
Abstract
Background:
Pericardial effusion is an independent predictor of mortality in patients with pulmonary arterial hypertension (PAH). However, the management and outcomes of patients with pulmonary hypertension (PH) and pericardial effusion are not well described.
Methods:
A retrospective, observational study was conducted at Baylor College of Medicine and The Methodist Hospital by screening all patients admitted between 1 June 2005 and 1 June 2010 with the International Classification of Diseases, ninth revision codes for PH and pericardial effusion. A total of 138 patients were identified, and 103 patients were excluded on the basis of valvular heart disease, recent surgery or end-stage renal disease. Thirty-five patients with PH diagnosed by a historical right heart catheterization or echocardiography and with documented pericardial effusion were included in this analysis. Demographic, hemodynamic, laboratory and survival data were collected.
Results:
The mean age was 49.5±36 years (mean ± standard deviation), 31 of 35 patients were women (93%) and pulmonary artery systolic pressure was 77 ± 19 mmHg. Mean follow-up period was 20.5 ± 12.9 months. Fifteen patients had PAH associated with connective tissue disease (50%). The majority of the patients (87%) with pericardial effusion were managed conservatively. Four patients (13%) who were hemodynamically unstable underwent pericardial window placement. One of them was started on epoprostenol, and two patients had the doses of PAH-specific medications uptitrated. Three of four pericardial window patients survived to the conclusion of the follow-up period. The overall survival in our cohort was 60%, with three patients lost to follow-up.
Conclusions:
Connective tissue disease associated PAH and female sex were predominant in our cohort of patients with pericardial effusion. Seventy-five percent of patients who were treated with pericardial window for hemodynamically unstable pericardial effusion survived until the end of the study period. Pericardial window may be a therapeutic option in patients with unstable PH with pericardial effusion. Further studies are needed to determine the optimal treatment strategy for such patients.
Background
Pericardial effusion in patients with pulmonary arterial hypertension (PAH) has been identified as an independent mortality risk factor with a hazard ratio of 1.35 [Benza et al. 2010]. PAH due to connective tissue disease such as scleroderma with pericardial effusion may confer additional risk [Benza et al. 2010; Campo et al. 2010; Dunne et al. 2011]. Data from the REVEAL registry suggest the prevalence of pericardial effusion among patients with World Health Organization (WHO) Diagnostic Group 1 PAH may be as high as 25% [Benza et al. 2010]. Pericardiocentesis or surgical pericardial window (PW) have been used for refractory, recurrent, or hemodynamically unstable pericardial effusions due to a wide range of etiologies [Becit et al. 2005]. A case series of six patients with PAH with pericardial tamponade revealed 50% mortality over a 1 year period if effusion was not drained and of two patients who received intervention for effusion with PW placement [de Perrot et al. 2012], one patient died. The management of such patients, particularly in the setting of impending or active hemodynamic instability, has not been well described in the literature. We present our single center experience of 35 patients with pulmonary hypertension (PH) and comorbid pericardial effusion, management of pericardial effusion, and long-term outcome.
Methods and materials
This was an observational study conducted at The Methodist Hospital in Houston, Texas. Institutional Review Board approval for the study was granted through Baylor College of Medicine and The Methodist Hospital, and following approval, the medical records were queried. The hospital charts of all patients admitted to The Methodist Hospital between 1 June 2005 and 1 June 2010 were searched using the International Classification of Diseases, ninth revision (ICD-9) codes for ‘pulmonary hypertension’ and ‘pericardial effusion’. Patient charts found to contain the relevant ICD-9 codes were then screened, and those patient encounters with a documented history of WHO Diagnostic Group 1, 3, 4, or 5 PH by historical right heart catheterization (RHC), echocardiogram, or both, as well as pericardial effusion demonstrated by echocardiogram or computed tomography were identified. Of the 138 patients identified with pericardial effusion, 103 with valvular heart disease, recent cardiothoracic surgery or end-stage renal disease (see Figure 1) were excluded. Thirty-five patients who met the inclusion criteria were included in this analysis.
