
Abstract
Background:
Studies of mechanically ventilated patients with a low risk of reintubation have suggested that the use of high-flow nasal cannula (HFNC) oxygen therapy reduces the risk of reintubation compared with conventional oxygen therapy (COT). However, the effect of HFNC following extubation in elderly patients with a high risk of reintubation remains unclear.
Methods:
All consecutive medical intensive care unit (ICU) patients aged >65 years who were mechanically ventilated for >24 h were prospectively registered between July 2017 and June 2018. Control was obtained from a historical database of patients attending the same ICU from January 2012 to December 2013. A total of 152 patients who underwent HFNC after planned extubation according to institutional protocols (HFNC group) were compared with a propensity-matched historical control group who underwent COT (n = 175, COT group). The primary outcome was the proportion of reintubated patients within 48 h after planned extubation.
Results:
One hundred patients from the HFNC group and 129 patients from the COT group were matched by a propensity score that reflected the probability of receiving HFNC, and all variables were well matched. Post-extubation respiratory failure (41.0% versus 33.3%, p = 0.291) and reintubation rate within 48 h (16.0% versus 11.6%, p = 0.436) did not differ between the HFNC and COT groups. However, decreased levels of consciousness as a sign of post-extubation respiratory failure (27.0% versus 11.7%, p = 0.007) were significantly increased in the HFNC group compared with the COT group.
Conclusion:
Among elderly patients who underwent planned extubation, HFNC was not associated with a decrease in the risk of reintubation. Further prospective study evaluating the clinical benefits of post-extubation HFNC in elderly patients is needed.
The reviews of this paper are available via the supplemental material section.
Keywords
Background
Despite advances in critical care, post-extubation respiratory failure following planned extubation has remained relatively unchanged over the last decade. 1 In addition, reintubation secondary to post-extubation respiratory failure is associated with several adverse outcomes, including increased nosocomial infections, length of hospitalization, and mortality.1–3 Therefore, following extubation, oxygen supplementation via a facial mask with inspiratory oxygen fraction (FiO2) targeted to physiological parameters is widely used during the post-extubation period to correct residual impairment in oxygenation.
Recent technological improvements have enabled the delivery of high-flow oxygen therapy via a nasal cannula (high-flow nasal cannula; HFNC); this oxygen therapy delivers a low level of continuous positive airway pressure with increased end-expiratory pressure and decreased work of breathing.4,5 Moreover, recent randomized clinical trials have demonstrated that HFNC reduced reintubation compared with conventional oxygen therapy (COT) in patients with low risk of reintubation and was not inferior to non-invasive mechanical ventilation (MV) in patients with high risk.6,7 Therefore, HFNC is emerging as an important modality in post-extubation patients.6,7
The number of elderly patients admitted to intensive care units (ICUs) is increasing.8,9 Elderly patients are typically highly vulnerable and acute exacerbations of chronic conditions result in increased disability or mortality. 10 In addition, weaning these patients from MV is challenging, and the reintubation rate following extubation is higher than that in younger patients. 11 Therefore, preventing reintubation following planned extubation is critical to reduce mortality and length of hospitalization. However, the effect of HFNC following extubation in elderly patients with a high risk of reintubation remains unclear.
Therefore, in the present study, we investigated the effects of post-extubation HFNC on reintubation in elderly patients compared with COT using a propensity score matching method.
