
Abstract
Primary responses in sepsis-mediated inflammation are regulated by pro-inflammatory cytokines. Variations in the cytokine genes might modify their transcription or expression, plasma cytokines levels and response to sepsis. Activation protein-1 (AP-1) and NF-κB regulate cytokines gene expression in sepsis. A total of 90 severely septic and 91 non-infected patients were prospectively studied. IL-1α (–889 C/T), IL-1β (+3954 C/T), IL-6 (–174 G/C), TNF-α (–238 G/A), TNF-α (–308G/A), IL-8 (–251A/T) and IL-10 (–1082 G/A) SNPs, plasma IL-1β, IL-4, IL-6, IL-8, IL-10, IL-13, IFN-γ, TNF-α and monocyte chemoattractant protein 1 (MCP-1) levels, and AP-1 and NF-κB gene expression by neutrophils were assessed. A allele carriers of TNF-α (–238 G/A) SNP were less frequent among septic patients. IL-6, IL-8, IL-10, TNF-α and MCP-1 levels were higher, and AP-1 and NF-κB gene expressions lower in septic patients. Sepsis was independently associated with higher fibrinogen, neutrophils counts and IL-8 levels, lower prothrombin, absence of the variant A allele of the TNF-α (–238 G/A) SNP, and haemodynamic failure. Death was independently associated with a higher APACHE II score, higher IL-8 levels, and the diagnosis of sepsis. TNF-a (–238 G/A) SNP could protect against sepsis development. Higher IL-8 levels are predictive of sepsis and mortality.
Introduction
Septic shock is the most common cause of death in intensive care units (ICU). Despite modern intensive care and antibiotic treatments, the mortality of sepsis still remains high, ranging from 20% to 30% in septic shock.
Primary responses in sepsis-mediated inflammation are regulated by pro-inflammatory cytokines, initially by the primary cytokines TNF-α and IL-1 and later by secondary pro-and anti-inflammatory mediators such as IL-6 and IL-10, respectively. Many cytokines display variations in their gene promoter regions. Polymorphisms in this promoter area might modify their transcription or expression, plasma cytokines levels and response to sepsis although results are controversial.1–19 Promoters contain cis-acting elements that represent short sequence motifs specific for binding of DNA-binding proteins nuclear factors such as the activation protein-1 (AP-1) and NF-κB. Both nuclear factors regulate cytokines gene expression in response to sepsis.1–3 Previous studies have shown some associations of TNF-α (–308 G/A), TNF-α (–238 G/A), IL-1α (–889 C/T), IL-1β (+3954 C/T), IL-1 RN VNTR L/2 and the IL-6(–174G/C) SNPs with sepsis, although the results are far from clear due to the relatively small size and the diverse ethnic origin of the populations studied and the different type of controls used.5–20
The aims of this study were to investigate whether different cytokines genes SNPs might associate with susceptibility to sepsis or influence the sepsis outcome with/without associated changes in plasma cytokines levels. In order to answer these questions, plasma levels of IL-1β, IL-6, IL-8, IL-10 and TNF-α as well as those of monocyte chemoattractant protein 1 (MCP-1) were measured and different cytokine SNPs: IL-1α (–889 C/T), IL-1β (+3954 C/T), IL-6 (–174 G/C), TNF-α (–238 G/A), TNF-α (–308G/A), IL-8 (–251A/T) and IL-10 (–1082 G/A) were genotyped in septic and uninfected ICU control patients. AP-1 and NF-κB gene expression by peripheral neutrophils was also assessed. Because cytokines plasma levels might change during sepsis development, the time course of plasma cytokines was also analysed in a subgroup of septic and uninfected ICU control patients.
Patients and methods
Patients
A total of 90 patients with severe sepsis admitted to the ICU of the Hospital Universitario Central de Asturias (HUCA) in Oviedo, Spain, were enrolled in the study. Patients were included as septic if they fulfilled the diagnosis of severe sepsis according to the 1992 International Sepsis Definitions Conference Criteria modified in 2003 and 2016 (Sepsis-3).21–23 In addition, all septic patients had positive blood cultures or a microbiologically demonstrated source of bacterial infection at ICU admission. All the infections were community-acquired. Patients with cancer, HIV infection, transplantation or other causes of immunodepression were excluded. A total of 91 uninfected patients admitted consecutively to the ICU for other non-infective diseases, mostly with severe polytrauma and cerebro-vascular attacks (CVA), were used as controls. APACHE II scores and number of organs that failed were calculated in septic patients and uninfected controls. Patients and controls were members of a homogeneous Caucasian population, and were residents of the same region (Asturias, Northern Spain), which has a small foreign immigrant population (less than 5%). Each participant or their legal representatives gave informed consent for the study, which was approved by the Ethics Committee of the HUCA. Haemodynamic and other organ dysfunction failures were defined according to Marshall. 24 Treatment of organ failures, volume resuscitation and supportive therapy for sepsis were based on currently applied guidelines. 25
Plasma cytokines
Blood (10 ml) was drawn by venipuncture in EDTA-containing tubes within the first 24 h of ICU admission in all the study individuals, and in a subgroup of 14 sepsis patients and 15 controls, chosen at random; samples were also obtained at d 1, 3 and 7 of ICU stay. Tubes were centrifuged for 5 min at 1800 g and serum was removed and frozen at –80°C until use. Plasma levels of IL-1β, IL-4, IL-6, IL-8, IL-10, IL-13, TNF-α, IFN-γ and MCP-1 were measured using the QuAb® Human Cytokine Array 1 from Raybiotech (Raybiotech, Parkway Lane, Norcross, GA, USA) according to the manufacturer’s instructions.
Cytokine SNP genotyping and linkage disequilibrium analysis
DNA was obtained from peripheral blood cells and stored at –20°C before use. The following SNPs of cytokines were genotyped by PCR: IL-1α (–889 C/T, rs1800587), IL-1β (+3954 C/T, rs1143634), IL-6 (–174 G/C, rs1800795), TNF-α (–238 G/A, rs361525), TNF-α (–308 G/A, rs1800629), IL-8 (–251 A/T, rs4073) and IL-10 (–1082G/A, rs1800896). Oligonucleotide primer sequences, PCR conditions and restriction enzymes used for genotyping and sequencing the different cytokines polymorphisms studied are described elsewhere. 26
After genotyping the previous SNPs of cytokines, a linkage disequilibrium (LD) analysis of TNF-α (–238 G/A, rs361525) and TNF-α (–308 G/A, rs1800629) was performed. Both SNPs are located adjacent in the genome, inside the promoter region of the TNF-α gene in the chromosome 6. LD is a population-based parameter that describes the degree to which an allele of one genetic variant is inherited or correlated with an allele of a nearby genetic variant within a given population.
