
Abstract
Background:
High-flow nasal cannula (HFNC) and conventional oxygen therapy (COT) are important respiratory support strategies for acute hypoxemic respiratory failure (AHRF) in coronavirus disease 2019 (COVID-19) patients. However, the results are conflicting for the risk of intubation with HFNC as compared to COT.
Objectives:
We systematically synthesized the outcomes of HFNC relative to COT in COVID-19 patients with AHRF and evaluated these outcomes in relevant subpopulations.
Design:
This study was designed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources and methods:
We searched PubMed, EMBASE, Web of Science, Scopus, ClinicalTrials.gov, medRxiv, BioRxiv, and the Cochrane Central Register of Controlled Trials for randomized controlled trials and observational studies that compared the efficacy of HFNC with COT in patients with COVID-19-related AHRF. Primary outcomes were intubation rate and mortality rate. Secondary outcomes were the ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2), respiratory rate, hospital length of stay, intensive care unit (ICU) length of stay, and days free from invasive mechanical ventilation.
Results:
In total, 20 studies with 5732 patients were included. We found a decreased risk of requiring intubation in HFNC compared to COT [odds ratio (OR) = 0.61, 95% confidence interval (CI): 0.46–0.82, p = 0.0009, I2 = 75%]. Similarly, we found HFNC was associated with lower risk of intubation rate compared to COT in the subgroup of patients with baseline PaO2/FiO2 < 200 mmHg (OR = 0.69, 95% CI: 0.55–0.86, p = 0.0007, I2 = 45%), and who were in ICU settings at enrollment (OR = 0.57, 95% CI: 0.38–0.85, p = 0.005, I2 = 80%). HFNC was associated with an improvement of PaO2/FiO2 and respiratory rate compared to COT. The use of HFNC compared to COT did not reduce the mortality rate, days free from invasive mechanical ventilation, hospital length of stay, or ICU length of stay.
Conclusion:
Compared to COT, HFNC may decrease the need for tracheal intubation in patients with COVID-19-related AHRF, particularly among patients with baseline PaO2/FiO2 < 200 mmHg and those in ICU settings.
Trial registration:
This systematic review and meta-analysis protocol was prospectively registered with PROSPERO (no. CRD42022339072).
Introduction
The severe acute respiratory syndrome coronavirus 2 pandemic has impacted the healthcare system and produced a substantial proportion of patients who are critically ill with mild-to-severe acute hypoxemic respiratory failure (AHRF).1–3 Over successive waves, most patients admitted to the hospital with coronavirus disease 2019 (COVID-19) have required COT which includes nasal cannula, venturi mask, simple face mask, non-rebreather mask (NRM), rebreather mask, or a combination of them. Additional noninvasive respiratory support strategies, such as high-flow nasal cannula (HFNC), continuous positive airway pressure, and noninvasive ventilation (NIV), are attractive treatment options that could avoid the need for invasive mechanical ventilation.4–6
HFNC is a noninvasive respiratory support modality that delivers warm, humidified oxygen at a maximum flow rate of 60 L/min and up to 100% of the inspired oxygen fraction (FiO2) through nasal probes. 7 It is able to deliver adequately heated and humidified medical gas at a high flow rate, and it has a number of physiological advantages over COT, including reduced anatomical dead space, PEEP, constant FiO2, and good humidification. 8
HFNC is a well-tolerated and effective respiratory support technique that is associated with a reduction in oxygenation failure compared to COT.9,10 However, in patients with COVID-19-related AHRF, the results for the risk of intubation with HFNC as compared to COT are conflicting,11–27 and most studies have not reported improved survival with HFNC.11–14,16–24,26 Two recent randomized controlled trials (RCTs)11,12 and five retrospective observational studies13–17 have suggested a decreased risk of intubation with HFNC relative to COT. However, five other RCTs (including one large-sample RCT)18–22 and five retrospective observational studies23–27 did not report a significant difference in intubation rates between HFNC and COT. The optimal initial method (HFNC versus COT) to provide oxygen support to patients with COVID-19-related AHRF is subject of significant controversy. To the best of our knowledge, conclusive data to compare the impact of HFNC and COT on patients with COVID-19 are still lacking. Here, we conducted a systematic review and meta-analysis of clinical trials comparing HFNC and COT to assess the effects of HFNC on the risk of intubation for patients with COVID-19-related AHRF.