Methods
Study design and population
All consecutive patients admitted to the medical ICU and requiring MV for more than 24 h between July 2017 and June 2018 were prospectively registered at Samsung Medical Center, a 1989-bed university-affiliated tertiary referral hospital in Seoul, South Korea. Patients aged older than 65 years who underwent a spontaneous breathing trial (SBT) for weaning from MV and planned extubation according to the standardized protocol were enrolled in the present study (Figure 1). A list of potential control individuals aged older than 65 years was obtained from a historical database of patients attending the same ICU from January 2012 to December 2013, which was included as described in our previous studies.12,13
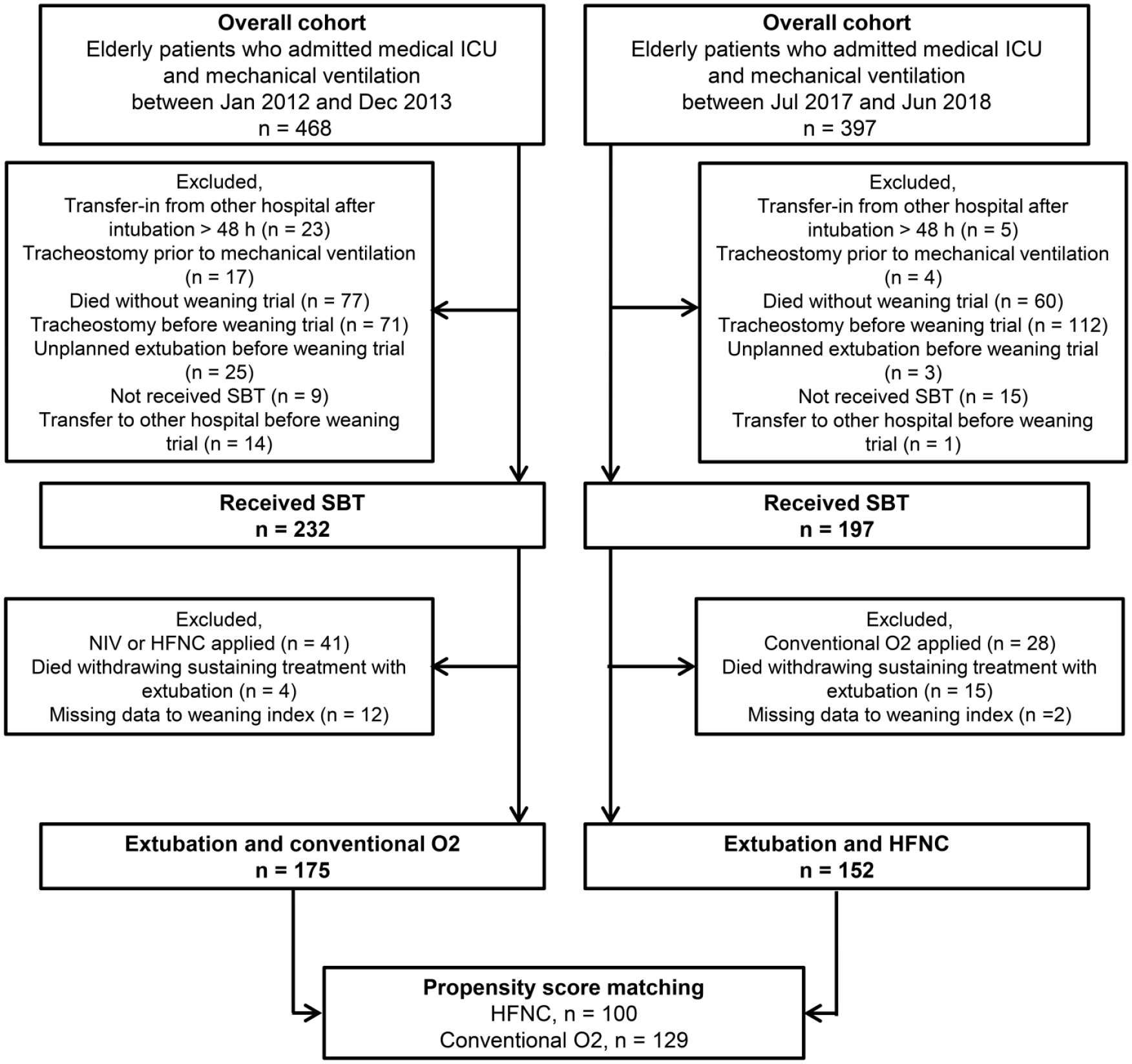
Flow chart of patient selection from the overall cohort for analysis.
