
Abstract
Riociguat is one of several approved therapies available for patients with pulmonary arterial hypertension (PAH). Treatment should be initiated and monitored at an expert center by a physician experienced in treating PAH, and the dose adjusted in the absence of signs and symptoms of hypotension. In certain populations, including patients with hepatic or renal impairment, the elderly, and smokers, riociguat exposure may differ, and dose adjustments should therefore be made with caution according to the established scheme. Common adverse events are often easily managed, particularly if they are discussed before starting therapy. Combination therapy with riociguat and other PAH-targeted agents is feasible and generally well tolerated, although the coadministration of phosphodiesterase type 5 inhibitors (PDE5i) and riociguat is contraindicated. An open-label, randomized study is currently ongoing to assess whether patients who do not achieve treatment goals while receiving PDE5i may benefit from switching to riociguat. In this review, we provide a clinical view on the practical management of patients with PAH receiving riociguat, with a focus on the opinions and personal experience of the authors.
The reviews of this paper are available via the supplemental material section.
Introduction
Pulmonary arterial hypertension and its management
Pulmonary arterial hypertension (PAH) is a life-threatening disease, characterized by progressive remodeling, narrowing, and obliteration of small pulmonary arteries due to proliferation of smooth muscle and endothelial cells, vascular wall inflammation, and fibrosis.1–4 PAH is rare, with the lowest estimates of incidence and prevalence in 2015 being 2.4 and 15 cases per million adult population, respectively. 5 For those with PAH, however, the disease is debilitating and patients are often affected by symptoms of dyspnea, fatigue, syncope and chest pain, and many progress to right ventricular failure and premature death.6,7
If PAH is suspected, patients should be referred to an expert pulmonary hypertension (PH) center for diagnosis and treatment by an experienced physician. 5 PAH diagnosis is confirmed by right heart catheterization (RHC), and hemodynamically defined by a mean pulmonary artery pressure (mPAP) of ⩾25 mmHg, normal pulmonary artery wedge pressure (⩽15 mmHg), and a pulmonary vascular resistance (PVR) of >3 Wood units (a new definition of mPAP ⩾20 mmHg and PVR ⩾3 Wood units for all forms of precapillary PH was proposed recently).5,8 After confirmation of PAH diagnosis, a number of targeted medical therapies are available for treatment.5,9 These therapies are based on four molecular targets (prostacyclin receptors, endothelin receptors, phosphodiesterase type 5 (PDE5), and soluble guanylate cyclase [sGC]). Prostacyclin analogs (PCAs) and the prostacyclin receptor agonist selexipag target the prostacyclin pathway, and endothelin receptor antagonists (ERAs) target the endothelin pathway, while PDE5 inhibitors (PDE5i) target PDE5 degradation of cyclic guanosine monophosphate (cGMP) in the nitric oxide (NO) pathway. The sGC stimulator riociguat has been shown to have a dual mode of action resulting in increased cGMP levels within the NO pathway: it directly stimulates sGC via an NO-independent binding site, and stabilizes NO binding with sGC (Figure 1).9–14

Mechanism of action of riociguat. 15 (a) Riociguat directly stimulates sGC in an NO-independent manner. (b) Riociguat sensitizes sGC to endogenous NO by stabilizing binding of the molecules.
It is common practice for patients with PAH to be treated with a combination of these therapies, through either initial or sequential addition, 9 although it is important to note that riociguat and PDE5i in combination is contraindicated. Currently, for patients with PAH who are World Health Organization functional class (WHO FC) II/III, a proactive approach with initial oral combination therapy is recommended. Regardless of the chosen treatment regimen or initial treatment response, patients should undergo regular comprehensive risk assessment, allowing patient stratification into low (<5%), intermediate (5–10%), or high (>10%) risk categories that estimate 1-year mortality.5,16
Since the availability of riociguat, clinicians have the option to incorporate it as part of existing treatment regimens for treatment-naive and pretreated patients who are not at therapeutic goal. This article aims to provide a clinical view on the practical management of riociguat in patients with PAH and will also provide insight from the authors’ personal experience. The reviews of this paper are available via the supplemental material section.
