
Abstract
Psoriasis is an (auto)immune-mediated disease that manifests as widespread desquamative erythema. The TNF-α/IL-23/IL-17A axis is crucial to its pathogenesis, which is demonstrated by its excellent therapeutic response to biologics that target this axis. There is a strong association between HLA-C*0602 and psoriasis, and researchers have identified autoantigens that are restricted to this major histocompatibility class I molecule. These auto-Ags include LL-37, A disintegrin and metalloprotease domain containing thrombospondin type 1 motif-like 5 (ADAMTSL5), and keratin 17. IL-17A-producing T cells have been identified in T cell populations that are reactive to these auto-Ags. In addition, lipid Ags have surfaced as candidate auto-Ags that activate IL-17A-producing T cells in a CD1a-restricted manner. In this article, we review the candidate auto-Ags that may contribute to the activation of the IL-17A-deviated immune response in psoriasis.
Keywords
Introduction
Psoriasis is an (auto)immune-mediated disease that manifests as widespread desquamative erythema,1,2 and occurs in approximately 2% of the general population of North America and Europe.1,2 Psoriasis patients represent 4.43% of all Japanese dermatological patients, 3 while its prevalence is estimated to be only 0.1% of the general population of Japan. 4 Males are twice as likely to be affected than females.4,5 The cosmetic disfigurement associated with psoriasis profoundly impairs the patients’ quality of life, treatment satisfaction and adherence, and socioeconomic stability.6–10
Therapeutic modalities for psoriasis include topical steroids, topical vitamin D3 derivatives, phototherapy, phosphodiesterase-4 inhibitors, cyclosporine, methotrexate, and biologics targeting TNF-α, IL-23, and IL-17A.11–19 The excellent therapeutic efficacy of anti-TNF-α/IL-23/IL-17A biologics for psoriasis point to a central role of the TNF-α/IL-23/IL-17A axis in its pathogenesis.20,21 Additionally, genetic and environmental factors are known to be involved in its pathogenesis.22–25
The autoimmune nature of psoriasis is exemplified by its high comorbidity with psoriatic arthritis,1,26 and other autoimmune diseases including autoimmune bullous diseases.27–31 The onset of psoriasis is commonly observed in patients who are infected with the human immunodeficiency virus or those who are undergoing treatment with immune checkpoint Abs.32–34 Psoriasis is also comorbid with cardiovascular diseases, metabolic diseases, and renal disorders, which represent a condition known as inflammatory skin march.35–41 Additionally, biological markers that represent systemic inflammation are elevated in psoriasis patients.42,43 It has also been shown that the biologics that target the TNF-α/IL-23/IL-17A axis also improve the symptoms of the comorbid diseases and the systemic inflammation.44,45
