
Abstract
Background:
Pleurodesis is often used to prevent the re-accumulation of a malignant pleural effusion (MPE). Intrapleural urokinase (IPUK) therapy facilitates lung re-expansion for patients with loculated MPE or a trapped lung that allows subsequent pleurodesis. MPE management has been traditionally regarded as a symptomatic treatment. We tried to evaluate their impact on patient survival.
Methods:
There were 314 consecutive patients with symptomatic MPE that underwent minocycline pleurodesis with (n = 109) and without (n = 205) the antecedent IPUK therapy between September 2005 and August 2015, who were recruited for the pleurodesis outcome and survival analysis.
Results:
The rate of successful pleurodesis was similar between the simple pleurodesis group and the IPUK therapy group followed by the pleurodesis group (69.0% versus 70.5%; p = 0.804). The patients who succeeded pleurodesis had a longer survival rate than those who failed in either the simple pleurodesis group (median, 414 versus 100 days; p < 0.001) or the IPUK therapy followed by pleurodesis group (259 versus 102 days; p < 0.001). The survival differences remained when the lung and breast cancer patients were studied separately.
Conclusion:
Successful pleurodesis translated into a better survival rate that promotes performing pleurodesis on lung re-expansion. The apparent shorter survival of the patients with loculated MPE or trapped lung, and those that did not respond to the IPUK therapy, lowered the probability of the survival benefit through the simple physical barrier by the fibrin formation to prevent the tumor spreading. The successfully induced inflammatory response by minocycline is supposed to prohibit the tumor invasion and metastasis. Further studies are warranted to clarify the mechanism and provide opportunities to develop novel therapeutic strategies.
Introduction
Current therapeutic options for malignant pleural effusion (MPE) include catheter pleural drainage or repeated thoracenteses.1,2 Chemical pleurodesis following catheter drainage aims to obliterate the pleural space to prevent fluid re-accumulation. Several categories of sclerosing agents were used with a success rate of 70–80%.1,2
For the medically inoperable cancer patients with loculated MPE or trapped lung, intrapleural fibrinolytic therapy using urokinase or streptokinase is a well-tolerated and useful nonsurgical adjunct therapy to break down fibrin and allow the ipsilateral lung re-expansion.3–6 Furthermore, when followed by successful pleurodesis, it will obviate the significant morbidities associated with repeated thoracenteses, or the risk of an indwelling intrapleural catheter with fibrous occlusion and catheter-related infection.
Pleurodesis is traditionally regarded as a symptomatic treatment, with rarely mentioned benefits on patient survival in previous literature. We had an incidental finding that patients with successful minocycline pleurodesis had a significantly longer cancer-specific survival rate than those without in a small patient group (n = 26). 7 The findings encouraged us to analyze more patients with MPE undergoing minocycline pleurodesis including those that required antecedent intrapleural urokinase (IPUK) therapy retrospectively over a 10-year follow-up period to confirm the trend and explore the possible underlying mechanism.
Materials and methods
Study population
Between September 2005 and August 2015, patients with symptomatic MPE requiring drainage with a size 8–14 Fr self-retaining catheter (SKATERTM Single step drainage set; Argon Medical Devices, TX, USA) at the Sun Yat-Sen Cancer Center, Taiwan, a 200-bed hospital, were recruited (Figure 1). All patients signed an informed consent for the procedures and the retrospective review of the data. The Institutional Review Board of the hospital approved this study (no.20160223A).

Treatment algorithm, patient distribution, and the pleurodesis outcome.
To maintain consistency in the evaluation of the radiographic results following the catheter drainage, we adopted the scoring system proposed by Bouros and colleagues. 8 The dimensions of the pleural fluid loculations or extrapulmonary air spaces were estimated by measuring the two orthogonal maximal diameters of either the effusion or air space on the chest radiographs. The overall reduction in dimension of the pleural fluid volume or extrapulmonary air collections was categorized as being one of the following: 0 (no change), 1 (less than one-third improvement), 2 (improvement of between one and two thirds), and 3 (more than two-thirds improvement).
The decision to perform pleurodesis or the IPUK therapy followed by feasible pleurodesis was made according to the scoring system.
Simple pleurodesis group
For patients who had a score of three for their level of radiographically determined improvement, 8 the infusion of minocycline (Mirosin; Taiwan Panbiotic Laboratories, Kaohsiung, Taiwan) for pleurodesis at a dosage of 7 mg per kg was performed, if the pleural drainage had fallen to a level of less than 150 ml every 24 h for 2 consecutive days.