Other laboratory analysis
A complete haemogram, coagulation and general biochemistry were obtained from patients and controls at d 1 of ICU admission.
Neutrophil isolation
Peripheral blood (10 ml) was drawn from each patient and control in an EDTA-K3E tube (Vacuette, Greiner Bio-One, Kremsmuenster, Austria) and neutrophils were separated with Ficoll-Hypaque (δ = 1.113) (Lymphoprep™, Axis-Shield Poc AS, Oslo, Norway) following the manufacturer’s instructions. Cells were re-suspended in HAM’S F-12 medium (GIBCO, Paisley, UK) and counted using with a Cell-Dyn® 3200 Coulter (Abbott Laboratories, Abbott Park, IL, USA). Neutrophil purity was always > 98%.
Neutrophil mRNA extraction and AP-1 and NF-κB expression analysis
Total RNA from the isolated neutrophils was extracted using the E.Z.N.A. Total RNA Kit (Omega Bio-Tek, Inc., Norcross, GA, USA) according to the manufacturer’s instructions. The quantity of total RNA extracted was measured using spectrophotometry at 260 nm. The RNA was then reverse-transcribed to cDNA using the High Capacity cDNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s protocol. Gene transcription levels of AP-1 and NF-κB were then analysed by quantitative real-time PCR (qRT-PCR) using the TaqMan Gene Expression Assays on a 7300 RealTime PCR System using the 7300 System SDS Software Version 1.4 (all from Applied Biosystems). GAPDH was the housekeeping gene used as endogenous control for calibration of mRNA levels. All primers and probes (AP-1 (c- Jun], cat. no. Hs01103582_s1; NF-κB cat. no. Hs00765730_m1, GAPDH, cat. no. Hs03929097_g1) were obtained commercially and are proprietary; thus, their sequences are not available (TaqMan Gene Expression Assays from Applied Biosystems). The conditions for the qRT-PCR were as follows: preheating at 50°C for 2 min and at 95°C for 10 min, followed by 40 cycles of shuttle heating at 95°C for 15 s and at 60°C for 1 min. All the RT-PCR reactions were performed in triplicate. The data analysis of the gene expression levels was performed on ΔΔCt values normalized to GAPDH expression as previously described and results were expressed as log10Qr. 27
Statistical analysis
Results are expressed as median and inter-quartile range (IQR), or proportions as appropriate. Correlations between the cytokine values and other continuous variables were assessed with the Spearman’s test. The Pearson χ2 test was used to compare allele and genotype frequencies and the clinical characteristics between the groups. Fisher’s exact test and the Yates correction were used when indicated. Mann–Whitney U test was used to compare continuous variables between two groups and the Kruskal–Wallis test for comparing more than two groups. The Wilcoxon signed rank test was used to evaluate the cytokine changes over time of each patient compared with himself/herself and a repeated measures general linear model procedure was carried out to evaluate the course of cytokines over time in septic versus control patients. A multivariate stepwise logistic regression analysis was also done to assess the factors associated independently with sepsis and death. Statistical analysis was performed with the SPSS Statistical Software package (version 25.0, IBM Corp., Armonk, NY, USA). All reported P values are two-sided. A P value < 0.05 was considered statistically significant. LD analysis was measured by the two most commonly used statistics, D′ and r2, for an easy comparison of cases and controls. LD was estimated using the R Statistical Software. (The R Project for Stastistical Computing; https://www.r-project.org/). In a disease association context, the r2 statistic is often used in calculations of power to detect disease-susceptibility loci. Under some conditions, the power to detect disease association with a marker locus when using a case-control sample of size N is approximately equal to the power to detect disease association with the true causal locus when using a sample of size Nr 2 , where r2 here denotes the value of the r2 statistic for the marker locus and the causal locus.
Results
Patients clinical and standard laboratory characteristics and outcome
Table 1 shows the demographic, clinical and standard laboratory characteristics and Table 2 shows the plasma cytokine levels and AP-1 and NF-κB neutrophils expression of both groups. Table 3 compares the demographic, clinical, laboratory and genotypic features in survivors and non-survivors.
Demographic and clinical characteristics and standard laboratory measures of ICU septic and uninfected patients.