The Institutional Review Board of Samsung Medical Center gave approval for the study to review and publish information from the patients’ records. Informed consent was waived because of the observational nature of the study. All patient records and data were anonymized and de-identified prior to analysis.
Standardized weaning process and oxygen therapy after extubation
Since 2010, the medical ICU of our hospital has utilized a specific protocol-based weaning program according to the recommendations by Boles et al. 14 Details of our weaning program were described in previous reports.12,13,15 In short, respiratory care practitioners, who are registered nurses specializing in respiratory care, screened patients daily for weaning readiness and conducted a 30-min T-piece SBT according to the protocol. If a patient failed the SBT, MV was resumed, and the team reviewed possible reversible etiologies for the failure. Again, when a patient proved ready for weaning, the SBT was repeated the following day. Patients who received more than one SBT or prolonged weaning underwent a 120-min T-piece SBT. When a patient passed the SBT, extubation was performed. Followed extubation, oxygen therapy was continuously administered via a non-rebreathing facemask at 9–10 L/min, with an FiO2 of 40%. Since July 2017, we have modified the protocol of oxygen therapy following planned extubation using HFNC (Optiflow, Fisher and Paykel Healthcare) routinely based on the results of recent trials.6,7 The flow was initially set at 30 L/min with an FiO2 of 40% and was adjusted according to patient oxygenation requirements. After 24 h, the flow was titrated downward to 25 L/min and changed to a conventional nasal cannula, if tolerable to the patient. The routine prophylactic steroid was not taken for prevention of post-extubation laryngeal edema.
Data collection
The following data were extracted from the medical records: general demographic information, underlying disease, reasons for ICU admission and intubation, and laboratory and clinical data on extubation day. Additionally, we collected SBT data, including data for the rapid shallow breathing index, negative inspiratory pressure, confusion assessment method for the ICU (CAM-ICU), Richmond Agitation–Sedation scale (RASS), PaO2/FiO2 ratio, and vital signs. The primary outcome was reintubation within 48 h following planned extubation. In addition, we documented secondary outcomes including post-extubation respiratory failure within 48 h, death or reintubation within 7 days, reintubation during hospital stay, cause of reintubation, tracheostomy rate, length of ICU stay and length of hospitalization, ICU and hospital mortalities, and hospital discharge type. Post-extubation respiratory failure was defined as the persistent presence of any of the following criteria: respiratory acidosis (pH <7.35 with PaCO2 >45 mmHg), SpO2 less than 90% or PaO2 of less than 60 mmHg at an FiO2 higher than 40%, respiratory rate of more than 35/min, decreased level of consciousness [Glasgow coma scale (GCS) >1 point decrease] or agitation, clinical signs suggestive of respiratory muscle fatigue, or increased work of breathing. 16
Statistical analysis
To compare the HFNC and COT groups, a pairwise matching method was used to reduce the effects of selection bias and possible confounding factors between the two groups. A propensity score was derived from a non-parsimonious logistic regression model that included interval between hospital admission to intubation, duration of MV support, clinical features [sequential organ failure assessment (SOFA) score, RASS, fluid balance, and suction frequency] at extubation day and clinical measurement (pH, PaCO2, PaO2/FiO2 ratio, and mean arterial pressure) before extubation. Each patient was assigned a propensity score that reflected the probability of receiving HFNC and variable ratio-matching was performed for a larger number of COT group than HFNC group in order to reduce sample loss and improve study power. Subjects from the two groups were matched by variable ratio-matching with their propensity score in blocks from 1:1 to 1:4 pairs. The quality of matching was assessed by calculating the standardized mean difference (SMD) between selected variables, with an SMD of <0.10 reflecting good matching.17–19 The matching ratio of 1:2 was selected for the final analysis. All data were presented as median values and interquartile range for continuous variables and as numbers and percentages for categorical variables. Continuous variables were analyzed using the Mann–Whitney–Wilcoxon U test, and categorical variables were analyzed using the Pearson χ2 test or Fisher exact test. Time to reintubation and time to death were assessed using the Kaplan–Meier analysis. All analyses were performed using R Statistical Software (Version 3.2.5; R Foundation for Statistical Computing, Vienna, Austria). p values are two-tailed and values of <0.05 were considered statistically significant.