Riociguat phase III clinical trial data
The efficacy and safety of riociguat in patients with PAH were demonstrated in the pivotal PATENT-1 study, leading to the approval of riociguat for the treatment of PAH in many countries. 17 Riociguat is also approved for inoperable or persistent/recurrent chronic thromboembolic pulmonary hypertension (CTEPH) based on a second phase III study, CHEST-1.5,18,19
PATENT-1 was a 12-week, double-blind, placebo-controlled phase III study in which riociguat significantly improved 6-min walking distance (6MWD), as well as secondary outcomes including WHO FC, N-terminal prohormone of brain natriuretic peptide (NT-proBNP), hemodynamic parameters, time to clinical worsening, and quality of life (QoL) according to the Living with Pulmonary Hypertension score. 17 PATENT-2 was the long-term, open-label extension of PATENT-1, which reported consistent improvements in 6MWD, WHO FC, and NT-proBNP at 2 years. Estimated survival and clinical worsening-free survival rates were 93% and 73%, respectively, and a significant association was found between 6MWD, NT-proBNP, and WHO FC and overall survival at baseline and follow-up.20,21 In addition, riociguat improved outcomes according to EuroQoL 5D at 2 years in PATENT-2. 22
Several post hoc and subgroup analyses have been undertaken in the PATENT database, assessing use of different endpoints (clinically relevant criteria or satisfactory clinical response)23,24 and risk assessment tools (allows patient risk stratification according to estimated 1-year mortality).25–27 In a retrospective assessment of the PATENT-1 population, it was found that, compared with placebo, riociguat increased the proportion of patients achieving prespecified endpoints at Week 12,23,24 or a lower-risk status (Figure 2)25–27 (Table 1).

Proportion of patients worsening, stabilizing, or improving REVEAL risk score at PATENT-1 Week 12. 26
Effect of riociguat on patients achieving prespecified endpoint and risk status.

Defined as ⩾10% improvement in 6MWD, WHO FC I/II, and no clinical worsening.
Pooled riociguat group (1.5 mg tid and 2.5 mg tid)
Defined as 6MWD ⩾380 m, WHO FC I/II, cardiac index ⩾2.5 l/min/m2, NT-proBNP <1800 pg/ml, SvO2 ⩾65%
Defined as the number of low-risk criteria fulfilled: 6MWD >440 m, WHO FC I/II, RAP <8 mmHg, cardiac index ⩾2.5 l/min/m2
Defined as the number of low-risk criteria fulfilled: 6WMD >440 m, WHO FC I/II, NT-proBNP <300 pg/ml
Defined as the mean of grades (1–3: low, intermediate, high) of six available criteria (6MWD, WHO FC, NT-proBNP, RAP, cardiac index, and SvO2) as defined in the European Society of Cardiology/European Respiratory Society 2015 treatment guidelines, rounded to the nearest integer
Data for two parameters typically included in the RRS calculation, pericardial effusion, and diffusing capacity of the lung for carbon monoxide were not available for the PATENT-1 cohort
Patients listed as pretreated were already receiving another PAH-targeted therapy at the beginning of PATENT-1.
6MWD, 6-min walking distance; NT-proBNP: N-terminal prohormone of brain natriuretic peptide; PAH, pulmonary arterial hypertension; RAP, right atrial pressure; RRS, REVEAL risk score; SvO2, mixed venous oxygen saturation; tid, three times daily; WHO FC, World Health Organization functional class.