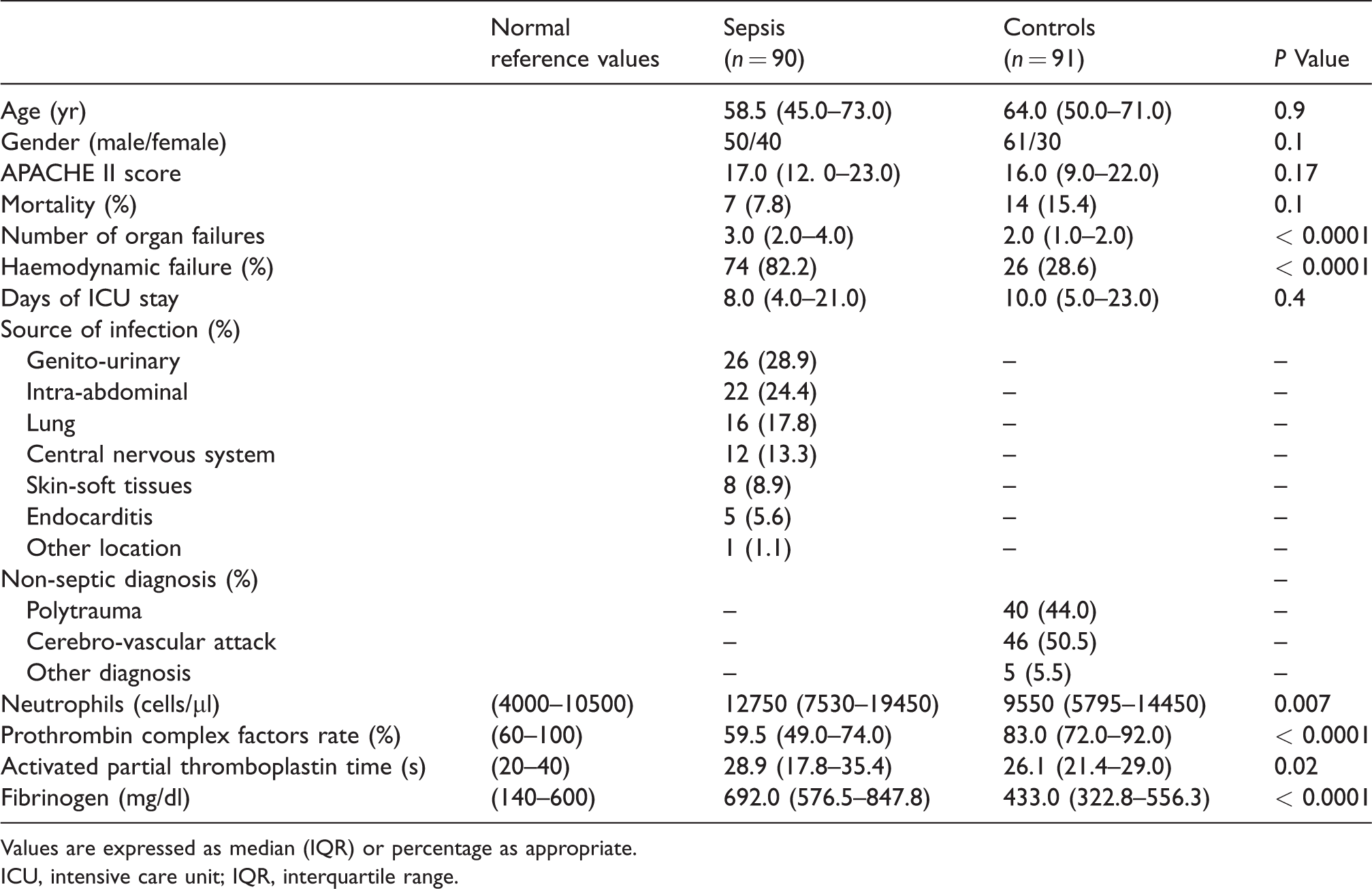
Values are expressed as median (IQR) or percentage as appropriate.
ICU, intensive care unit; IQR, interquartile range.
Plasma cytokines and neutrophils activating transcription factor expression data of ICU septic and uninfected patients.
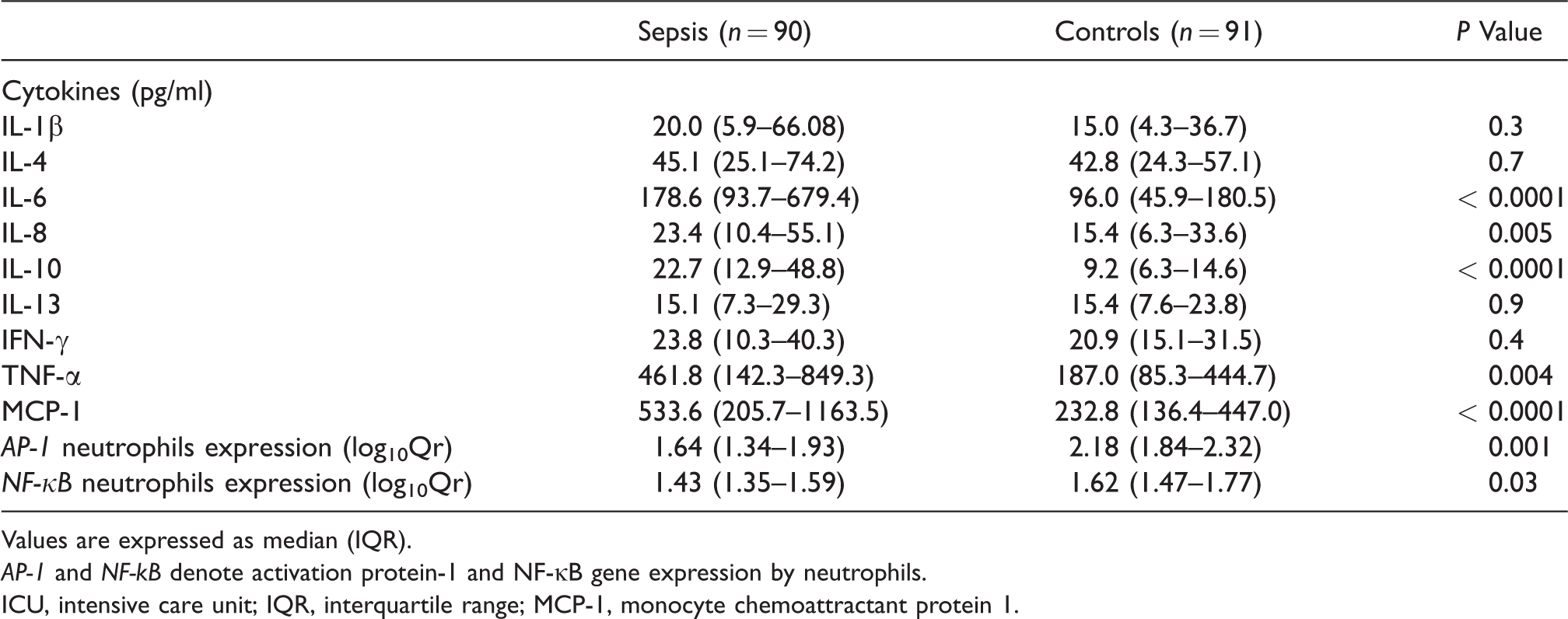
Values are expressed as median (IQR).
AP-1 and NF-kB denote activation protein-1 and NF-κB gene expression by neutrophils.
ICU, intensive care unit; IQR, interquartile range; MCP-1, monocyte chemoattractant protein 1.
Demography, clinical, laboratory and genotypic features in survivors and non-survivors.