Results
Study population
Overall, 327 patients—152 in the HFNC group from July 2017 to June 2018 and 175 in the COT group from January 2012 to December 2013—who underwent planned extubation via the standardized weaning process and received HFNC or COT in the medical ICU were included (Figure 1). The median age was 73 years, and 67.3% of the patients were male. The most common comorbidity was hypertension (52.0%) followed by malignant disease (48.0%). The most common reason for ICU admission was respiratory disease (53.2%), followed by cardiovascular disease (8.9%).
The baseline characteristics of both groups are presented in Table 1. Patients who received HFNC exhibited a higher initial SOFA score, were less likely to have diabetes, and had fewer interval days between hospital admission and intubation. Clinical characteristics on the day of extubation are presented in Table 2. Clinical features, including the SOFA score, fluid balance, number of suctions per day, PaO2 at pre- and post-extubation, CAM-ICU, and RASS, were better in the HFNC group compared with the COT group.
Clinical characteristics of the study population at the time of ICU admission.

Data are presented as number (percentage) or median (interquartile range).
AE, acute exacerbation; ARDS, acute respiratory distress syndrome; BMI, body mass index; COPD, chronic obstructive pulmonary disease; COT, conventional oxygen therapy; CPR, cardiopulmonary resuscitation; CVD, cerebral vascular disease; HFNC, high-flow nasal cannula; ICU, intensive care unit; ILD, interstitial lung disease; SOFA, sequential organ failure assessment.
Clinical characteristics of the study population on the day of planned extubation.

Data are presented as number (percentage) or median (interquartile range).
BGA, blood gas analysis; CAM-ICU, confusion assessment method for the intensive care unit; COT, conventional oxygen therapy; FiO2, inspiratory oxygen fraction; GCS, Glasgow Coma Scale; HFNC, high-flow nasal cannula; MV, mechanical ventilation; NIP, negative inspiratory pressure; RASS, Richmond Agitation–Sedation Scale; RSBI, rapid shallow breathing index; SBT, spontaneous breathing trial; SOFA, sequential organ failure assessment.
The propensity score analysis matched 100 patients from the HFNC group to 129 patients from the COT group. After propensity score matching, the baseline characteristics were well balanced between the two groups, with the SMD being <0.10. In the matched HFNC group, patients were more likely to have increased PaO2 at pre-extubation (100 mmHg versus 92 mmHg, p = 0.045) and decreased hemoglobin (9.6 g/dL versus 10.1 g/dL, p = 0.001) compared with the matched COT group on extubation day.
Clinical outcomes
Clinical outcomes of the matched patients are shown in Table 3. The reintubation rate within 48 h was 16.0% and 11.0%, respectively, in the HFNC and COT groups (p = 0.436). In addition, the death or reintubation within 7 days following the extubation was 27.0% and 21.7%, respectively, in these groups (p = 0.439). Post-extubation respiratory failure within 48 h did not significantly differ between the two groups (41.0% versus 33.3% in the HFNC versus COT groups, p = 0.291); however, the decrease in levels of consciousness, one of the signs of post-extubation respiratory failure, was higher in the matched HFNC group than that in the matched COT group (27.0% versus 11.7%, p = 0.007). Figure 2 shows the Kaplan–Meier curve for reintubation within 48 h. The cumulative reintubation rate was not different between the two matched groups (p = 0.316, log-rank test). The reason for reintubation differed between the two groups (p = 0.046). Unbearable dyspnea, one of the reasons for reintubation, was significantly increased in the HFNC group. Of all matched patients, unbearable dyspnea was the most common cause of reintubation, followed by persistent hypoxemia.