Practical management of riociguat in PAH
As with all PH-targeted treatment, riociguat treatment for PAH should be initiated and monitored at an expert center by a physician experienced in treatment of the condition.5,28 This is because many of the techniques used in the diagnosis and monitoring of PAH, such as RHC and cardiopulmonary exercise testing, are technically demanding and require a considerable level of expertise in their application and interpretation. In a retrospective study of claims-based algorithms for PAH, a hemodynamic diagnosis of PAH determined by RHC was recorded in only 26% of patients with PAH. 29 Important considerations for the use of riociguat in clinical practice are discussed below.
Riociguat dosing and administration
Riociguat is available as a film-coated tablet for oral administration. For patients who are unable to swallow whole tablets, riociguat tablets may be crushed and mixed with water or soft foods, such as apple sauce, immediately before use and taken orally. 30 Bioavailability is similar for whole and crushed tablets, and there are no clinically relevant food effects on oral absorption, although patients prone to hypotension should not switch between fed and fasted riociguat intake owing to increased peak plasma levels in the fasted compared with the fed state. 31
Riociguat exposure shows pronounced interindividual variability in patients with PAH and it is, therefore, administered using an individualized dose-adjustment scheme at treatment initiation. The recommended starting dose for riociguat is 1 mg three times daily (tid) for 2 weeks, with tablets being taken approximately 6–8 h apart. For patients with low blood pressure, physicians may consider starting riociguat at 0.5 mg tid. The dose should then be adjusted up to a maximum of 2.5 mg tid in 0.5 mg increments, according to signs and symptoms of hypotension. A summary of the individual dose-adjustment strategy for riociguat is illustrated in Figure 3. 32

Riociguat dose-adjustment strategy.
If riociguat treatment is interrupted for ⩾3 days, patients are advised to restart treatment at 1 mg tid for 2 weeks and continue treatment following the dose-adjustment scheme.33,34 Riociguat has a low risk of clinically relevant drug interactions; however, some drugs do affect riociguat exposure, and riociguat solubility may be influenced by gastric pH (Table 2).35,37,39
Drug interactions during concomitant use with riociguat and recommendations for management (adapted from Frey and colleagues 36 ).

ARV, antiretroviral; AUC, area under the curve; bid, twice daily; BP, blood pressure; Cmax, maximum serum concentration; FDC, fixed-dose combination; PD, pharmacodynamic; PDE5i, phosphodiesterase type 5 inhibitors; qd, once daily; tid, three times daily.
With regard to drug–drug interactions between riociguat and other PAH-targeted therapies, bosentan is known to reduce the exposure of riociguat; however, the reduction is not significant, and no dose adjustment is needed. It is important to note that sildenafil increases bosentan exposure; 43 therefore, patients who are switching from sildenafil to riociguat while maintaining bosentan therapy should be closely observed during the PDE5i washout period and immediately after the switch.
Real-world data from CAPTURE, an international, uncontrolled, retrospective chart review designed to assess how switching to riociguat is managed in clinical practice, showed that the recommended dose adjustment is generally followed successfully in clinical practice, and the majority of patients reach the maximum dose of 2.5 mg tid within 8 weeks. 44
Author opinion
There is a paucity of data in patients who do not closely resemble those enrolled in clinical trials (for example, those who have comorbidities, are elderly, or very young). As such, in some populations, it may be necessary to diverge from the recommended dosing schedule, by reducing the starting dose to 0.5 mg tid or extending the uptitration to 3–4 weeks, for example. If side effects occur during the dose-adjustment phase, riociguat should be reduced to the previously well-tolerated dose, usually by 0.5 mg tid. Following 2 or 3 weeks at this dose, uptitration may be attempted again through dose increases of 0.5 mg tid every 2–3 weeks.
Administration of riociguat may also be complicated by difficulty swallowing in populations such as the elderly; however, based on clinical experience, crushing riociguat tablets or cutting them in half does not result in any side effects or loss of bioavailability.