Methods
Search strategy
We conducted a systematic review in accordance with the methods recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 28 Two authors (WT and JCW) searched PubMed, EMBASE, Web of Science, Scopus, ClinicalTrials.gov, medRxiv, BioRxiv, and the Cochrane Central Register of Controlled Trials for eligible studies from 1 January 2020, to 1 October 2022.
We searched for studies that referred to adult COVID-19-related AHRF patients treated with HFNC compared to COT using the key words ‘HFNC’ OR ‘high-flow nasal cannula’ OR ‘high-flow nasal oxygen’ OR ‘high-flow oxygen’ AND ‘conventional oxygen therapy’ OR ‘standard oxygen therapy’ OR ‘low-flow nasal cannula’ OR ‘mask’ OR ‘face mask’ OR ‘oxygen masks’ AND ‘COVID-19’ OR ‘SARS CoV 2’ OR ‘2019 Novel Coronavirus’ OR ‘2019 nCoV’ OR ‘Coronavirus Disease 2019’ OR ‘Coronavirus Disease 19’ OR ‘Severe Acute Respiratory Syndrome Coronavirus 2 Infection’ OR ‘SARS Coronavirus 2 Infection’ OR ‘COVID 19 Pandemic OR COVID-19’, with the detailed search strategy available in the appendix (Supplemental Appendix, p. 2). The language of publication was restricted to English, and the geographical location was not limited.
Study selection
We included all RCTs and observational studies that met the following criteria: (1) population: adult patients (⩾16 years old) confirmed to have COVID-19 by polymerase chain reaction; (2) intervention: HFNC compared with COT. COT stands for conventional oxygen therapy which includes nasal cannula, venturi mask, simple face mask, NRM, rebreather mask, or a combination of them; and (3) predefined outcomes: intubation rate, mortality rate, or both. To evaluate the effects of HFNC and COT on the intubation risk for adult patients with COVID-19, we excluded studies where (1) patients did not meet the screening criteria, (2) the reports were not published in English or were commentaries, reviews, or duplicate publications from the same study, or (3) data could not be extracted by the reported statistical methods or non-targeted outcomes.
Outcomes and definition
The primary outcome was the intubation rate (28 days or in-hospital), and the secondary outcomes included mortality rate (28 days or in-hospital), PaO2/FiO2, respiratory rate, hospital length of stay, intensive care unit (ICU) length of stay, and days free from invasive mechanical ventilation. We also performed two post hoc subgroup analyses comparing COVID-19-related AHRF patients on baseline PaO2/FiO2 < 200 mmHg versus those with >200 mmHg, and those admitted to the ICU versus those admitted to non-ICU sections (ward and emergency department). In addition, we performed subgroup analyses of mortality at 28, 60, and 90 days.
Data extraction and study quality
Two authors (WT and JCW) extracted data independently using a predefined data extraction form, and a third author (YP) resolved disagreements. A case record form designed for the purposes of the study was used to record information on the following variables: enrollment location, follow-up days, age, sex, body mass index, Acute Physiology and Chronic Health Evaluation II score, Sequential Organ Failure Assessment score, baseline PaO2/FiO2, baseline physiological parameters, comorbidities, laboratory parameters, details of intervention, time from symptom onset to enrollment, duration of oxygen therapy, treatment (prone positioning, use of dexamethasone or Il-6 inhibitors), and the following outcomes: the intubation rate, mortality rate, PaO2/FiO2 and respiratory rate at 4–6/24 h after oxygen therapy, hospital length of stay, ICU length of stay, and days free from invasive mechanical ventilation. Data from each study were tabulated and cross checked before inclusion in the analysis.
They independently assessed risk of bias using the Cochrane collaboration risk of bias tool for RCTs, 29 which considers allocation sequence generation, concealment of allocation, masking of participants and investigators, incomplete outcome reporting, selective outcome reporting, and other sources of bias. The Newcastle–Ottawa Scale (NOS) was used to assess the risk of bias in observational studies. 30 In observational studies, scores of 0–4, 5–7, and 8–9 were judged as low, moderate, and high quality, respectively. Full details are provided in the Supplemental Appendix.