Clinical outcomes of the matched high-flow nasal cannula group and conventional oxygen therapy group.

Data are presented as number (percentage) or median (interquartile range).
Heart rate less than 50/min with loss of alertness or severe hemodynamic instability (systolic blood pressure <90 mmHg for >30 min).
One or more signs may be listed. Respiratory acidosis: pH <7.35 with PaCO2 >45 mmHg; hypoxia: SPO2 <90 or PaO2 <60 mmHg at FiO2 >40; decreased level of consciousness: Glasgow Coma Scale >1-point decrease; increased respiratory rate: respiratory rate >35/min.
COT, conventional oxygen therapy; FiO2, inspiratory oxygen fraction; HFNC, high-flow nasal cannula; ICU, intensive care unit.
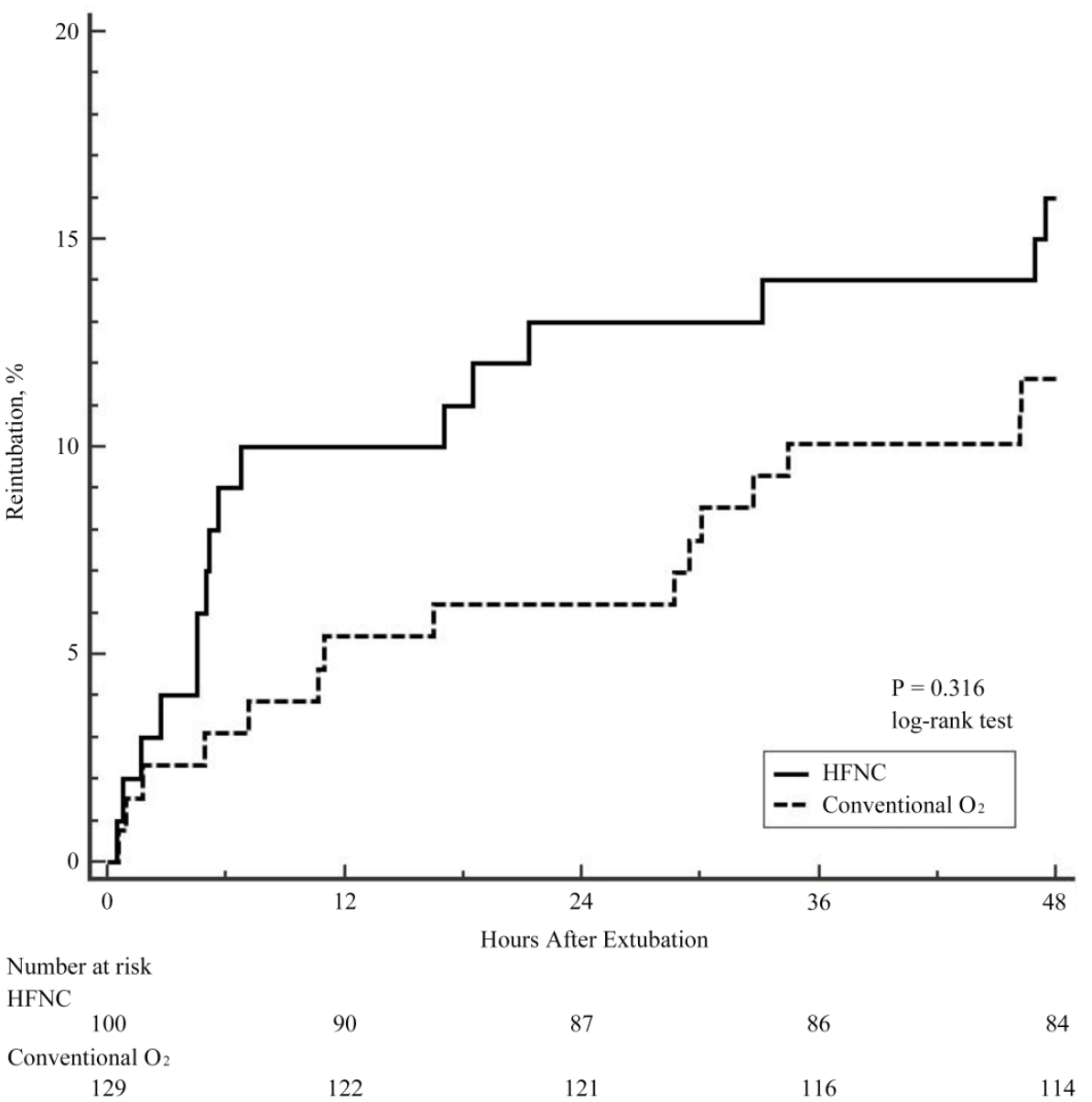
Kaplan–Meier analysis of time from extubation to reintubation. The cumulative reintubation rate was not different between the two matched groups (p = 0.316, log-rank test).