Blood pressure should be measured regularly during the riociguat dose-adjustment period. This is carried out by either a nurse during clinical visits or at home by the visiting nurse. In addition, where available and approved by the healthcare provider, patients may monitor their blood pressure at home and report the results to their healthcare professional. In patients who are concurrently treated for systemic hypertension (a common occurrence in the elderly population), reducing or even discontinuing the systemic antihypertensive medication may allow for straightforward uptitration of riociguat.
As hemoptysis was observed more often with riociguat treatment in PATENT-1 (56% of patients were receiving anticoagulants), 17 concomitant anticoagulation with riociguat requires cautious follow-up. If a patient does not have comorbidities such as atrial fibrillation, decisions regarding anticoagulation should be made on a case-by-case basis following assessment of benefit:risk for the individual patient, that is, in patients with SSc-associated PAH in whom anticoagulation has not proven beneficial.45,46
In the international, multicenter, prospective, noninterventional EXPERT registry, reflecting real-world riociguat use, 49% of patients were receiving anticoagulation therapy (unpublished data). In patients with PAH in EXPERT, the exposure-adjusted rates of hemoptysis/pulmonary hemorrhage were 2.5 adverse events (AEs) per 100 patient-years and 1.8 serious AEs (SAEs) per 100 patient-years (unpublished data). These rates were lower than those reported in PATENT-2, the long-term extension study of riociguat in PAH.20,21 The lower rate of bleeding seen in EXPERT could be due to a more careful exclusion of patients at risk of hemoptysis from riociguat treatment following publication of the SAE in the PATENT study. Despite the seemingly low risk of bleeding, an individual benefit:risk assessment during riociguat therapy is mandatory.
Use of riociguat in special patient populations
Some patients in need of PAH-targeted treatment have been underrepresented or not represented in clinical trials. Several recommendations concerning if, and how, riociguat should be managed and prescribed in these patients are summarized in Table 3.
Management of riociguat in special patient populations.
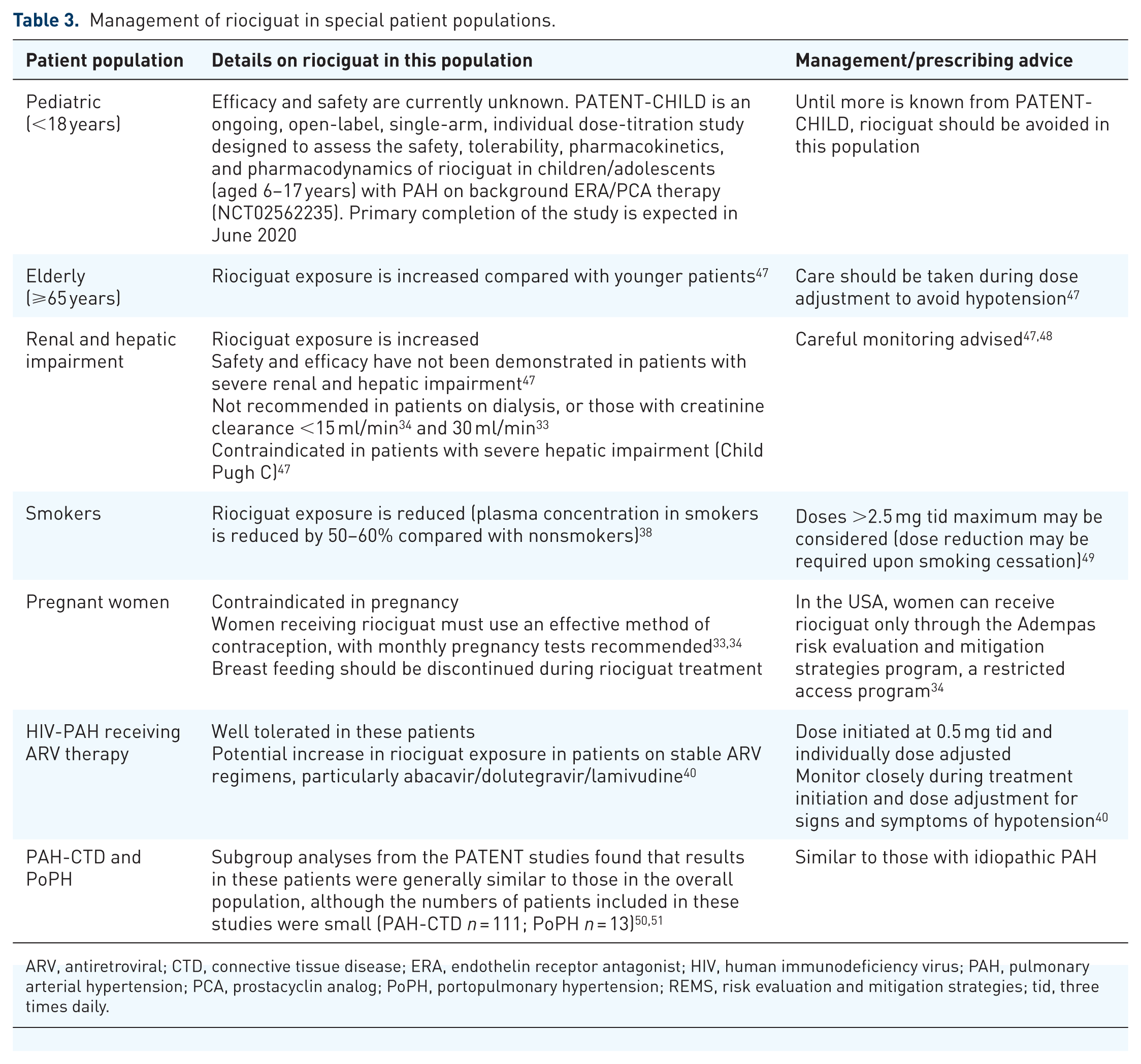
ARV, antiretroviral; CTD, connective tissue disease; ERA, endothelin receptor antagonist; HIV, human immunodeficiency virus; PAH, pulmonary arterial hypertension; PCA, prostacyclin analog; PoPH, portopulmonary hypertension; REMS, risk evaluation and mitigation strategies; tid, three times daily.
Author opinion