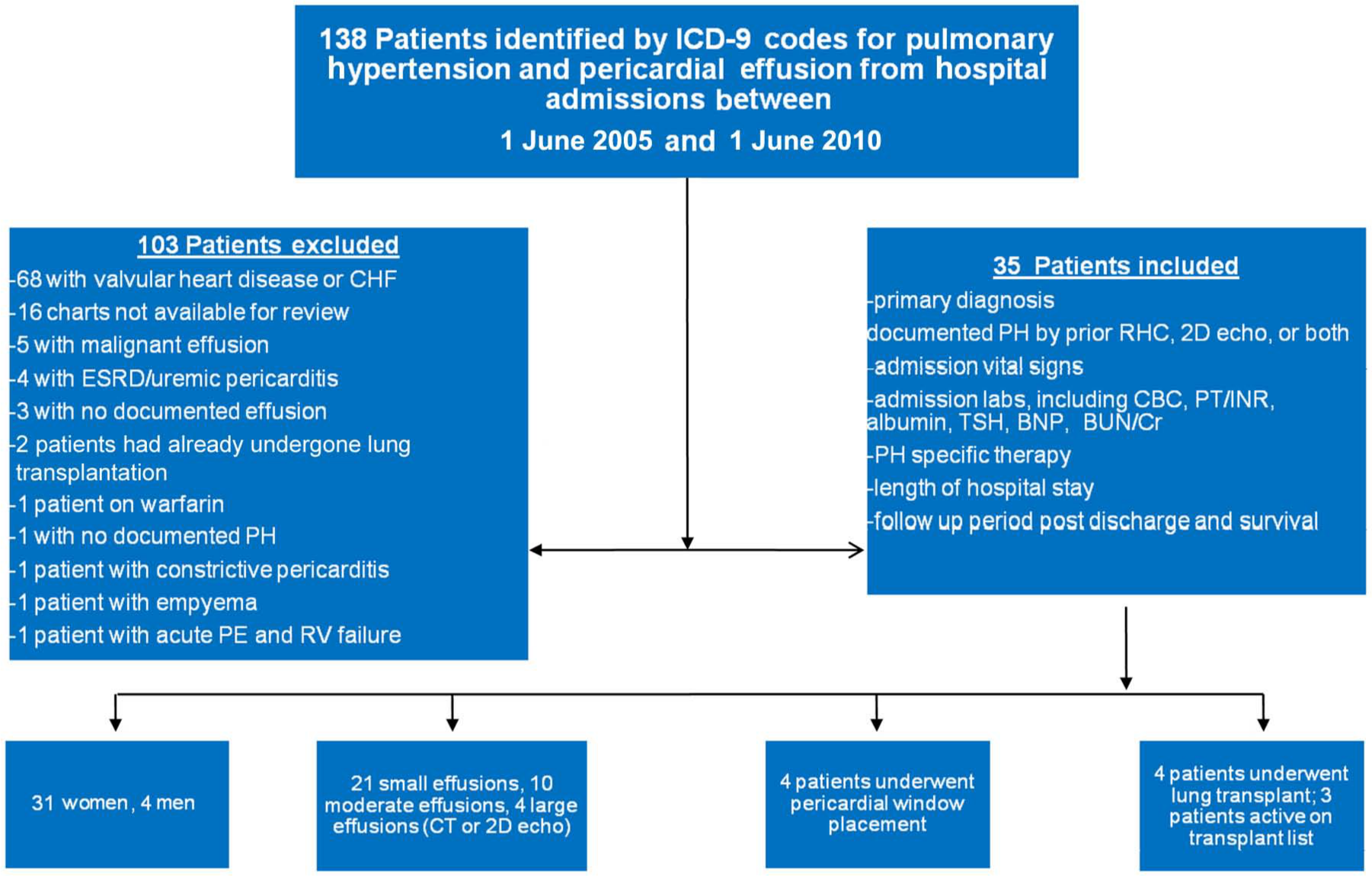
Flow diagram of patients in the study. 2D, two-dimensional; BNP, B-type natriuretic peptide; BUN, blood urea nitrogen; CBC, complete blood count; CHF, congestive heart failure; Cr, creatinine; CT, computed tomography; ESRD, end-stage renal disease; ICD-9, International Classification of Diseases, ninth revision; INR, international normalized ratio; PE, pericardial effusion; PH, pulmonary hypertension; PT, prothrombin time; RHC, right heart catheterization; RV, right ventricle; TSH, thyroid-stimulating hormone.