There was no significant difference in the ICU mortality between the two groups (8.1% versus 4.5%, p = 0.288). In addition, the hospital mortality did not significantly differ between the two groups (19.8% versus 19.8%, p = 1.000). The cumulative mortality following post-extubation was not different between the two matched groups (p = 0.120, log-rank test) (Figure 3). The discharge type was not different between the two groups (p = 0.633). In all matched patients, home was the most common discharge destination, followed by other general hospitals. Also, tracheostomy rate (12.0% versus 20.9%, p = 0.108), length of ICU stay (6 days versus 6 days, p = 0.647), and length of hospitalization (18 days versus 23 days, p = 0.055) were not different between the two groups.

Kaplan–Meier analysis of time from extubation to death. The cumulative mortality following post-extubation was not different between the two matched groups (p = 0.120, log-rank test).
Discussion
The present study investigated the effects of post-extubation HFNC in comparison with COT on reintubation within 48 h following planned extubation and assessed the clinical outcomes in the elderly patients admitted to the medical ICU using a protocol-based weaning program. The HFNC was not associated with prevention of reintubation and reduction in mortality outcomes. In addition, HFNC did not reduce post-extubation respiratory failure within 48 h after planned extubation.
Some controversy exists concerning the effectiveness of HFNC in post-extubation patients. Several studies have shown the positive effects of post-extubation HFNC compared with post-extubation COT.6,20,21 However, these studies were conducted only in low-risk or postsurgical patients, and there is no conclusion regarding high-risk patients. Corley et al. reported that HFNC did not improve oxygenation, atelectasis, respiratory rate, or dyspnea, and it did not reduce rates of allocated therapy failure among patients with a body mass index ⩾30 kg/m2 who have recently undergone extubation. 22 In addition, Zhang et al. evaluated post-extubation HFNC patients using electrical impedance tomography and found that their response to HFNC was variable, with varying degrees of recruitment and overdistension. 23 These results indicate that HFNC might be of benefit to selected patients rather than to all patients with safety concerns.
Age is a non-modifiable but important factor with regard to reintubation following extubation. 24 Considering geriatric frailty, HFNC might be effective in elderly patients owing to several benefits associated with it. HFNC facilitates the maintenance of a constant FiO2 during peak inspiratory flow and confers benefits, such as a low level of continuous positive airway pressure with increased end-expiratory volume and reduced work of breathing, partly via intrinsic positive end-expiration pressure compensation and dead space washout.4,25–27 Moreover, the inspired gases are warmed and humidified, thereby improving comfort and improving respiratory secretion drainage. 20 Previous randomized clinical trials have demonstrated that the use of HFNC compared with COT in patients with low risk of reintubation reduced this risk.6,28 However, in the present study, HFNC post-extubation did not reduce the reintubation rate compared with COT in elderly patients who were at a high risk of reintubation.