Although riociguat exposure is known to be altered in patients with hepatic and renal impairment, smokers, and the elderly, the recommended dose-adjustment scheme allows for appropriate management of these patients.
In elderly patients, particularly those with cardiopulmonary comorbidities, dose escalation of riociguat, and other PAH-targeted drugs, should be performed with caution. As noted in Table 3, riociguat is contraindicated in pregnant women and there is little or no clinical experience in this population. Riociguat is also contraindicated in patients with severe hepatic impairment (Child Pugh C) owing to limited experience in this population.
Management of AEs during riociguat treatment
Overall, riociguat is well tolerated in patients with PAH,17,52 and the AEs experienced with riociguat treatment are mostly explained by the underlying disease and mechanism of action of riociguat. Its safety profile was sustained in long-term clinical studies20,21 and in the EXPERT registry, designed to assess the safety of riociguat in clinical practice.
Commonly occurring AEs in the PATENT studies included headache, dizziness, dyspepsia, peripheral edema, nausea, diarrhea, vomiting, nasopharyngitis, and hypotension.17,21 The only drug-related SAEs occurring in patients receiving riociguat in the PATENT-1 study were three cases of syncope (1% of patients) and single cases of increased hepatic enzyme levels, dizziness, presyncope, acute renal failure, and hypotension. 17 Overall, syncope events were more common in the placebo group (4% versus 1% in riociguat patients). At 2 years in the PATENT-2 long-term extension, SAEs were recorded in 238 patients (60%), with 45 (11%) discontinuing treatment because of AEs. 21
Results from EXPERT were consistent with the known safety profile of riociguat, with 26% of newly-treated patients with PAH experiencing an AE considered to be study drug-related (compared with 7% of pretreated patients). Seven percent of patients experienced a study drug-related SAE (13% of newly-treated and 3% of pretreated patients). 53
Respiratory tract bleeding was rare in the riociguat clinical studies, although serious bleeding occurred more frequently with riociguat (2%, 12/490 patients) than with placebo (0%, n = 214). In the EXPERT registry, 2% (n = 8) of patients with PAH experienced hemoptysis. There was no link between an increased risk of respiratory tract bleeding events and antithrombotic therapy, treatment with vitamin K antagonists, or the quality of international normalized ratio in the PATENT studies. Riociguat should be prescribed with caution in patients with a prior history of hemoptysis, and a patient’s risk of respiratory tract bleeding should be regularly assessed during riociguat treatment.