Data synthesis and analysis
All analyses were performed in RevMan 5.4.1 (Nordic Cochrane Review Centre, Copenhagen, Denmark) software and STATA 16 (StataCorp, College Station, TX, USA). Categorical outcomes were extracted as the number of patients with each outcome and the total number of patients in each group (denominator). Continuous outcomes were extracted as the sample sizes and means (standard deviations) or medians (interquartile ranges) provided in the studies. When required, medians and interquartile ranges were converted to means and standard deviations for the purpose of the meta-analysis. 31 The DerSimonian and Laird random effects model was used to pool the weighted effect of estimates across all studies. 32 The Mantel–Haenszel method was used to estimate study weights for categorical outcomes and inverse variance for continuous outcomes. For categorical outcomes, we calculated odds ratios (ORs) and 95% confidence intervals (CIs). For continuous outcomes, mean differences (MDs) and 95% CIs were calculated.
Publication bias was assessed using Egger’s test and funnel plots. Statistical heterogeneity assessment between studies was performed using the Mantel–Haenszel model and reported with the I2 and chi-squared (χ2) statistics, 33 in which I2 indicated the degree of heterogeneity (range: 0–100%), as follows: nonsignificant heterogeneity (0–25%), moderate heterogeneity (25–50%), and substantial heterogeneity (>50%). p < 0.05 was considered to indicate a significant difference.
Results
Search results
Following the electronic search, 5765 studies were imported for screening, and 3263 were screened by titles and abstracts after removal of duplicates. Of these, 156 studies underwent full-text assessment, and 20 studies11–27,34–36 were included in our meta-analysis (8 RCTs11,12,18–23 and 12 observational studies13–17,24–27,34–36). The study-selection process is shown in Figure 1.

Study flow diagram.
The basic characteristics of the included studies are summarized in Table 1, and further demographic details of each study are shown in Supplemental Tables S1–5 (Supplemental Appendix, pp. 3–14). The 20 studies included a total of 5732 patients, with population sizes ranging from 23 to 1333; 12 studies11,13–18,20,22–24,26 were conducted in ICUs, 421,25,27,34 in wards or EDs, 212,19 in any department including ICUs and wards, and 2 studies35,36 did not mention enrollment location. Baseline PaO2/FiO2 varied among the included studies, being >200 mmHg in 4 studies19,20,22,25 and <200 mmHg in 11 studies,11–16,21,24,26,27,35; it was not mentioned in 5 studies.17,18,23,34,36
Characteristics of included studies.

COT, conventional oxygen therapy; ED, emergency department; HFNC, high-flow nasal cannula; ICU, intensive care unit; MD, missing data; No, number; RCT, randomized controlled trial; UK, United Kingdom; US, United States.
Literature quality and bias assessment
The risk of bias for the eight RCTs11,12,18–23 are summarized in Supplemental Figure S1 (Supplemental Appendix, p. 18). For all RCTs, most domains were evaluated to have low risk of bias. Due to the impossibility of blinding among patients and medical staff because of the dramatic differences between HFNC and COT, performance bias was high in all studies.
The NOS quality of the 12 observational studies13–17,24–27,34–36 is presented in Supplemental Table S5 (Supplemental Appendix, p. 15). All studies were of medium-level quality (⩾6 stars) or above, and six were considered high quality (⩾8 stars). The Egger’s funnel plots of the intubation, mortality rate, hospital length of stay, ICU length of stay, and days free from invasive mechanical ventilation indicated no obvious publication bias, which was corroborated by the results of the Egger’s test (p = 0.415, 0.188, 0.083, 0.304, and 0.041, respectively) (Supplemental Figures S2–6, Supplemental Appendix, pp. 19–23).
Clinical outcomes
In total, 17 studies (5547 patients)11–27 reported on endotracheal intubation outcomes. HFNC therapy may reduce the need for invasive mechanical ventilation relative to COT (OR = 0.61, 95% CI: 0.46–0.82, p = 0.0009, I2 = 75%, Figure 2). In the subgroup analyses, we also found a lower intubation rate in HFNC group in patients with baseline PaO2/FiO2 < 200 mmHg (p = 0.0007), but not in patients with baseline PaO2/FiO2 > 200 mmHg (p = 0.20); similarly results were found in patients who were in ICU settings at enrollment (p = 0.005), but not in patients in non-ICU settings at enrollment (p = 0.45) (Figure 3).

Intubation for included studies.

Subgroup analysis of intubation.
All 20 studies11–27,34–36 (5732 patients) reported on mortality outcomes. We found no evidence of a difference in mortality when HFNC was compared to COT (OR = 0.84, 95% CI: 0.67–1.06, p = 0.15, I2 = 51%, Figure 4). There was no significant difference in the mortality rate between HFNC and COT when we performed the subgroup analyses based on patients’ baseline PaO2/FiO2, enrollment settings and mortality at 28, 60, and 90 days (Supplemental Figure S7, Supplemental Appendix, pp. 24–26).

