reporting of this study conforms to the CONSORT guidelines. 11
Statistical methods
SPSS v. 19.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Student’s t-test and the rank-sum test were used to analyze continuous data, and the chi-square test was used to analyze categorical data. Statistical significance was set at P < 0.05. We did not perform a sample size calculation.
Results
Participant characteristics
Seventy-two patients were studied, with n = 36 per group. The general characteristics of the participants in both groups are shown in Table 1. The two groups did not differ significantly in terms of sex, age, duration of disease, or the prevalences of underlying conditions (P > 0.05).
Comparison of the general characteristics of the two groups.

Data are mean ± SD or median (interquartile range).
HFNC, high-flow nasal cannula; non-invasive positive-pressure ventilator.
Comparisons of the blood gas data and intubation rates before and after treatment
The blood gas indices before and after treatment of the two groups are shown in Table 2. The blood gas analysis showed no statistically significant differences in the pH, PaCO2, PaO2, PaO2/FiO2, or
Comparison of the specified blood parameters between the two groups before and after treatment.
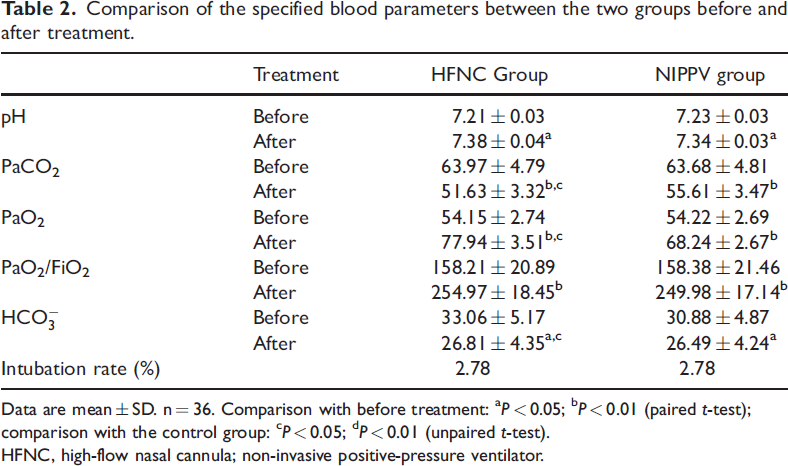
Data are mean ± SD. n = 36. Comparison with before treatment: aP < 0.05; bP < 0.01 (paired t-test); comparison with the control group: cP < 0.05; dP < 0.01 (unpaired t-test).
HFNC, high-flow nasal cannula; non-invasive positive-pressure ventilator.
Comparison of the comfort level before and after treatment
The data collected using the questionnaire before and after treatment for the two groups are shown in Table 3. There were no significant differences in CA, DA or EA between the groups before treatment, but all of these were significantly lower following treatment (P < 0.05 or 0.01), and the CA and EA showed larger decreases in the HNFC group than in the NIPPV group (P < 0.05).
Comparison of the comfort levels of the two groups before and after treatment.

Data are mean ± SD. n = 36. Comparison with before treatment: aP < 0.05; bP < 0.01 (paired t-test); comparison with the control group: cP < 0.05; dP < 0.01 (unpaired t-test).
HFNC, high-flow nasal cannula; non-invasive positive-pressure ventilator; CA, daily activity; DA, dyspnea; EA, experience.
Discussion
The progression of COPD is often accelerated by respiratory infections, and AECOPD ultimately leads to respiratory failure and severe ventilatory dysfunction, which represents the final stage of the disease. In such patients, mechanical ventilation and rational oxygen therapy are typically used as treatments. 12 HFNC has been shown to have beneficial effects in patients with stable COPD, in whom the external positive end-expiratory pressure (PEEP) effect can offset the endogenous PEEP. The flushing effect of HFNC on nasopharyngeal dead space optimizes ventilatory efficiency and promotes CO2 expulsion. In addition, a sufficient level of warm air-flow reduces inspiratory resistance, prevents dry air-induced bronchoconstriction and improves pulmonary mucosal ciliary clearance. Therefore, HFNC can be highly beneficial in the management of AECOPD, mainly because of the significantly higher comfort, compared with NIPPV.12–14 Therefore, in the present study, we evaluated the blood gas data, intubation rate, and comfort of patients before and after HFNC therapy for AECOPD in combination with type II respiratory failure, to provide a basis for its clinical use.
Wenyun et al.
15
showed that respiration and the circulation are stimulated when the PaO2 decreases and the PaCO2 increases. Specifically, the heart and respiratory rates increase, the cardiac blood displacement and cardiac load also increase, and blood pressure shows an abnormal increase, owing to early respiratory acidosis. When the PaO2 decreases and the PaCO2 increases to within a certain range, respiration and the circulation are impaired, involving reductions in the heart and respiratory rates, lower blood pressure, and complications such as pulmonary encephalopathy, pulmonary heart disease, and cardiac arrest in severe cases.15–16 We found that the pH, PaO2, and PaO2/FiO2 of patients with AECOPD in combination with type II respiratory failure were higher after treatment with nasal high-flow humidified oxygen therapy. In addition, their
In the present study, only one participant in each group required intubation, and most were able to largely recover in terms of their respiratory and circulatory function by the end of the treatment period. Patients undergoing HFNC therapy were more comfortable and had a better experience than those undergoing NIPPV. This may be because the HFNC nasal cannula is soft, fits well, and does not require sealing or specific parameter-setting by the operator. Therefore, adverse effects such as claustrophobia and abdominal distension do not occur. 17 In addition, compared with NIPPV, HFNC can improve the comfort of patients by making it easier for them to drink, eat, remove sputum, and communicate; and it is also not associated with pain around the nose, which is caused by tight masks and fixed headbands.18–19 We evaluated the comfort of the participants before and after treatment by assessing their pulmonary function and dyspnoea, using a questionnaire regarding CA, DA and EA. After treatment, the CA and EA scores of the HFNC group had decreased significantly and to a greater extent than those of the control NIPPV group. The DA scores of the HFNC group were also somewhat better than those of the NIPV group, indicating that HFNC treatment significantly improves the comfort of patients.
In conclusion, transnasal high-flow humidified oxygen therapy improves the blood gas parameters and comfort of patients with AECOPD and type II respiratory failure. The findings of the present study provide a theoretical basis for the clinical use of this treatment. However, the sample studied was relatively small; therefore, further studies of larger samples are needed to corroborate our conclusions. In addition, we did not assess conditions other than AECOPD, such as pneumonia, pulmonary edema, heart failure, and pulmonary hypertension, which may also have led to some bias. Furthermore, we did not follow the participants for a long period of time following the treatment, and therefore future studies should involve longer-term follow-up, to more fully determine its effects on the clinical outcomes of patients. Finally, we only assessed certain clinical parameters and the subjective experiences of the participants. Therefore, research regarding the mechanisms involved and the pathophysiology may be needed.
Footnotes
Author Contributions
AL: Conceptualization, Methodology, Formal analysis, Data curation, Writing–original draft preparation. YZ: Investigation, Writing–Review & Editing, Project administration, Funding acquisition. ZP: Validation, Investigation, Visualization.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The research was supported by the Fund of Science and Technology Bureau of Nantong City, Jiangsu Province (JCZ2022122).