Author opinion
The common AEs experienced during treatment with riociguat are generally not problematic for patients and can be managed using the strategies outlined in Figure 4. Furthermore, patient adherence to treatment is not affected in those who are informed of potential AEs and how to manage them, and no specific monitoring for AEs is necessary. In some patients, however, it may be advisable to schedule patient visits more frequently to monitor AEs such as hypotension. In the case of syncope, hemoptysis, and pulmonary hemorrhage, riociguat should be stopped immediately.

Riociguat in combination with other PAH-targeted therapies
Patients with PAH are often treated with upfront combination therapy or, as PAH progresses, with sequential combination therapy. Sequential combination of riociguat with ERAs and PCAs has been shown to be beneficial, with the PATENT-1 study demonstrating that the benefit of riociguat was consistent in patients who were receiving ERAs (44% of patients) and inhaled or subcutaneously administered PCAs (6% of patients), and in those who were receiving no other treatment for PAH. 17 Similarly, patients participating in PATENT-2 who were receiving long-term riociguat monotherapy or in combination with ERAs or PCAs experienced similar sustained improvements in clinical and functional status at 2 years. 21
In the PATENT studies, there was no difference in safety when patients were treated with riociguat alone or with combined therapy. Safety data for use of riociguat in combination with other PAH-targeted therapies in real-world clinical practice are available from EXPERT and CAPTURE, with most patients with PAH in these studies receiving riociguat in combination with ERAs.44,53 In an analysis of the EXPERT registry (where most patients with PAH were receiving riociguat in combination with ERAs), riociguat was generally well tolerated with no new safety signals. In CAPTURE, the most common postswitch therapies were a combination of an ERA with riociguat (68%), and triple combination of an ERA, riociguat, and a PCA (18%). Both studies found that riociguat was well tolerated in combination with other PAH-targeted therapies, and had a similar safety profile to riociguat monotherapy. 44
An ongoing independent, prospective, open-label study of up-front combination therapy with riociguat and ambrisentan has also found that the combination is well tolerated and associated with improvements in hemodynamics and right ventricular function within 4 months. 55 A retrospective chart review of 15 intermediate- or high-risk patients receiving an open-label combination of riociguat and macitentan found significant improvements in 6MWD, NT-proBNP, WHO FC, and hemodynamics (PVR, mPAP, cardiac index) over a median of 12 months. At 1-year follow-up, 47% of patients had achieved a low-risk status. There were no unexpected side effects, and the transplant-free survival rate was 85% at 36 months. 56
Riociguat and PDE5i: contraindication and switching therapy
In the blinded, randomized PATENT PLUS study, patients with PAH receiving sildenafil (20 mg tid) were randomized to placebo or riociguat (up to 2.5 mg tid) for 12 weeks. 39 In the long-term extension phase of the study, potentially unfavorable safety signals were observed, primarily a high incidence of discontinuation as a result of hypotension, with no evidence of a positive benefit:risk ratio. As a result, the use of PDE5i with riociguat is contraindicated. 5
More recently, the possibility of switching to riociguat from PDE5i has been investigated in RESPITE, a 24-week, uncontrolled, open-label, multicenter pilot study to determine whether replacing PDE5i with riociguat in patients with PAH is safe and feasible. 57 Patients switching from sildenafil or tadalafil to riociguat were permitted to continue background therapy with ERAs if they had been receiving stable treatment for ⩾90 days. Of the 61 patients enrolled in the study, 82% were receiving concomitant ERA treatment at baseline. At Week 24, replacing PDE5i with riociguat resulted in improvement from baseline in hemodynamic variables, NT-proBNP, and clinical endpoints, including 6MWD and WHO FC, in the 51 patients who completed the study.