Intrapleural urokinase therapy followed by pleurodesis group
Patients with persistent dyspnea in the presence of substantial residual loculated pleural effusions, or trapped lung, were evaluated for IPUK therapy. The locule walls or peels surrounding the trapped lung were less than 5 mm in thickness. The size of the residual pleural fluid collection or the extrapulmonary air occupied more than one-third of the chest height on the chest radiographs. A bronchoscopy was performed to exclude the possibility of endobronchial obstruction as and when needed. Patients with bleeding diathesis, designated medical conditions contraindicating the application of fibrinolytic therapy, and major thoracic or abdominal surgery within 10 days were excluded. 6
Eligible patients were infused with 100,000 IU urokinase (Green Cross, Osaka, Japan) in 100 ml saline via an intrapleural catheter, on a daily basis for 3 consecutive days. The dosages and procedure of the IPUK therapy were based on the published experience pertaining to patients with parapneumonic effusions and empyema by Bouros and colleagues. 8 Urokinase was re-instilled for a partial response following the earlier instillations.
For patients who had a score of three radiographic improvements, 8 an infusion of minocycline for pleurodesis was performed in a similar manner as described in the simple pleurodesis group.
All the patients received treatment of the underlying primary tumors according to the current guidelines and were followed by medical oncologists.
Assessment of pleurodesis outcomes
Follow-up chest radiographs were obtained at 1, 3, and 6 months after pleurodesis and repeated as and when required. The outcome of pleurodesis was determined according to the relevant definitions proposed by the American Thoracic Society and the European Respiratory Society Consensus Statement. 1 Complete success was defined as the long relief of symptoms related to the effusion, with the absence of fluid re-accumulation on the chest radiograph until death. Partial success was defined as the diminution of dyspnea related to the effusion, with only partial re-accumulation of fluid (less than 50% of the initial), with no further therapeutic thoracenteses required for the remainder of the patient’s life. Lack of success as defined above belongs to the failed pleurodesis.
Survival analysis
The survival time was calculated from the date of diagnosis of MPE and censored at the date of death or the last follow up. The survival rate was compared between the patients that had succeeded and failed pleurodesis in both the simple pleurodesis group and the IPUK therapy followed by pleurodesis group. Survival analyses were also separately completed on the lung cancer and breast cancer subgroup to discriminate the effect of tumor heterogeneity. Univariate analysis including the presence of other sites of distant metastasis than MPE, age, sex, Eastern Cooperative Oncology Group performance score, and smoking history, followed by the multivariate analysis if indicated, to decide as to whether the successful pleurodesis was an independent prognosticator. The survival of the patients with loculated MPE, or trapped lung, that failed to respond to the IPUK therapy was also analyzed.
Statistical analysis
Descriptive statistics of the mean, median, standard deviation, and frequency were used to process the demographic data. Continuous variables were compared using the two-sample Student’s t test, whereas the categorical variables were compared using the Chi-square test or the Fisher’s exact test. Survival estimates were derived by Kaplan–Meier plots, while the log-rank tests were used to assess the differences in survival. Multivariate analysis of the overall survival rate was evaluated according to the Cox proportional hazards model by using the clinical prognostic factors with significant differences in the univariate analysis. A p value <0.05 for comparisons was considered to represent a statistical significance. All analyses were performed using the statistical software package SAS, version 9.4 (SAS Institute; Cary, NC, USA).
Results
Between September 2005 and August 2015, 1351 patients were diagnosed with MPE. Among them, 618 patients symptomatic from MPE required the pigtail intrapleural catheter drainage (Figure 1). There were 205 patients (with a mean age of 58.6 years; range, 19–89, and 144 women), that achieved adequate pleural fluid drainage and ipsilateral lung re-expansion and were therefore eligible for minocycline pleurodesis (Table 1). There were 184 patients with loculated pleural effusion, or trapped lung, after catheter drainage that were eligible for IPUK therapy. Among them, 109 (59.2%) patients (with a mean age of 59.1 years; range, 20–88, and 88 women) achieved the ipsilateral lung re-expansion following IPUK therapy that allowed the subsequent minocycline pleurodesis (Table 1). The mean dosage of the IPUK instillations per patient was 360,000 IU (range, 300,000–900,000 IU). The median time lapse between the administration of the final dosage of IPUK and the start of pleurodesis was 4 days. For the 75 IPUK nonresponders, 18 patients underwent thoracoscopy or decortication, and 30 patients adopted the intrapleural catheter as indwelling usage and removed it later. The remaining patients had the catheter removed and returned for repeated thoracenteses as and when required.