Patients were divided according to the size of the pericardial effusion and the presence of pericardial tamponade physiology. The baseline patient demographics that were recorded included age, follow-up time from admission, PH-specific medications at the time of admission or added during the admission, baseline laboratory values including creatinine, international normalized ratio (INR), B-type natriuretic peptide (BNP) levels, whether the patient underwent solid organ transplantation during the observation period and outcome.
For PW, the following protocol was undertaken: with the patient in the supine position, under monitored anesthesia care and local anesthesia, a longitudinal incision was made beginning just below the xiphoid process and carried down approximately 6 cm through skin, subcutaneous tissue, linea alba, and subxiphoid to the pericardium. The pericardium was placed on tension using two silk sutures in the pericardium; following that, the pericardium was pulled and opened with cautery and scissors. A segment of pericardium was removed approximately 4 cm in diameter. A Blake drain was inserted through a separate stab wound, brought through the incision and then placed in the posterior pericardium and secured in place with skin sutures and the incision was subsequently closed.
Statistical analysis
Data are presented as mean ± standard deviation. Hemodynamic parameters obtained for each pericardial effusion size group (small, moderate, large and tamponade), mean pulmonary artery pressure (by RHC), mean right atrial pressure, pulmonary artery systolic pressure (by echocardiogram), and mean arterial pressure (by blood pressure cuff) were compared using analysis of variance and baseline laboratory values for BNP, creatinine, INR, and platelet count. Logistic regression for multivariate analysis with death as an endpoint was performed for multiple covariates, including age, sex, pulmonary artery systolic pressure (as estimated by two-dimensional echocardiogram), mean right atrial pressure, mean arterial blood pressure (measured noninvasively by blood pressure cuff), BNP level on admission, INR, creatinine, and the size of pericardial effusion (small, moderate, large, or tamponade physiology). Kaplan–Meier survival curves were produced for all patients with PH and pericardial effusion, those patients with pericardial tamponade who underwent PW placement, those managed conservatively (medical management only), and those who underwent transplantation during the follow-up period. The p value was considered significant at 0.05. All statistical calculations were done using SAS software (SAS Institute, Cary, NC, USA).
Results
Demographic characteristics
The mean age of the cohort was 46.1±15.8 years, there were 31 women and four men, and the mean follow-up time from hospitalization was 22.5 ± 15.1 months (Table 1). Ten patients (28.6%) carried a diagnosis of idiopathic PAH (IPAH), 10 patients had CREST/scleroderma-related PH (28.6%), five patients had a diagnosis of systemic lupus erythematosus or other connective tissue disease associated PH (14.3%), three patients had a history of congenital heart disease related PH (8.6%), two patients had portopulmonary hypertension (5.7%), and five patients had miscellaneous etiologies (2.9% each) (Figure 2). All but one patient (34 of 35, 97.1%) were on PH-specific therapy at the time of hospitalization. The patient not on any PH-specific therapy had not been evaluated by the PH service. During admission, six patients were started on new PAH-specific therapy (two on ETRA and four on intravenous prostacyclin). The four patients who developed pericardial tamponade comprised the major represented etiologies in our cohort: two patients with IPAH and two with scleroderma/CREST-associated PH.