The 24-week, open-label Riociguat rEplacing PDE-5i Therapy evaLuated Against Continued PDE-5i thErapy (REPLACE) study is currently ongoing, and will provide further data on switching to riociguat. REPLACE is a randomized, controlled study designed to investigate the potential clinical benefit of switching from PDE5i to riociguat in patients who are not achieving treatment goals with PDE5i (NCT02891850).
Although switching from PDE5i to riociguat is not recommended in the current treatment guidelines, 5 the riociguat prescribing information provides recommended treatment-free periods to be used should patients switch between the drugs. A PDE5i washout period of 24 h for sildenafil or 48 h for tadalafil is recommended before initiating riociguat, and a washout of 24 h if switching from riociguat to PDE5i. 44 Patients should be monitored for any signs and symptoms of hypotension after switching.
Switching from PDE5i to riociguat in real-world clinical practice was evaluated in CAPTURE, an international, multicenter, uncontrolled, noninterventional, retrospective chart review designed to evaluate how and why patients with PAH and CTEPH are switched to riociguat in real-world clinical practice. 44 Of patients with PAH, most were receiving ERA + PDE5i (60%) or ERA + PDE5i + PCA (23%) at the time of switching, and 85% switched to riociguat from PDE5i. The majority of patients maintained their ERA or PCA treatment. The main reason for switching to riociguat was lack of efficacy of previous PAH-approved therapies. The recommended dose adjustment was followed and the recommended treatment-free period when switching to riociguat from sildenafil was used. However, a slightly longer period than recommended for tadalafil was used. Most patients did not receive riociguat and PDE5i therapy concomitantly, in line with the contraindication. 44 A number of independent studies have also highlighted the feasibility of switching patients to riociguat from PDE5i in patients with PAH.58–61
Author opinion
Switching from PDE5i to riociguat (usually owing to lack of PDE5i efficacy) should be performed only within expert centers participating in the ongoing REPLACE study, as all thus far completed studies of switching were not randomized controlled trials. Until further data are available, switching cannot be recommended outside clinical trials.
In our experience, switching patients from riociguat to PDE5i is unusual in clinical practice, but may be used for patients who experience AEs with riociguat. In current practice, almost all patients with PAH receiving riociguat also receive an ERA.
Implementing risk assessment tools in the clinic
Treatment of patients with PAH is characterized by a complex strategy that includes an initial evaluation of severity and then continued assessment of patient response to treatment.5,16,62
The 2015 European Society of Cardiology (ESC)/European Respiratory Society (ERS) treatment guidelines provide a tool for regular risk assessment of patients, allowing for prediction of 1-year mortality based on risk stratification according to 13 variables. 5 Using identified parameters of prognostic relevance derived from registry analyses, a number of risk assessment tools have since been developed, including three abbreviated versions of the ESC/ERS risk stratification tool,7,63,64 and the weighted REVEAL risk score calculator 65 (an updated tool, REVEAL 2.0, was recently developed 66 ). The prognostic abilities of each of these tools have been investigated post hoc in patients in the PATENT database, demonstrating that riociguat decreases patient risk of 1-year mortality, and that each method can discriminate between low-, medium-, and high-risk patients in terms of survival and clinical worsening-free survival over 2 years.25,26,67
Author opinion
If patients receiving an ERA, PCA, or both, are not achieving a low-risk status, adding riociguat is an option. Likewise, if a patient receiving riociguat is not achieving a low-risk status, an ERA or PCA (or both) may be added.