Characteristics of the patients who underwent minocycline pleurodesis with and without antecedent intrapleural urokinase therapy.

IPUK, intrapleural urokinase.
There were no major complications following the minocycline pleurodesis, except for minor pain manageable with analgesics. Overall four patients (2.2%) suffered from major complications following the IPUK therapy, three developed an immediate hemothorax, and one had Pseudomonas aeruginosa empyema during the process of the lung re-expansion. All four episodes were resolved after adequate management. The inpatient hospital days were longer in the IPUK therapy followed by pleurodesis group than the simple pleurodesis group (13.3 ± 2.7 versus. 6.0 ± 2.8; p = 0.024).
Pleurodesis outcomes
In the simple pleurodesis group, 142 patients (69.3%) were assessable for the pleurodesis outcome. The median follow up was 276 days (13–2283 days). Among them, 70 patients achieved complete success and 28 patients achieved partial success (69.0% successful rate total).
In the IPUK therapy followed by pleurodesis group, 95 patients (87.2%) were assessable for the pleurodesis outcome. The median follow up was 190 days (7–2208 days). Among them, 42 patients achieved complete success and 25 patients achieved partial success (70.5% successful rate total).
The rate of successful pleurodesis was similar between the simple pleurodesis group and the IPUK therapy group followed by pleurodesis group (p = 0.804).
The patients with the extremely short follow up belonged to the failure group with rapid pleural fluid re-accumulation. For the 77 patients not assessable for the outcome (63 in the simple pleurodesis group and 14 in the IPUK followed by pleurodesis group), 39 patients were transferred to other hospitals for further treatment or palliative care earlier to determine the pleurodesis outcome. There were 15 patients lost to follow up. Chest radiograph was not followed as scheduled in 17 patients. A total of six patients died soon after the minocycline pleurodesis.
Survival analysis
In the simple pleurodesis group, patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed pleurodesis [median, 414 versus 100 days; p < 0.001; Figure 2(a)]. Univariate analysis showed that successful pleurodesis was the only prognosticator with significance [hazard ratio, 0.271; 95% confidence interval (CI), 0.18–0.41; p < 0.001].

In the simple pleurodesis group, patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed (a). In the IPUK therapy followed by pleurodesis group, patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed (b). Similar survival differences in both groups were observed when studied the lung cancer (c and d) and breast cancer (e and f) patients separately.
In the IPUK therapy followed by pleurodesis group, patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed pleurodesis [median, 259 versus 102 days; p < 0.001; Figure 2(b)]. Univariate analysis showed that successful pleurodesis was the only prognosticator with significance (hazard ratio, 0.374; 95% CI, 0.23–0.61; p < 0.001).
Lung cancer patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed, in either the simple pleurodesis group [median, 560 versus 108 days; p < 0.001; Figure 2(c)], or the IPUK therapy followed by pleurodesis group [median, 350 versus 94 days; p = 0.004; Figure 2(d)]. Univariate analysis showed that successful pleurodesis remained the only prognosticator with significance (hazard ratio, 0.236; 95% CI, 0.15–0.38; p < 0.001).
Breast cancer patients who completely or partially succeeded pleurodesis had a significantly longer overall survival rate than those that failed in either the simple pleurodesis group [median, 318 versus 106 days; p = 0.013; Figure 2(e)] or the IPUK therapy followed by pleurodesis group [median, 247 versus 116 days; p = 0.001; Figure 2(f)]. Univariate analysis showed that successful pleurodesis remained the only prognosticator with significance (hazard ratio, 0.357; 95% CI, 0.21–0.61; p < 0.001).
After catheter drainage, patients with loculated MPE, or trapped lung, had a shorter survival rate than those with the near-complete ipsilateral lung re-expansion [median, 135 versus 180 days; p = 0.027; Figure 3(a)]. The patients with loculated MPE, or trapped lungs that did not respond to the IPUK therapy had a similar survival rate to those that failed pleurodesis in either the simple pleurodesis group [median, 77 versus 100 days; p = 0.665; Figure 3(b)], or the IPUK therapy followed by pleurodesis group [median, 77 versus 102 days; p = 0.725; Figure 3(c)].