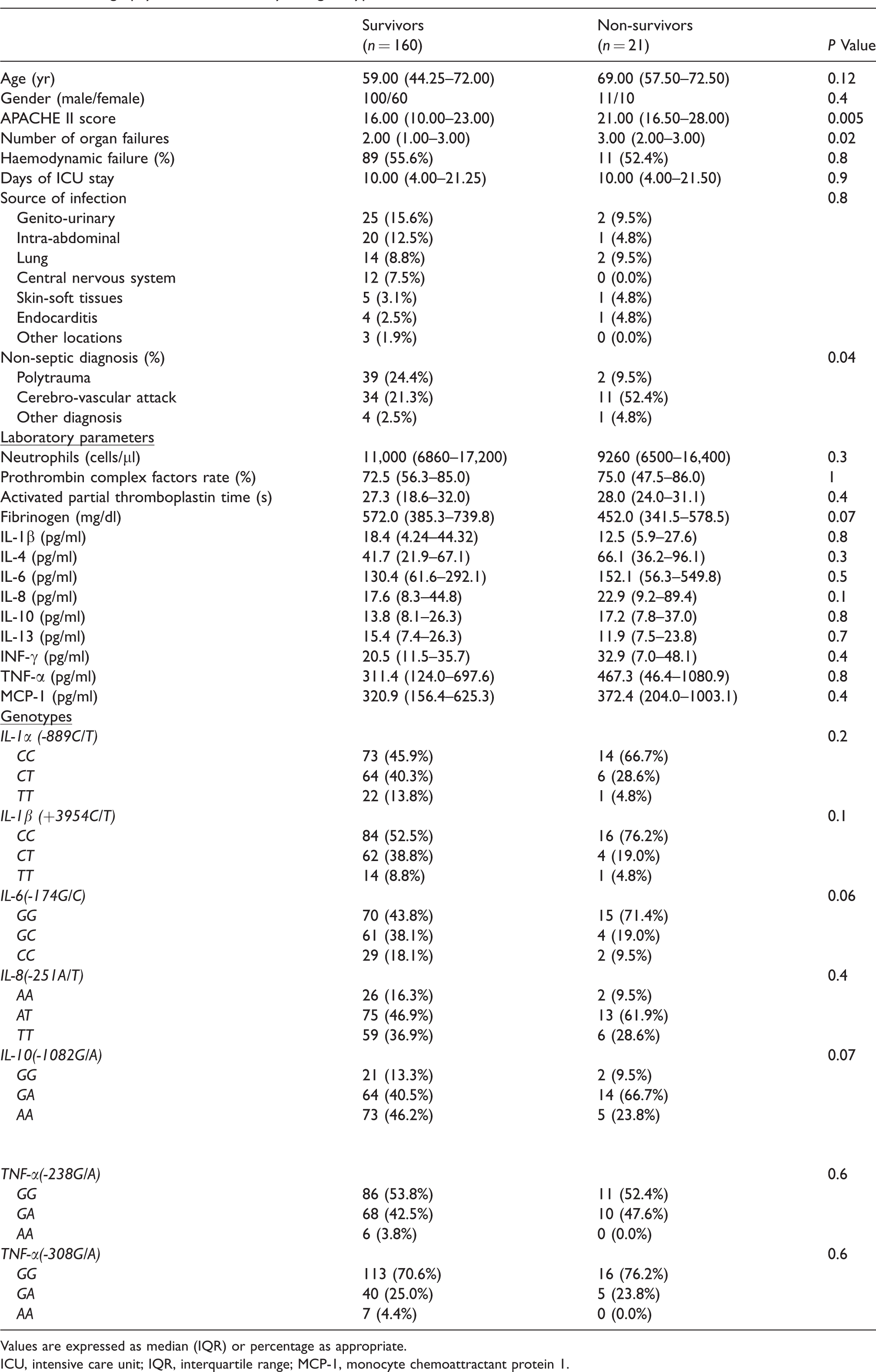
Values are expressed as median (IQR) or percentage as appropriate.
ICU, intensive care unit; IQR, interquartile range; MCP-1, monocyte chemoattractant protein 1.
Septic and uninfected ICU patients were matched in age and sex. There were no differences in APACHE II score. A total of 21 individuals died (11.6%). Although more uninfected controls died, there were no statistically significant differences compared with the septic patients. As expected, the number of organs that failed was significantly higher in septic patients. In addition, the APACHE II score and the number of organ failures were significantly higher in non-survivors (21 patients) compared with survivors (160 patients) (Table 3). Positive blood cultures were obtained in 75 (83.3%) of septic patients; 40 (53.3%) of them grew Gram-negative bacteria, mostly Escherichia coli (18 patients, 24%) and 35 (46.7%) grew Gram-positive bacteria, mostly Streptococcus pneumoniae (16 patients, 21.3%). The main sources of infection were urinary, intra-abdominal and respiratory. The uninfected control group was composed of ICU patients admitted mainly because of polytrauma and CVA problems.
Plasma cytokine levels and AP-1 and NF-κB neutrophil expression in septic and uninfected controls
We observed significantly higher levels of neutrophils, activated partial thromboplastin time, fibrinogen and plasma IL-6, IL-8, IL-10, TNF-α and MCP-1 in septic patients compared with uninfected controls at d 1 of ICU admission. Prothrombin complex factor rate was decreased in septic compared with uninfected ICU controls. In the septic group, patients who died had significantly higher levels of IL-8 and IL-10 than those who survived (69.3 pg/ml (23.7–938.4) versus 21.4 (10.1–50.3), P = 0.03; and 52.5 pg/ml (33.9–536.4) versus 21.9 (12.8–42.3), P = 0.04, respectively]. Non-survivors had also higher levels than survivors regarding other cytokines, such as IL-4, IL-6, IFN-γ, TNF-α and MCP-1, although the differences did not reach the significance level, probably because of the small number of patients who died. There were no significant differences in the cytokine levels of septic patients according to the etiology of the sepsis (Gram-positive versus Gram-negative organisms) or the primary site of infection (data not shown). Similarly, there were no differences in the control patients according to the diagnosis, with exception of IFN-γ, which was higher in polytrauma than in CVA patients (26.5 pg/ml (17.2–35.0) versus 18.2 (9.0–25.3), respectively, P = 0.026). AP-1 and NF-κB gene expressions by the neutrophils were significantly decreased in septic compared with uninfected ICU controls (Table 2)
Cytokine SNPs and plasma cytokine values
Table 4 shows the genotypic and allelic frequencies of different cytokine SNPs in septic and control patients.