Patient management
Expert healthcare and the introduction of targeted therapies have improved outcomes for patients with PAH in terms of symptom management and disease progression. 5 As patients live longer, new challenges arise that go beyond diagnosis and treatment of their condition. The physical and psychological effects of PAH can severely impair patient relationships with family and friends, their ability to work, cope, and handle stressors, and their QoL.68,69
A number of studies, including PATENT-1,70–74 have found that PAH-targeted treatments are associated with improved QoL, and therefore patient adherence is important not just for improving a patient’s condition, but also for their QoL. Actively involving patients with PAH in their own treatment and self-care from the time of diagnosis improves outcomes at lower healthcare costs.75–77
Author opinion
Depending on the individual patient, support may be needed from multiple specialists, such as pneumologists, cardiologists, transplant critical care physicians, rheumatologists, radiologists, hepatologists, psychosomatic physicians, and nephrologists.
In the authors’ opinion, specialist nurses are critical for both in- and out-patient visits and for patient contact between visits, and positive experiences have been reported with telephone hotlines and regular (often weekly during the dose-adjustment phase) telephone contact between patient and nurse.
Patient adherence can be encouraged if a patient recognizes and understands the importance of treatment and can feel its benefit. In particular, the improved exercise capacity resulting from treatment can lead to an increased QoL and social life. Specialized rehabilitation programs, supervised by PH experts, can help to optimize patients’ awareness and handling of their physical abilities and limitations.
Conclusion
Efficacy and safety of riociguat in patients with PAH were demonstrated in the phase III PATENT-1 study. Improvements were maintained in PATENT-2, and no new safety signals were observed. Riociguat is well tolerated, and AEs experienced by patients can generally be managed simply in clinical practice.
Riociguat dosing is based on an individualized dose-adjustment scheme. Dosing adjustments should be made with caution in patients who display altered riociguat exposure. Currently, in patients with PAH, riociguat may be prescribed as monotherapy or in combination with ERAs or PCAs, but combination with PDE5i is contraindicated.
Since its introduction, riociguat has become an important part of the management of patients with PAH. Physicians should be aware of the specific needs of their patients, particularly those in special populations not specifically represented in clinical trials, so that the efficacy of treatment can be optimized while minimizing AEs.
Supplemental Material
Author_response_v.1 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Author_response_v.1 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Author_response_v.2 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Author_response_v.2 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Reviewer_1_v.1 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Reviewer_2_v.1 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.1 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Reviewer_3_v.1 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.2 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Reviewer_3_v.2 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_3_v.3 – Supplemental material for Practical management of riociguat in patients with pulmonary arterial hypertension
Supplemental material, Reviewer_3_v.3 for Practical management of riociguat in patients with pulmonary arterial hypertension by Michael Halank, Kristin Tausche, Ekkehard Grünig, Ralf Ewert and Ioana R. Preston in Therapeutic Advances in Respiratory Disease
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: Editorial assistance was provided by Adelphi Communications Ltd, funded by Bayer AG.
Conflict of interest statement
MH reports personal fees and nonfinancial support from AstraZeneca, Actelion, Bayer AG, Berlin Chemie, GSK, MSD, Novartis, and OMT. KT reports no conflicts of interest. EG reports grants and personal fees from Actelion, Bayer AG, and MSD; grants from GSK, Novartis, and United Therapeutics; and personal fees from SCOPE, OrPha Swiss GmbH, and Zurich Heart House. RE reports personal fees from Actelion, Bayer AG, GSK, MSD, Novartis, and OMT and grants from Actelion and OMT. IRP reports grants and personal fees from Actelion, Arena, Bayer AG, Gilead, and United Therapeutics; grants from Liquidia; and personal fees from Pfizer and Reata.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.