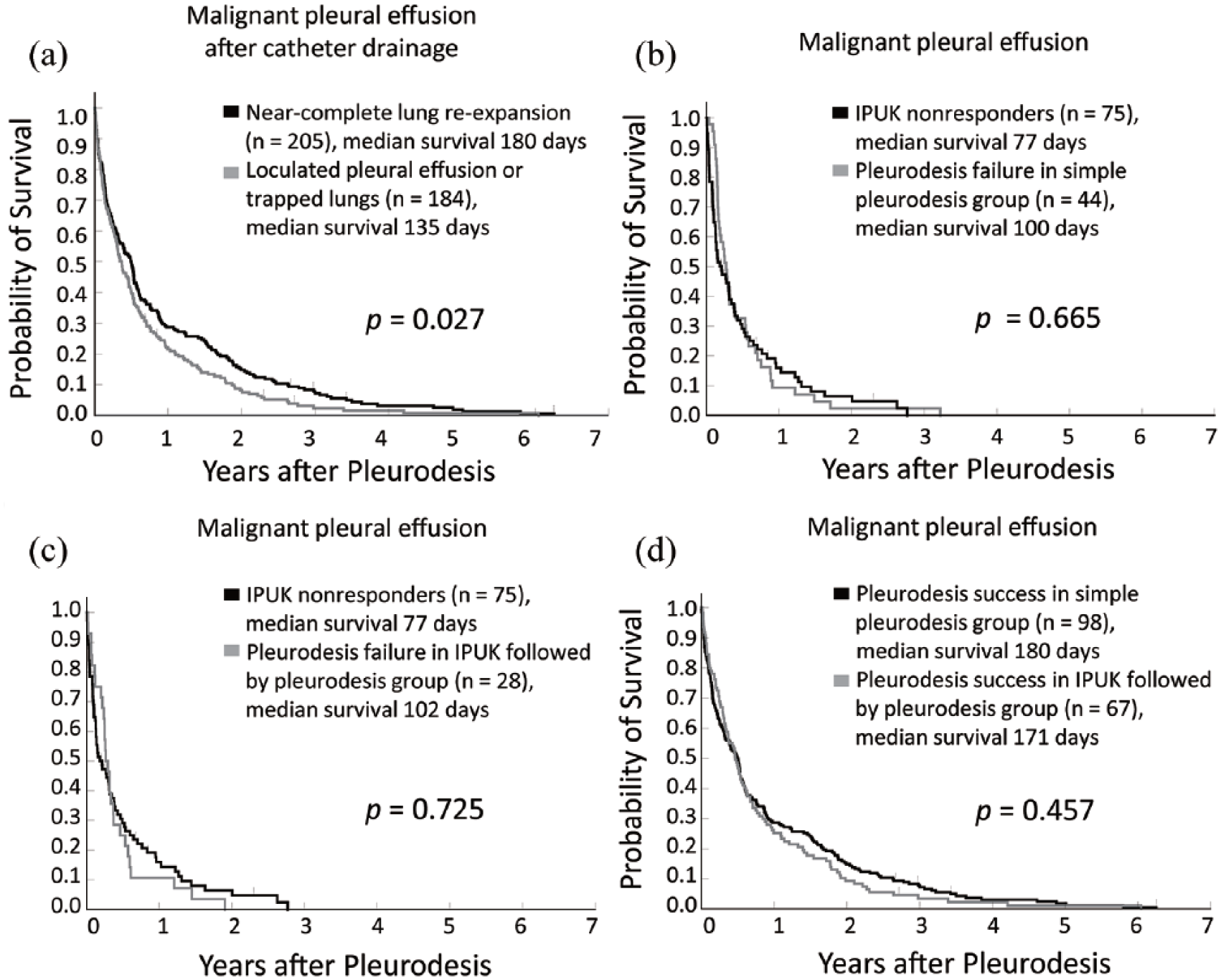
After catheter drainage, the patients with loculated MPE, or trapped lung, had a shorter survival rate than those with a near-complete ipsilateral lung re-expansion (a). The IPUK nonresponders among them had a similar survival rate to those that failed pleurodesis in the simple pleurodesis group (b) and the IPUK therapy followed by pleurodesis group (c), respectively. For patients who completely or partially succeeded pleurodesis, there was no survival difference between the simple pleurodesis group and the IPUK therapy followed by pleurodesis group (d).