Patient characteristics.

ASD, autism spectrum disorder; CHD, congenital heart disease; COPD, chronic obstructive pulmonary disease; CREST, limited scleroderma (calcinosis, rayanunds, esophageal dysmotility, sclerodactyly, telangiectasia); CTD, connective tissue disease; ETRA, endothelin receptor antagonist; F, female; F/U, follow up; M, male; NSIP, nonspecific interstitial pneumonia; PAH, pulmonary arterial hypertension; PDE5-I, phosphodiesterase type 5 inhibitor; PH, pulmonary hypertension; SD, standard deviation; s/p BLTx, bilateral lung transplantation; s/p OHT/DLT, orthotopic heart and double lung transplantation; s/o OLT, orthotophic liver transplantation; VSD, ventricular septal defect.

Etiology of pulmonary hypertension in the studied population. CHD, congenital heart disease; COPD, chronic obstructive pulmonary disease; CTD, connective tissue disease; CREST, limited scleroderma (calcinosis, rayanunds, esophageal dysmotility, sclerodactyly, telangiectasia); CTEPH, chronic thromboembolic pulmonary hypertension; IPAH, idiopathic pulmonary arterial hypertension; PAH, pulmonary arterial hypertension; SLE, systemic lupus erythematosus.
Pericardial effusion size
The included patients were divided by the qualitative size of the pericardial effusion determined by echocardiography or computed tomography into small, moderate, large, or evidence of pericardial tamponade by diastolic collapse of the right atrium, right ventricle or left ventricle (Figure 3). Twenty-one patients (60%) were found to have a small pericardial effusion, nine patients with a moderate-sized pericardial effusion (25.7%), one with a large pericardial effusion but without tamponade physiology (2.8%), and four patients with pericardial tamponade (11.5%) of whom three had large pericardial effusions and one had moderate-sized effusion. PWs were done for all four patients found to have evidence of pericardial tamponade (Figure 4). Failure to respond to diuretic therapy was noted in patients undergoing PW.
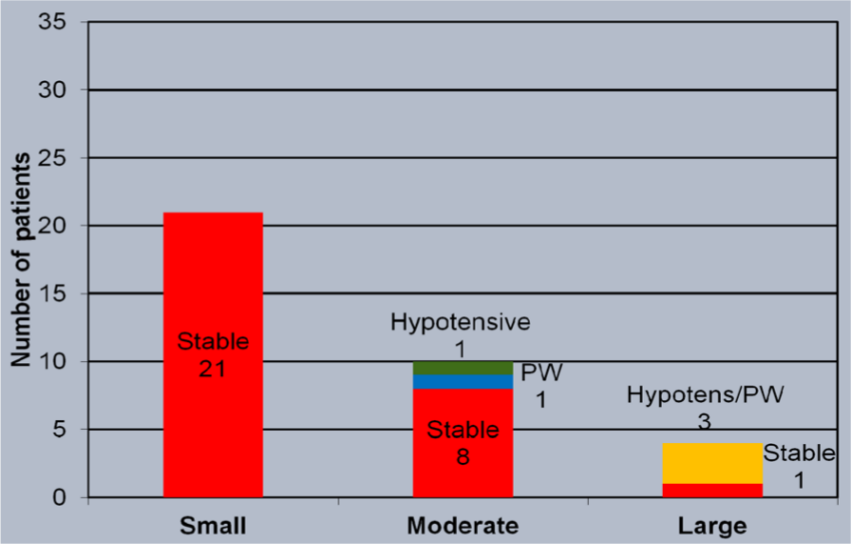
Number of patients with small, moderate and large pericardial effusions. PW, pericardial window.

Computed tomography of chest in a patient with cardiac tamponade. The patient presented with decompensated right heart failure and hypotension. The patient successfully underwent subxiphoid pericardial window for refractory pericardial effusion and unstable hemodynamics. LV, left ventricle; PE, pericardial effusion; RV, right ventricle.