Genotypic and allelic frequencies of different cytokine SNPs in ICU septic patients and uninfected controls, and their association with circulating plasma cytokines.
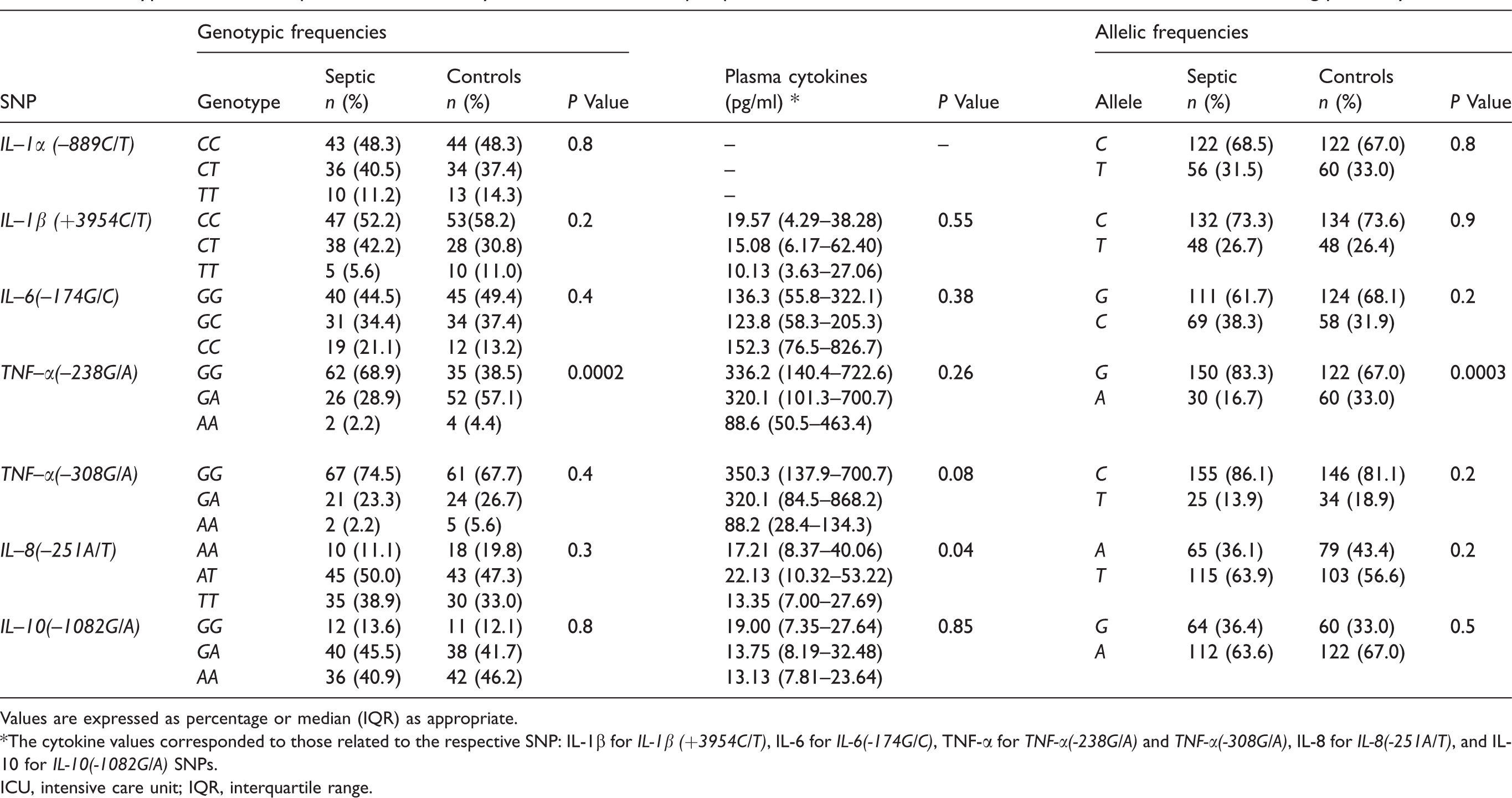
Values are expressed as percentage or median (IQR) as appropriate.
*The cytokine values corresponded to those related to the respective SNP: IL-1β for IL-1β (+3954C/T), IL-6 for IL-6(-174G/C), TNF-α for TNF-α(-238G/A) and TNF-α(-308G/A), IL-8 for IL-8(-251A/T), and IL-10 for IL-10(-1082G/A) SNPs.
ICU, intensive care unit; IQR, interquartile range.
Of all the cytokine SNPs studied, we found that only the variant GA and AA genotypes of the TNF-α (–238 G/A) SNP and the variant A allele of the same SNP were significantly less frequent in septic patients compared with uninfected ICU controls. When we compared the frequency of genotypes of the TNF-α (–238 G/A) SNP among polytrauma and CVA uninfected ICU controls, no differences were observed (P = 0.4). No differences regarding cytokine SNPs genotypic frequencies when comparing Gram-positive and -negative septic patients were observed (P = 0.3). No differences regarding cytokine SNPs genotypic frequencies when comparing survivors (160 patients) versus non survivors (21 patients) were observed either (Table 3).
The diverse cytokine SNPs were not associated with different concentrations of their respective cytokines in the patients as a whole (P = 0.08 to 0.8), except for the IL-8 (-251 A/T) SNP, which was related to different levels of IL-8 (genotype TT 13.4 pg/ml (7.0–27.7), AA 17.2 pg/ml (8.4–40.1), AT 22.1 pg/ml (10.3–53.2), P = 0.04). Table 5 shows the correlations of the diverse cytokines themselves and with other parameters.
Correlations of the diverse plasma cytokines in sepsis.