Mortality for included studies.
Many studies yielded data on physiological parameters. These studies demonstrated increased mean PaO2/FiO2 levels at 4–6 h (MD = 29.46, 95% CI, 23.31–35.61, p < 0.00001, I2 = 0%; with two included studies12,22) and 24 h (MD = 30.14, 95% CI, 13.12–47.16, p = 0.0005, I2 = 41%; with two included studies15,22), decreased respiratory rate at 4–6 h (M = −1.95, 95% CI, −2.23 to 1.67, p < 0.00001, I2 = 0%, with two included studies12,22 ) in HFNC group compared to COT (Figure 5(a)–(c)).
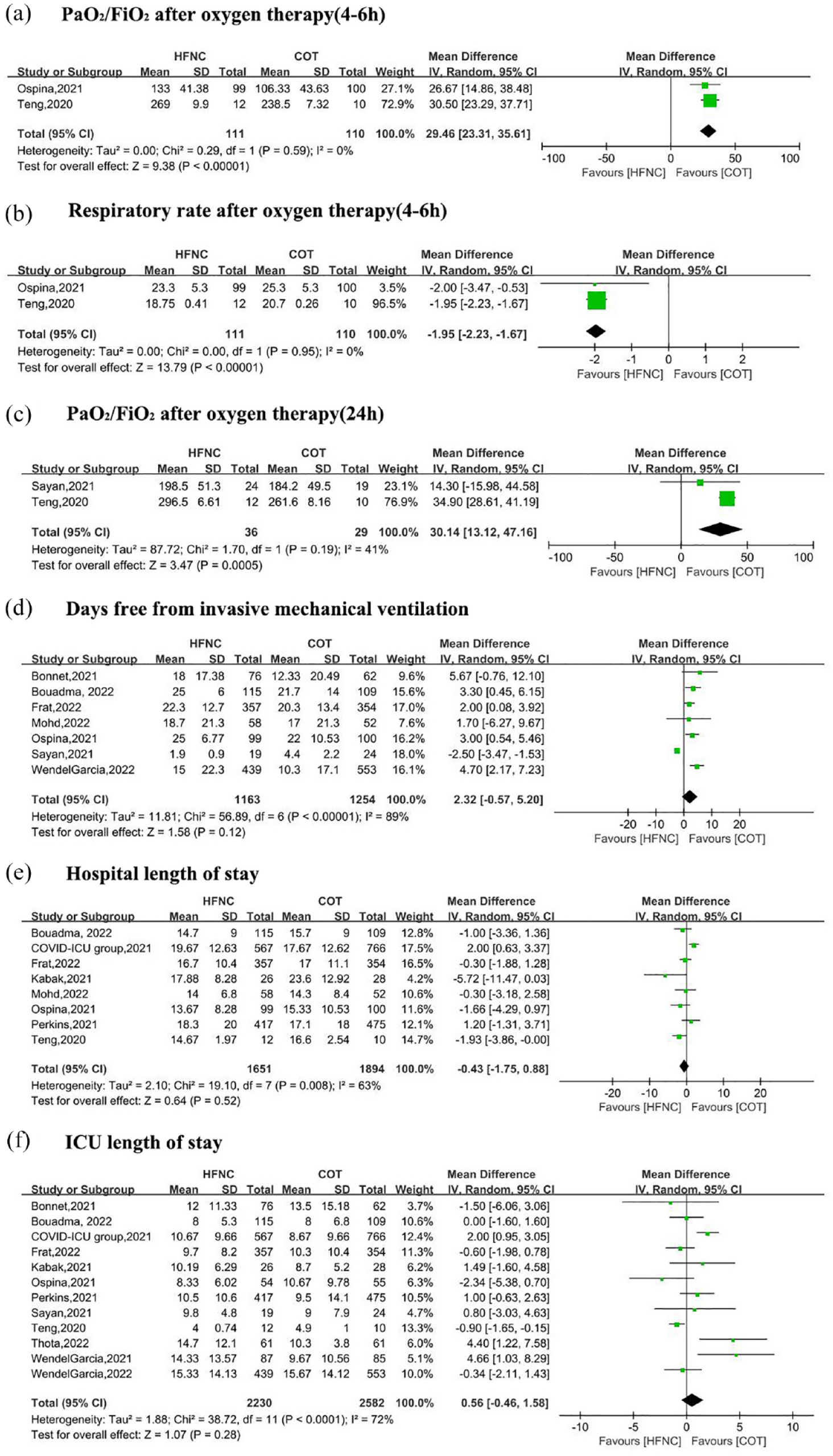
The secondary outcomes for included studies. PaO2/FiO2 after oxygen therapy (4–6 h) (a), respiratory rate after oxygen therapy (4–6 h) (b), PaO2/FiO2 after oxygen therapy (24 h) (c), days free from invasive mechanical ventilation (d), hospital length of stay (e), and ICU length of stay (f).