Hemodynamics analysis
Hemodynamic parameters were analyzed within individual subgroups of pericardial effusion sizes. Using analysis of variance (ANOVA) methodology, there were no significant differences in the mean pulmonary artery pressure measured by RHC (p = 0.636), pulmonary artery systolic pressure by echocardiography (p = 0.636), mean right atrial pressure measured by RHC (p = 0.467), or mean arterial pressure by noninvasive blood pressure monitoring (p = 0.867) at the time of admission of any of the pericardial effusion subgroups.
Laboratory parameters
Laboratory parameters for the pericardial effusion subgroups were likewise compared using ANOVA analysis (Table 2). There were no significant differences in the BNP (p = 0.773), INR (p = 0.847), platelets (p = 0.813), and creatinine (p = 0.926) for any of the pericardial effusion subgroups.
Laboratory values for the studied population.

INR, international normalized ratio; ND, not done.
Outcome analysis
Logistic regression with death as an endpoint was performed for multiple variables. There were no significant associations found between an increased risk of death and patient age [odds ratio (OR) 1.04, 95% confidence interval (CI) 0.93–1.16, p = 0.531], patient sex (male versus female, OR 0.28, 95% CI 0.01–14.76, p = 0.526), mean pulmonary artery systolic pressure, mean right atrial pressure, mean arterial pressure, BNP, creatinine, INR, size of pericardial effusion (OR 5.77, 95% CI 0.22–156.62, p = 0.294), or the placement of a PW (OR 0.01, 95% CI <0.001–50.31, p = 0.296).
At the conclusion of the observation period, 21 of 35 patients (60%) were alive, with 12 patients deceased (34.3%), and two patients lost to follow up (5.7%) (mean follow-up period 22.5 ± 15.1 months). Four patients underwent solid organ transplantation (11.4%), three heart/double lung transplantations and one orthotopic liver transplantation, and all four survived to the conclusion of the observation period (mean follow-up post transplant 21.3 ± 15.5 months). Of the four patients who had a PW placed for tamponade physiology, three survived to the end of the observation period (75%) and one died (Figure 5). One of them was started on epoprostenol and two patients had the doses of intravenous prostacyclin uptitrated. Two patients who had PW placed for hemodynamically significant effusions were active on the list for heart/double lung transplantation (mean follow up 29.5 ± 4.9 months). None of the patients who ultimately went on to solid organ transplantation during the observation period had a PW placed.

Five-year Kaplan–Meier plot of mortality in patients with pulmonary hypertension in different treatment groups. Patients who were transplanted did not have a significant survival advantage compared with the other subgroups, although this study may be underpowered to detect this difference. PW, pericardial window.
Discussion
Evidence that the presence of pericardial effusion is an independent mortality risk factor in the setting of PAH [Benza et al. 2010] presents a challenge to clinicians in the management of this subset of the PH cohort. In our patient population, we did not demonstrate a correlation between mortality and the size of pericardial effusion or tamponade, or between multiple covariates, including hemodynamics and demographic characteristics and increased risk of patient death. These findings may be reflective of small sample size, although they suggest that the size of pericardial effusion is less important from a standpoint of prognosis than is the presence or absence of effusion. In the special case of pericardial tamponade complicating pericardial effusion, we did not show any mortality or survival benefit between the nonoperative pharmacologic management of patients with PH with pericardial effusion and the surgical creation of a PW.