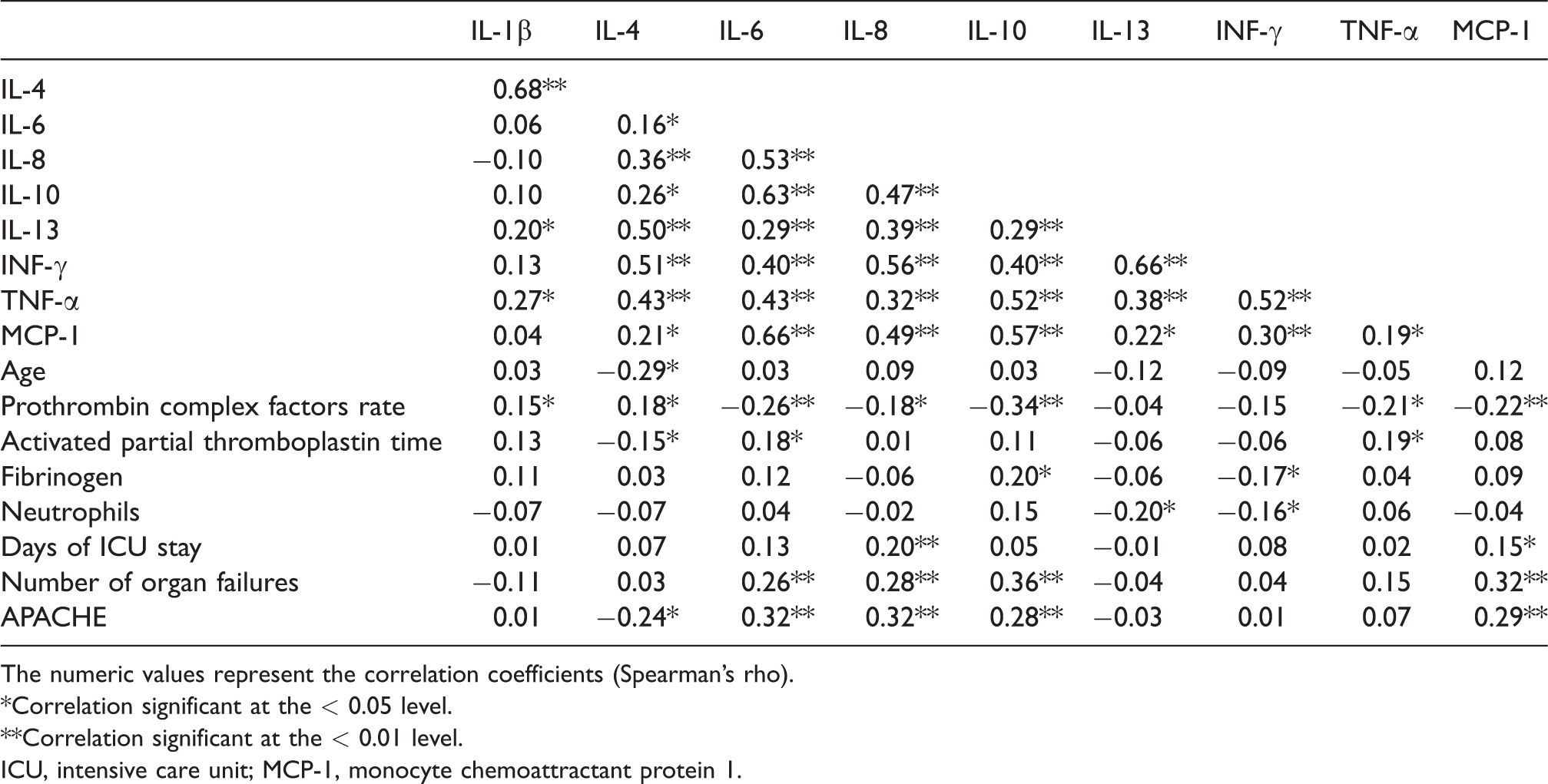
The numeric values represent the correlation coefficients (Spearman's rho).
*Correlation significant at the < 0.05 level.
**Correlation significant at the < 0.01 level.
ICU, intensive care unit; MCP-1, monocyte chemoattractant protein 1.
The number of organs that failed correlated with plasma levels of IL-6, IL-8, IL-10 and MCP-1, while the APACHE II score correlated with plasma levels of IL-6, IL-8, IL-10 and MCP-1 and negatively with plasma levels of IL-4. Similarly, most cytokines correlated among themselves, frequently with correlation coefficients higher than 0.5. No differences in the AP-1 or NF-kB gene expression by the neutrophils among carriers of the different genotypes of the cytokine SNPs studied here were observed (data not shown).
LD analysis
Estimates of LD based on D′ and r2 were different for cases and controls. For cases we observed these values: D′ = 0.9503 and r2 = 0.8534. With these values, we can say that the two SNPs, TNF-α (–238 G/A, rs361525) and TNF-α (–308 G/A, rs1800629), are in strong LD. However, for controls we obtained the following values: D′ = 0.5138 and r2 = 0.1727. The r2 = 0.1727 is low and suggest that these SNPs are not in high LD, indicating weak correlation between SNPs.
Plasma cytokine timecourse according to diagnosis
The course of cytokines over time was evaluated in a subgroup of 14 sepsis and 15 control patients, who underwent measurements at d 1, 3 and 7 of ICU admission. Among the septic patients, only IL-10 showed a statistically significant decrease between the d 1 and 7 measurements (P = 0.008), whereas the remaining cytokines did not experience significant changes (IL-1β, P = 0.9; IL-4, P = 0.6; IL-6, P = 0.1; IL-8, P = 0.18; IL-13, P = 0.3; IFN-γ P = 0.3; TNF-α, P = 0.9). No significant changes in the cytokines levels over time were observed in the control group (P = 0.1–0.9).
Regarding the comparison between the two groups, the slopes of the IL-10 and TNF-α curves over time were different between septic and control patients (P = 0.007 and P = 0.02, respectively), due mainly to a decrease of IL-10 in septic and of TNF-α in control patients. The slopes of the remainder cytokines did not differ significantly between septic and controls (P = 0.09–0.80).
Multivariate analysis
Variables with a P value < 0.1 in the univariate comparisons were used in the logistic regression analysis. Sepsis was associated independently with the following variables at the first day of ICU admission: higher fibrinogen, neutrophils count and IL-8 plasma levels, lower prothrombin complex factors rate, presence of haemodynamic failure, and absence of the variant A allele of the TNF-α (–238 G/A) SNP. Death was associated independently with a higher APACHE II score, higher plasma levels of IL-8 and diagnosis of sepsis in the multivariate regression analysis (Table 6).