There were no differences between the HFNC and COT groups in days free from invasive mechanical ventilation (MD = 2.32, 95% CI, −0.57 to 5.20, p = 0.12, I2 = 89%, with seven included studies11–13,15,17,18,27), the hospital length of stay (MD = −0.43, 95% CI, −1.75 to 0.88, p = 0.52, I2 = 63%, with eight included studies11,12,14,18,21,22,26,27), and ICU length of stay (MD = 0.56, 95% CI, −0.46 to 1.58, p = 0.28, I2 = 72%; with 12 included studies11–18,21–23,26) (Figure 5(d)–(f)).
Adverse events were variably reported across five studies11,12,18,21,23 (Supplemental Table S6, Supplemental Appendix, pp. 16–17), which precluded our ability to conduct pooled analysis.
Discussion
In this systematic review and meta-analysis, we found that HFNC was associated with a lower intubation rate than the COT in patients who were hospitalized for COVID-19, in particular among patients whose baseline PaO2/FiO2 < 200 mmHg and those who were in an ICU setting at enrollment. It also showed an improvement in oxygenation at 4–6 and 24 h, and in respiratory rate at 4–6 h in the HFNC group compared to COT. There were no significant differences in mortality rate, days free from invasive mechanical ventilation, hospital length of stay, or ICU length of stay between the HFNC and COT groups.
As with several meta-analyses in non-COVID-19 patients with AHRF,37,38 we found that use of HFNC was associated with a reduction in intubation rate relative to COT in COVID-19 patients with AHRF. This aligns with a previous study that enrolled 782 patients with COVID-19-related AHRF with baseline PaO2/FiO2 < 200 mmHg, and all of these patients were in an ICU setting at enrollment. 11 A post hoc subgroup analysis of non-COVID-9 patients with AHRF also found that the intubation rate was lower in patients with a PaO2/FiO2 < 200 mmHg treated with HFNC relative to those treated with NIV or COT. 39 For these reasons, we performed a subgroup analysis of patients with COVID-19 with baseline PaO2/FiO2 < 200 mmHg and treatment in an ICU and found that use of HFNC significantly decreased the need for mechanical ventilation support compared to COT. The certainty of evidence for these outcomes was moderate or high, however, due to the small number of RCTs that have reported separate outcome data from these subgroups, more RCTs may needed in the future.
The findings of the subgroup analysis might have several explanations. First, patients with baseline PaO2/FiO2 < 200 mmHg are more likely to progress to invasive mechanical ventilation. Taken together, lower PaO2/FiO2 is associated with extensive areas of low ventilation-perfusion matching for COVID-19. 40 The use of HFNC in these patients may be associated with an increase in end-expiratory lung volume and alveolar recruitment and a more homogeneous distribution of lung aeration relative to COT, which leads to better ventilation-perfusion matching and better oxygenation. 41 Therefore, we found that HFNC improves oxygenation and respiratory rate and further may reduce the intubation rate relative to COT. Second, experimental data suggest that patients with PaO2/FiO2 < 200 mmHg may represent the most at risk population of patient self-inflicted lung injury (P-SILI). 42 High flows of HFNC can more adequately match patients’ respiratory flow demands, thereby decreasing the risk for P-SILI,43,44 which may have important implications for the management of the heterogeneous pulmonary manifestations of patients with COVID-19. 45 This effect can be obtained by starting with a minimum gas flow of 30 L/min and increasing with an increase in HFNC flow. 46 However, subgroup analysis based on different HFNC settings requires further analysis. It is worth noting that too much delay for invasive mechanical ventilation may induce P-SILI as well. The HFNC treatment failure rate was highest among patients with low PaO2/FiO2 ratios and the evolution of the respitatory oxygenation index (ROX index), we should determine the optimal timing of intubation for those in whom HFNC support fails.