The accurate assessment of the mortality benefit in this subgroup of patients is difficult retrospectively for at least two reasons. First, the standard of care for treatment of patients with pericardial tamponade and impending hemodynamic collapse has been pericardial drainage [Becit et al. 2005; Campo et al. 2010; Dunne et al. 2011; Hemnes et al. 2008] either percutaneously by pericardiocentesis or by surgical decompression. Previously reported data by Hemnes and colleagues suggested that the 1-year mortality of patients with PH with hemodynamically significant pericardial effusion in the absence of intervention was 50%, and that the perioperative mortality associated with operative intervention in their patient population was also 50% (one of two patients died) [Hemnes et al. 2008]. The mechanisms responsible for this high mortality post drainage of effusion in the PH cohort are not well understood. It is also not known whether the high mortality rates associated with pericardial effusion in PH are directly related to the effusion, or are a surrogate for deteriorating hemodynamics or another, as of yet, undiscovered risk factor. Second, in our cohort, additional interventions were performed at the time of PW placement, including the initiation or titration of PH-specific medications perioperatively. As this is a retrospective study, we cannot accurately define hemodynamic instability; however, patients were assessed to have pericardial tamponade by the treating physician at the time of the care. This would take into account hemodynamic stability, failure to respond to diuretics and addition of PH therapy. The effect of optimization of PH-specific pharmacotherapy in combination with PW placement cannot be defined with these data.
The significant limitation of the available data is small sample size, which may affect determinations of statistically significant differences between subgroups, as well as the retrospective nature of the study design. As 16 patients were excluded due to unavailability of their charts, it is difficult to say what the results would have been if those charts were available. However, we believe that our results and conclusions would have remained unchanged. In addition, of the patients who survived to undergo solid organ transplantation, none had pericardial tamponade, although two of the four patients with tamponade who survived to the conclusion of the observation period were active on the solid organ transplantation list.
As previously discussed, there was no statistically significant difference between conservative management and surgical drainage of pericardial effusion in the PH cohort. In addition, there was no statistically significant difference for PW placement versus transplantation, although there may have been a trend towards a survival benefit of transplantation.
The central question to be addressed in future investigations is what, if anything, can be done to mitigate the dismal mortality statistics for this subset of patients with PH. Lung transplantation has been shown to improve survival in patients with PH with New York Heart Association/WHO functional class III–IV symptoms and deteriorating clinical status despite medical therapy [de Perrot et al. 2012; Lordan and Corris, 2011; Mendeloff et al. 2002]. Nevertheless, there has been criticism of the Lung Allocation Score (LAS) used by the United Network for Organ Sharing for prioritizing organ transplant recipients in placing patients with PH at a relative disadvantage compared with other advanced lung disease categories [United Network for Organ Sharing, 2012].
The current LAS algorithm does not take into account the presence of pericardial effusion as a harbinger of poor prognosis in PH. Further studies on patient outcomes would be helpful in clarifying the possibility of adding pericardial effusion to the LAS as a surrogate for mortality risk in patients with PH.
More data is required to define the role of medical and surgical interventions in the management of patients with PH with pericardial effusion, although lung transplantation remains an option in patients with end-stage PH.
Conclusion
Patients with PH complicated by pericardial effusion currently carry a poor prognosis, and limited data exist to support management options in this complex clinical scenario. The standard of care for hemodynamically unstable pericardial effusion has historically been catheter or surgical decompression, although it is unclear from the available information whether this approach is beneficial in the setting of PH-associated effusions. The pathophysiology of hemodynamic decompensation in patients with PH after pericardiocentesis or PW placement is not well understood. In addition, the size of pericardial effusion may be less important in this patient population than the presence of effusion. Further studies with larger patient cohort will be needed to clarify the proper evaluation and risk stratification of patients with PH with pericardial effusion, and which interventions, if any, can be used to alter their clinical outcomes.
Footnotes
Acknowledgements
The authors appreciate the editorial help of Ms Janice Brister in the preparation of this manuscript.
Funding
This study was supported by the National Institute of Health (grant number K23 HL-093214) to ZS.
Conflict of interest statement
Zeenat Safdar is on the scientific advisory board and speakers bureau for Gilead Sciences, Actelion Pharmaceuticals and United Therapeutics.