Variables independently associated with sepsis and death.
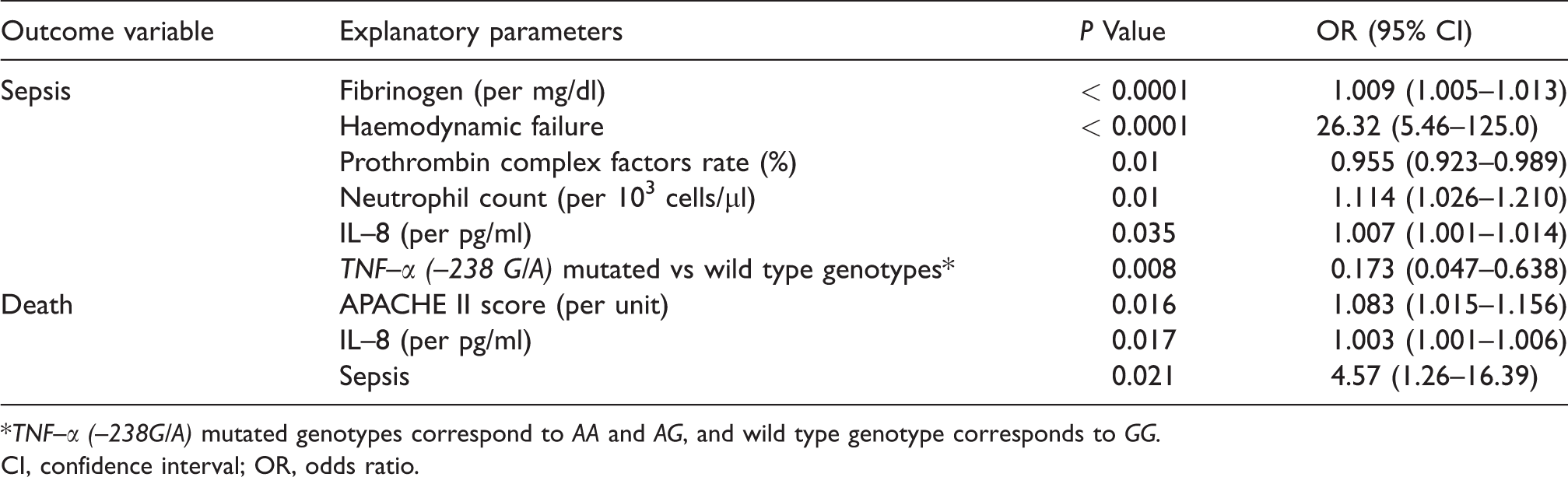
*TNF–α (–238G/A) mutated genotypes correspond to AA and AG, and wild type genotype corresponds to GG.
CI, confidence interval; OR, odds ratio.
Discussion
We report for the first time an association of the TNF-α (–238 G/A) SNP with protection against the development of severe sepsis. The carriage of the variant A allele of this TNF-α SNP was less frequent among septic patients than in uninfected ICU controls. However, no associations of this TNF-α SNP with mortality, APACHE II score, number of organs that failed, etiology of the sepsis, primary site of infection or plasma cytokine levels were observed. The uninfected controls were consecutive ICU patients with polytrauma (44%) and CVA (66%) with no differences in their genotypes for the TNF-α (–238 G/A) SNP.
Some attention has been paid so far to the role played by the TNF-α (–238 G/A) SNP in infections in general, and in sepsis in particular, with contradictory results.1–3, 6 , 14 , 15 , 18 , 28 Pappachan et al. found that the frequency of the A allele of the TNF-α (–238 G/A) SNP was significantly higher in ICU septic patients who died compared with those who survived but in association with other lymphotoxin-alpha (LTA, +252 A/G) and TNF-α (–308 G/A; -1031T/C) SNPs haplotypes. 28 TNF-α (–238 G/A) along with TNF-α (–308 G/A), (–376 G/A, rs 1800750) and (+489 G/A) SNPs have been associated with the development of severe sepsis and septic shock in Hindu patients. 18 An association of the TNF-α (–308 G/A) but not of the (–238 G/A) SNP with septic shock in Caucasian French patients was observed. 6 Very recently an association of TNF-α (–308 G/A) and NOS3 (–786 T/C, rs 2070744) SNPs with sepsis in Turkish patients was also reported. 19 TNF-α (–238 G/A) G allele, but not the A allele, along with other alleles of different SNPs of TNF-α (–308 G/A, –527C/T, –455A/G, –245C/T, –424G/A), constituted a protective haplotype (h1) against sepsis progression in Greek patients in a recent work. 14 TNF-α and LTA are neighbouring genes that are in high LD with each other. 29 TNF-α (–238 G/A) along with TNF-α (–308 G/A) SNPs are also in strong LD, as we also observed in our septic patients. Therefore, it is difficult to elucidate the individual effect of the TNF-α (–238 G/A) SNP on sepsis susceptibility from previous studies. No association of the TNF-α (–308 G/A) or (–238 G/A) SNPs and sepsis susceptibility were found in Caucasian Romanian patients in other recent study. 15 An association between TNF-α (–238 G/A) SNP and tuberculosis susceptibility by meta-analysis was also ruled out. 30 TNF-α (–238 G/A) SNP has been associated with severe malaria parasitemia in African populations.31–33 It has been suggested that the TNF-α (–238 G/A) SNP might enhance malaria by altering the existent balance between the anti-inflammatory cytokine IL-10 and the pro-inflammatory cytokine TNF-α. 31
Direct functional studies provided contrasting results on the effect of the variant A allele of the TNF-α (–238 G/A) SNP on the TNF-α gene promoter activity.34–36 Thus, replacing 10 bp covering the TNF-238 region with an irrelevant sequence increased basal transcription. 37 In addition, it has been suggested that the TNF-238 region contains a repressor site and a TNF-α promoter SNP might modify its activity. 38 An association of the TNF-α (–238 G/A) SNP with changes in the TNF-α plasma levels enhanced by sepsis is a very attractive hypothesis although with contradictory results reported so far. 6 , 15 , 39 , 40 Georgescu et al. observed increased TNF-α plasma levels in Romanian patients with septic shock carriers of the G allele of the TNF-α (–238 G/A) SNP. 15 However, Mira et al. reported that the TNF-α (–308 G/A) SNP association with septic shock was independent of TNF-α plasma levels in TNF-α SNP carriers. 6 Our data agree with the observations of Mira et al. We did not find either differences in plasma levels of TNF-α or other cytokines in carriers of the different genotypes of the TNF-α (–238 G/A) SNP or other cytokines SNPs except for the IL-8 (–251A/T) SNP.