An important concern of HFNC is that it delays reintubation, resulting in worse clinical outcomes. 29 However, in the present study, the Kaplan–Meier analysis revealed that the reintubation rate was higher in the matched HFNC group within 12 h compared with the matched COT group. In addition, hospital mortality did not differ between the two groups. Therefore, post-extubation HFNC was not associated with delayed intubation and worse clinical outcomes in this study. This finding could be attributed to the predefined criteria for extubation failure under the protocol-based weaning program, which prevents potentially precarious delays in intubation.
Interestingly, decreased level of consciousness as a sign of post-extubation respiratory failure within 48 h was higher in the matched HFNC group than that in the matched COT group, although other potential confounding variables for level of consciousness, such as RASS, GCS, and presence of delirium at the time of SBT, were not different between the two groups. It is difficult to explain this result, but it might be related to unmeasured bias for level of consciousness rather than adverse event associated with HFNC. In addition, this finding could have been generated by misclassification bias since the CAM-ICU has relatively low sensitivity to find a change of mental status (delirium) in routine practice. 30
To the best of our knowledge, this is the first comparative study evaluating the clinical benefits of post-extubation HFNC in elderly patients with a control group. However, there are several potential limitations to our study that should be acknowledged. First, considering the observational nature of the study, a possibility of selection bias influencing the significance of our findings exists. However, the propensity score analysis was used to reduce selection bias. Further, data were prospectively collected from consecutive patients admitted to the medical ICU receiving MV support for more than 24 h. The patients were screened daily for weaning readiness according to a protocol-based weaning program. Therefore, our cohort is more likely to reflect the patients encountered in routine ICU practice and thus can be readily applicable in similar settings. However, the present study was conducted at a single institution with a protocol-based weaning program. Accordingly, our findings may have limited generalizability. Second, for the convenience of research, the historical control was the already available data from the previous published study collected between July 2010 and September 2013. Although the patients were managed according to a protocol-based weaning program, the advances in medical care for the different time period may influence the clinical outcome. Finally, although the data were prospectively collected from all patients consecutively admitted to the medical ICU with MV support for more than 24 h, no detailed information on deviation of the weaning protocol was collected.
In summary, post-extubation HFNC was not associated with a decrease in the risk of reintubation in elderly patients who underwent planned extubation under a protocol-based weaning program. However, current evidence does not permit firm conclusions regarding the role of post-extubation HFNC in elderly patients and further prospective study evaluating the clinical benefits of post-extubation HFNC in carefully selected elderly patients with a high risk of reintubation is needed.
Supplemental Material
Author_Response_1 – Supplemental material for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study
Supplemental material, Author_Response_1 for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study by Ryoung-Eun Ko, Chul Park, Jimyoung Nam, Myeong Gyun Ko, Soo Jin Na, Joong Hyun Ahn, Keumhee C. Carriere and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_Response_2 – Supplemental material for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study
Supplemental material, Author_Response_2 for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study by Ryoung-Eun Ko, Chul Park, Jimyoung Nam, Myeong Gyun Ko, Soo Jin Na, Joong Hyun Ahn, Keumhee C. Carriere and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study
Supplemental material, Reviewer_1_v.1 for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study by Ryoung-Eun Ko, Chul Park, Jimyoung Nam, Myeong Gyun Ko, Soo Jin Na, Joong Hyun Ahn, Keumhee C. Carriere and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study
Supplemental material, Reviewer_1_v.2 for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study by Ryoung-Eun Ko, Chul Park, Jimyoung Nam, Myeong Gyun Ko, Soo Jin Na, Joong Hyun Ahn, Keumhee C. Carriere and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study
Supplemental material, Reviewer_2_v.1 for Effect of post-extubation high-flow nasal cannula on reintubation in elderly patients: a retrospective propensity score-matched cohort study by Ryoung-Eun Ko, Chul Park, Jimyoung Nam, Myeong Gyun Ko, Soo Jin Na, Joong Hyun Ahn, Keumhee C. Carriere and Kyeongman Jeon in Therapeutic Advances in Respiratory Disease
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Samsung Medical Center grant (SMO1180151). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.