For patients who completely or partially succeeded pleurodesis, there was no survival difference between the simple pleurodesis group and the IPUK therapy followed by pleurodesis group [median, 180 versus 171 days; p = 0.457; Figure 3(d)].
Discussion
In 2006, we reported the first prospective cohort study and suggested that IPUK is a well-tolerated and useful adjunct therapy for loculated MPE, or trapped lungs, in medically inoperable cancer patients. 6 Thereafter, Okur and colleagues, and Saydam and colleagues, conducted two randomized controlled studies of intrapleural fibrinolytic therapy using another agent (streptokinase) for loculated MPE that demonstrated similar benefits.9,10 However, a recent randomized controlled trial of IPUK versus placebo for nondraining MPE by Mishra and colleagues, reported against the benefit in dyspnea relief, despite the significant improvements in radiographic appearance, hospital stay, and survival. 11 The differences in the degree of dyspnea and the pleural effusion amount at the study enrollment may affect the measurement of dyspnea relief. On the other hand, we excluded the patients with locule walls or peels surrounding the trapped lung with more than 5 mm in thickness, as those were expected refractory to fibrinolytic. Mishra and colleagues excluded patients with a survival rate of fewer than 28 days, and those with a trapped lung may well benefit more from IPUK therapy. 11 The treatment protocol also differed, although with a similar total dosage. In the study of Mishra and colleagues, three doses of 100,000 IU urokinase were infused at 12-hour intervals followed routinely by talc slurry pleurodesis 24 h later, regardless of the ongoing fluid drainage volume and the chest radiograph appearance. We infused urokinase for 3 consecutive days when loculated effusion became evident after a median of 5 days following the catheter drainage. Minocycline pleurodesis was performed when the daily drainage was less than 150 ml for 2 consecutive days with evidence of lung re-expansion after IPUK therapy. The median time lapse between the last dosage of IPUK and pleurodesis was 4 days.
The rate of successful pleurodesis in the IPUK therapy followed by pleurodesis group (70.5%) was similar to that of the simple pleurodesis group (69%) and comparable with the results of the studies describing the chemical pleurodesis using a tetracycline analog.1,2 The remnant urokinase and its metabolites in the pleural space following IPUK therapy did not counteract the action of minocycline and led to pleurodesis failure. The studies of Okur and colleagues, Saydam and colleagues and Mishra and colleagues also concurred with this finding.9–11
Minocycline was used in the study instead of alternative agents such as graded talc. The usage of thoracoscopy to remove the fluid followed by talc poudrage appeared to be the most promising method to prevent fluid re-accumulation. 12 However, the talc powder could not be blown through a catheter into the pleural cavity. The potential disadvantages of talc slurry include a lack of uniform distribution; accumulation in the dependent areas of the pleural space, possibly leading to incomplete pleurodesis and loculations; and a decreased direct contact time with the pleural surface, due to the liquid suspension, with a subsequent decrease in effectiveness. 1 The selection of a sclerosing agent also depended on the local availability, experience, and their adverse events, which may not be identified in randomized trials. 13
In our study, the patients that succeeded minocycline pleurodesis had a significantly longer survival rate than those that failed (Figure 2). The antecedent IPUK therapy did not affect the survival rate [Figure 3(d)]. The apparent shorter survival of patients with loculated MPE, or trapped lung [Figure 3(a)], and those that did not respond to the IPUK therapy [Figure 3(b and c)], lowered the probability of the survival benefit through the simple physical barrier by the fibrin formation to prevent the tumor spreading.
The mesothelium itself may regulate the first step of the pleural fibrosis following the instillation of a sclerosing agent, through the inflammatory response, which is decisive for the pleurodesis outcome and survival. Cytokines are signaling molecules that are key mediators of inflammation.14,15 They can be generally classified as proinflammatory and tumorigenic, or as anti-inflammatory and tumor suppressive.15–18 Depending on the balance of cytokines, their collective effect can be either pro- or anti-tumorigenic. Whether the therapy-induced acute inflammation is a friend or a foe remains to be debated as it may well stimulate cancer cell growth. Conversely, it has also been found to stimulate antigen presentation by tumor-infiltrating dendritic cells, and to induce the production of cytokines (e.g. interleukin-1 beta) that stimulate the anti-tumor immunity.14,19,20 In our preliminary study between September 2015 and April 2016, 15 consecutive patients (breast cancer in 8, lung cancer in 6) with MPE undergoing minocycline pleurodesis were evaluated. The pleural fluid levels of the interleukin-1 beta and interleukin-10 were elevated after the instillation of the sclerosing agent in the nine patients that succeeded pleurodesis (lung cancer in five, breast cancer in four; unpublished data). At follow up, patients who succeeded pleurodesis also had a significantly longer survival rate than those that failed. The selective elevation of the anti-inflammatory cytokines suggests an anti-tumor effect and translates to a longer survival. More patients will be recruited to confirm this trend. Further studies to observe the release of inflammatory cytokines from the mesothelial cell after the addition of the sclerosing agent,21–23 and the effects of the conditional media, inflammatory cytokines and their antagonists on cancer cell viability, proliferation, migration, and invasion are warranted to clarify the mechanism, and thereby provide opportunities to develop the novel therapeutic strategies.