Changes in DNA-binding proteins nuclear factors expression might be other reasonable hypothesis to explain the protective effect of the TNF-α (–238 G/A) SNP on sepsis considering that AP-1 and NF-κB might regulate cytokine gene expression in response to severe infection. Although AP-1 and NF-κB gene expression by neutrophils were significantly decreased in septic patients compared with uninfected ICU controls, no differences regarding AP-1 and NF-κB gene expression among carriers of the different genotypes of the TNF-α (–238 G/A) SNP or other cytokines SNPs were found. Therefore, the mechanism of the protective effect of this TNF-α SNP on sepsis remains elusive. It might be that the TNF-α (–238 G/A) A allele serves as a marker for a functional SNP elsewhere in the TNF gene or in another nearby immunologically relevant gene, as suggested by Zhang et al. 30 TNF-α (–238 G/A) SNP is in LD with HLA-A1, –B8 and –DR3 alleles, and HLA-A1 has been associated with tuberculosis response and might modify sepsis response as well. 41 , 42 Very recently, our group was found that the A variant allele of the TNF-α (–308 G/A) SNP, in strong LD with the TNF-α (–238 G/A) SNP, was significantly less frequent in patients with infected orthopaedic prosthesis compared with patients with implanted prosthesis that did not develop infection after 12 yr of follow up (unpublished observation). This recent observation reinforces the idea of a protective role against infection played by the A variant allele of the TNF-a (–238 G/A) SNP. This is the main novelty brought forward by the present sepsis study, and needs further studies for confirmation.
We have no clear explanation for the decreased AP-1 and NF-κB gene expression by the neutrophils of septic patients compared with those of uninfected controls in our study when both activating transcription factors are usually up-regulated in LPS-induced sepsis. 43 Perhaps the large number of polytrauma uninfected ICU controls (44% of the overall controls) might explain this contradictory result considering that tissue factor released after trauma enhances AP-1 and NF-κB gene expression and this effect might be stronger than LPS. 44 The increased expression of microRNAs in critical polytraumatized patients contributed to their pro-inflammatory status by increasing NF-κB activity. 45 However no differences in plasma cytokine levels between polytrauma and CVA uninfected controls to justify this hypothesis were observed in our study (data not shown). Previously reported associations of sepsis development or mortality with TNF-α (–308G/A), IL-1α (–889 C/T), IL-1β (+3954 C/T) and the IL-6(-174G/C) SNPs could not be demonstrated in our study.4–9, 28 The relatively small size of the cohort, the strict inclusion criteria we used and the low mortality rate might explain this discrepancy, as suggested by others. 2 , 46 All septic patients enrolled were immunocompetent and had positive blood cultures or a microbiologically demonstrated source of bacterial infection at ICU admission. The low mortality rate in this septic cohort of ICU patient with a mean of three organs that failed might be due to the exclusion of patients with cancer, HIV infection, transplantation or other causes of immunodepression. These immunocompromised patients, with an expected shorter life span due to their primary health problems, were usually included in previous ICU sepsis series. Our restrictive inclusion criteria also greatly limited the number of septic patients enrolled and expanded the recruitment window of the study.
Many studies based on few cytokines and chemokines measurements in sepsis have been published. In the present study, we assessed the profiles of nine inflammatory cytokines and chemokines in sepsis using the multiplex Ab array that measures multiple proteins simultaneously within a single sample. The simultaneous assessments of multiple cytokines have the advantage of discovering possible associations among them and with sepsis severity parameters. Most of the cytokines and MCP-1 studied here showed significantly increased plasma levels in septic patients compared with uninfected controls, as previously published.47–63 IL-6, IL-8, IL-10 and MCP-1 plasma levels correlated with a high number that organs that failed and high APACHE II score in our cohort, as reported by others.47–55 We found an independent association of plasma levels of IL-8 with sepsis diagnosis and mortality. IL-8 levels seemed to be a useful tool to predict sepsis mortality in our study. Our data agree with previous reports that showed the predictive value of IL-8 for diagnosis of sepsis after burn injury and of neonatal sepsis.56–62
Regarding the time course of expression of cytokines and chemokines, only IL-10 exhibited a persistent decrease between d 1 and 7 of ICU admission in septic patients. A confounding effect of sepsis therapy cannot be ruled out. However, except for TNF-α, cytokine plasma levels did not change in uninfected ICU controls that did not receive sepsis treatment. We could speculate that increases in IL-10 plasma levels over time might imply sepsis therapy failure or sepsis relapse. Our data agree with other reports from burned and septic patients. In such patients, in addition to having decreasing time course IL-10 slopes, this cytokine was a predictor of ICU mortality.54–56, 63
The main limitations of our study are the relatively small sample size, the low mortality rate and our Caucasian-only population. The relatively small sample size (90 septic cases and 91 controls) might bias the results in SNP-related studies such as the present one. More research in multi-ethnic larger populations of septic patients is needed to confirm our findings.
We report here the differential regulation of various inflammatory proteins that might contribute to sepsis pathophysiology. TNF-a (–238G/A) SNP could protect against sepsis development. This effect was independent of cytokines plasma levels or transcription factors expression by peripheral neutrophils. In addition, high levels of IL-8 were the best predictive markers of fatal outcome.
Footnotes
Acknowledgements
This work was supported by the Oviedo University research grants (UNIOV-12-MA-03 and SV- PA-13-ECOEMP-57) given to V.A. and by grants from Janssen Pharmaceuticals and Red Temática de Investigación de SIDA (RIS), Instituto de Salud Carlos III (ISCIII), Plan Estatal I+D+i & European Regional Development Fund (ERDF) ‘‘Una manera de hacer Europa’’ (grant RD06/0006/0010).
These results were presented in part at the 54th ICAAC Meeting, ASM, Washington DC, 5–9 September 2014, Abstract E-935.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.