The provision of an ICU setting and lower PaO2/FiO2 are directly correlated, and the delivery of high flow allows matching patients’ inspiratory peak flow, even in patients generating high inspiratory peak flow, avoiding dilution with room air and thus providing higher FiO2. 41 Patients who require ICU admission are also sicker, the increased inspiratory effort and vigorous inspiratory effort can contribute to lung injury. As we discussed above, high flows of HFNC can more adequately match patients’ respiratory flow demands, thereby reducing the work of breathing and mitigating the inspiratory effort, as well as decreasing the risk for lung injury.43,44 Furthermore, ICU patients also experience more respiratory distress, the heat, and humidification delivered by HFNC help to maintain hydration and mobilize secretions, which positively affect the mucus hypersecretion of patients. 41 By contrast, no significant differences in intubation were seen between HFNC and COT groups among patients with baseline PaO2/FiO2 > 200 mmHg or non-ICU admission. The application of HFNC and COT according to varying oxygenations and locations could prove helpful in resource-constrained settings during a pandemic. It is worth noting that, those DNI/do-not-bring to the ICU order patients may also quit sick and have a relatively low PaO2/FiO2 ratio. However, we cannot extract the data of those DNI for analysis. HFNC maybe useful for them and further studies/analysis are needed to verify it.
As in several previous meta-analyses,47,48 no significant difference in mortality between the HFNC and COT groups was found, although there was moderate statistical heterogeneity in the mortality outcome data. Similar results were obtained for mortality in the subgroup analyses of COVID-19 patients with different PaO2/FiO2 (i.e. <200 mmHg versus >200 mmHg), treatment in different locations (i.e. ICU versus non-ICU), and different follow-up times (28, 60, and 90 days). There were no differences in days free from invasive mechanical ventilation, hospital length of stay, and ICU length of stay.
It was not possible to conduct a meta-analysis of adverse events because they were variably reported across studies. However, patients receiving HFNC did not seem to have increased risk for adverse events compared to those receiving COT. HFNC and COT are both less invasive than invasive mechanical ventilation, and the adverse events associated with HFNC and COT are always self-limiting.
There were several limitations to this study. First, the results were based on both RCT and non-RCT studies. For all RCTs, most domains were evaluated to have low risk of bias, but performance bias was high due to the impossibility of blinding among patients and medical staff; all non-RCT studies were of medium-level quality or above, and the certainty of evidence for most outcomes was moderate or high, which may have led to an underestimation of the heterogeneity and reduced the precision of our pooled effect estimate. Thus, large-sample RCTs are necessary to confirm our findings. Second, there were crossovers between groups in some studies, whereas crossovers were not allowed in others. Third, the DNI policy and other treatments (Supplemental Table S4, Supplemental Appendix, pp. 13–14) such as differences in amount of prone positioning, use of dexamethasone or IL-6 inhibitors in both groups also vary, which further increases heterogeneity. In addition, only a few studies have reported accurate settings of HFNC, and this information might not have been recorded very precisely, as it was observed and recorded unsystematically. Furthermore, the comparison might be biased because COT is defined quite broadly, comparing with 4 L nasal canula is different than comparing with NRM. Therefore, we were not able to assess the different daily treatment durations and flow settings of HFNC for patient outcomes.
Conclusion
In conclusion, this systematic review and meta-analysis found that in patients who were hospitalized for COVID-19, HFNC was associated with a relatively lower intubation rate than the COT group, and may be more significant among patients whose baseline PaO2/FiO2 < 200 mmHg and those who were in an ICU setting at enrollment. The evidence also shows improvement in the oxygenation and respiratory rate in the HFNC group relative to COT. However, our meta analyses do not demonstrate a benefit in the mortality rate, days free from invasive mechanical ventilation, hospital length of stay, or ICU length of stay in the HFNC group.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231225323 – Supplemental material for Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tar-10.1177_17534666231225323 for Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: a systematic review and meta-analysis by Jian-chao Wang, Yun Peng, Bing Dai, Hai-jia Hou, Hong-wen Zhao, Wei Wang and Wei Tan in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666231225323 – Supplemental material for Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: a systematic review and meta-analysis
Supplemental material, sj-docx-2-tar-10.1177_17534666231225323 for Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: a systematic review and meta-analysis by Jian-chao Wang, Yun Peng, Bing Dai, Hai-jia Hou, Hong-wen Zhao, Wei Wang and Wei Tan in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.