The decision-making process to choose the most beneficial treatment for MPE continues to be a challenge for clinicians. In addition to, and from the viewpoint of the expected survival, cost-effectiveness, and pleural elastance,24–26 the results encouraged us to perform pleurodesis on lung re-expansion. As the renowned thoracoscopist Philippe Astoul, Hôpital Nord-Marseille, France, said, the current standard palliative methods are suboptimal with a few drawbacks. The new targets for the treatment of MPE in the future will be several mediators enrolled in the biological cascade. 27
To the best of our knowledge, this is the largest MPE patient population involved with minocycline pleurodesis and intrapleural fibrinolytic therapy with the longest follow up. However, there are several limitations that need to be addressed, which include the retrospective study design, and a significant proportion of the patients were not evaluable due to either a lost or a too short follow up. Our patients with breast cancer and MPE had a shorter survival rate than those with lung cancer that may well be attributed to a higher percentage of MPE in the breast cancer patients presented as a relapsed disease (66/72, 91.7%,), when compared with the lung cancer patients (59/134, 44.03%). In fact, we have also found the survival of some patients with MPE was extraordinarily longer than that expected in the literature. Ethnic differences between western and eastern countries in terms of the clinico-epidemiology and the treatment outcome of the patients should be considered. We conceived this study before the development of the LENT score for prognostication in patients with MPE, which may allow a more precise survival comparison between the groups. 28 Patients with a better survival and performance status mount a better inflammatory response in pleura that may lead to a higher pleurodesis success rate. Despite all the patients undergoing treatment of the underlying primary tumors according to the current guidelines after the minocycline pleurodesis, the compliance and response to the anti-cancer treatments need to be ascertained. We also need to address the comorbidities using a validated risk adjustment score that predicts the mortality and resource utilization, such as the Deyo’s Charlson comorbidity index. 29 Several drivers of lung cancer, such as EGFR (55.7%), KRAS (5.2%), BRAF (2.0%), HER2 (0.7%) mutations, and EML4-ALK translocation have been recognized in recent years and can be treated with drugs. 30 The estrogen receptor/progesterone receptor/human epidermal growth factor receptor 2 status also affects the treatment and prognosis in breast cancer. The successful response to pleurodesis may also depend on the positive response to systemic therapy, especially the usage of targeted therapy in patients with driver oncogenes. The problems of confounding therapeutic factors can be solved by a randomized controlled trial with adequate stratification in the future.
Conclusion
The present study showed that patients who succeeded minocycline pleurodesis with and without the antecedent IPUK therapy have a longer survival rate. The findings promote performing pleurodesis on lung re-expansion. The successfully induced inflammatory response should be considered as a positive way to prohibit tumor invasion and metastasis.
Footnotes
Acknowledgements
This work was presented at the 18th World Conference on Lung Cancer, Yokohama, Japan, October 15–18 2017.
Y-F.L. and S-H.K. contributed equally to this article as co-senior authors.
The authors would like to offer their sincere thanks to Dr Hsiang-Yi Lin, Dr Ming-Chih Chern, Dr Yung-Yi Cheng, Dr Chu-Yun Chen, Dr Chi-Feng Chung, Dr Mau-Ching Wu, Dr Peng-Yu Chen, and Dr Lun-Wei Chiou for their assistance with the procedure and follow up; Mr Michael Wise for his help with the English language editing; Miss Yun-Ying Chen, Miss Shiao-Chiu Huang, and Miss Mei-Chun Chen for their assistance with the figures, data and references preparation.
Funding
This study was funded by the Ministry of Science and Technology, Taiwan (grant numbers MOST 106-2314-B-368-001).
Conflict of interest statement
The authors declare that there is no conflict of interest.