Genetic meta-analyses reveal that HLA-C*0602 is a strong susceptibility allele for psoriasis and that HLA-C*0602-positive patients with psoriasis exhibit a younger age of onset and a more severe phenotype than HLA-C*0602-negative patients.46,47 As a result, several HLA-C*0602-restricted auto-Ags have been identified.48–51 Additionally, some lipid auto-Ags are restricted to CD1a. 52 These auto-Ags-reactive T cells produce IL-17 and are considered to be pathogenic in psoriasis.48–52
In this review, we summarize the recent advances in the field concerning the pathogenesis of psoriasis with a focus on autoantigens.
The pathogenic role of the TNF-α/IL-23/IL-17A axis in psoriasis
The histopathology of psoriasis is characterized by epidermal acanthosis, accelerated keratinocyte proliferation, and infiltration of neutrophils and T cells (Figure 1). 1 Gene expression of TNF, IL23, and IL17A is up-regulated in the skin lesions of psoriasis.2,53 Three of the six IL17 family genes, IL17A, IL17F, and IL17C, are overexpressed in psoriatic lesions, but the pathogenic role of IL-17F and IL-17C remains unclear.54,55 IL-17A, which is produced by T helper 17 (Th17) cells and T cytotoxic 17 (Tc17) cells, accelerates the proliferation of keratinocytes.56–58 Additionally, IL-17A stimulates keratinocytes to produce cyto/chemokines that attract neutrophils (CXCL1, CXCL2, CXCL8, and IL-36) and Th17 cells (CCL20).56–60
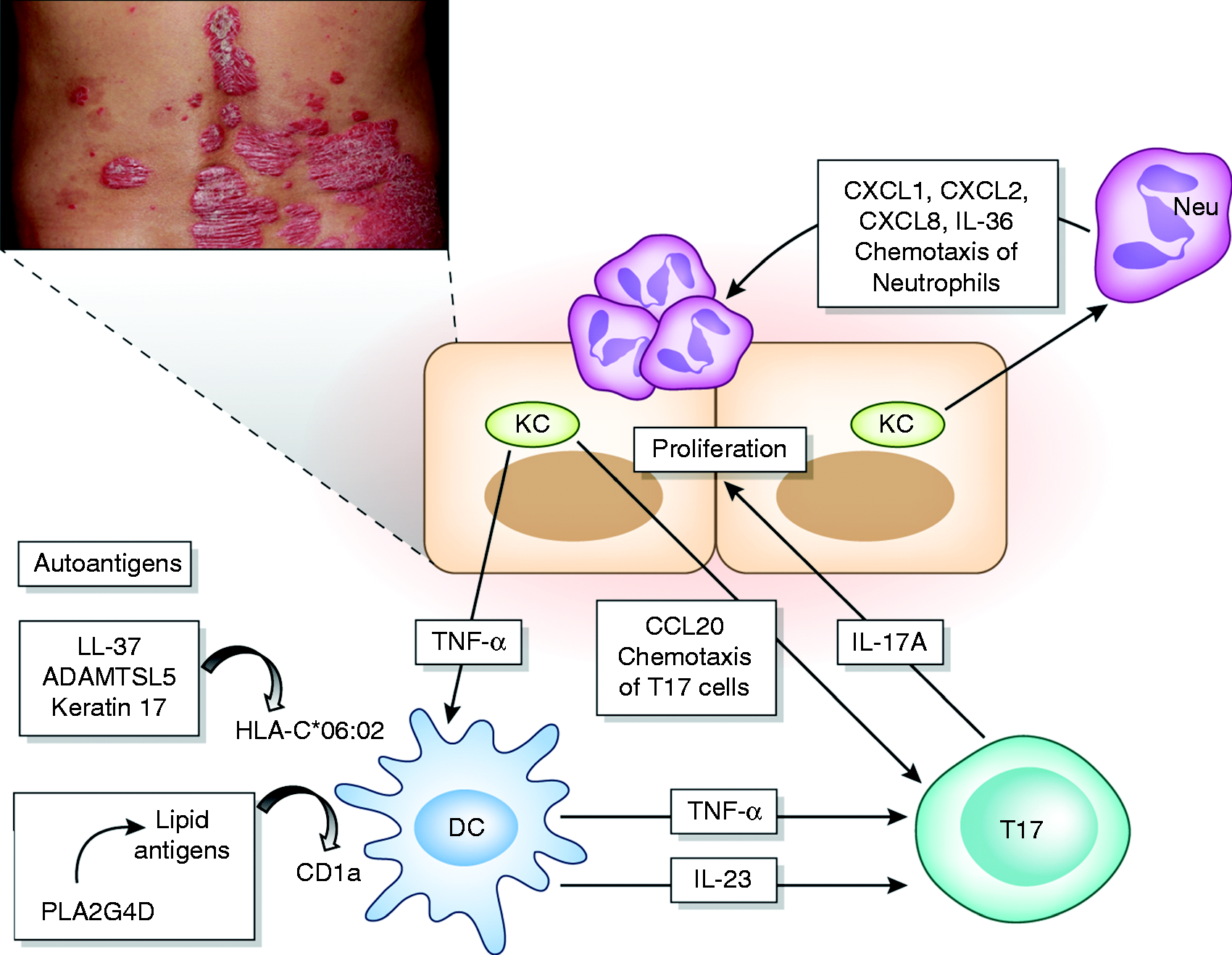
The simplified pathogenesis of psoriasis. Psoriasis is an (auto)immune-mediated inflammatory skin disease. Increased reactivity of T cells against autoantigens has been observed in psoriasis. Dendritic cells (DCs) present auto-Ags such as LL-37, ADAMTSL5, and keratin 17 in association with HLA-C*06:02. The phospholipase A2 group IV D (PLA2G4D) enzyme generates various lipid metabolites. Some lipid Ags are presented by DCs in association with CD1a. TNF-α and IL-23 produced by DCs induce IL-17A-producing T (T17) cells. IL-17A induces the proliferation of keratinocytes. IL-17A also induces the production of CXCL1, CXCL2, CXCL8, and IL-36 in keratinocytes, all of which stimulate neutrophil (Neu) migration into the epidermis. Moreover, IL-17A stimulates keratinocytes to produce CCL20, which recruits T17 cells. The TNF-α/IL-23/IL-17A axis plays a crucial role in the pathogenesis of psoriasis.
TNF-α and IL-23 are critical for dendritic cells (DCs) to induce and maintain Th17 and Tc17 cells.61–63 A highly sensitive immunohistological study found that the expression of TNF is confined to the HLA-DR+CD11c+ DCs and the CD163+ macrophages in psoriatic lesions. 64 In the first 48 h after an intravenous administration of the TNF antagonist infliximab, no overt changes in the number of TNF+ cells or signs of apoptosis were observed. However, a rapid decrease in IL-12/IL-23p40, CCL20, and IL-12/IL-23RB1 mRNA levels was detected, which suggests that TNF antagonism efficiently inhibits the activation of Ag-presenting cells. 64 In addition, psoriatic keratinocytes produced larger amounts of TNF-α as well as CXCL8 when compared to keratinocytes from healthy volunteers in ex vivo cultures. 65
IL-23 is composed of two subunits, p19 and p40. While the p19 subunit is an element unique to IL-23, the p40 subunit is shared with IL-12. 66 IL-12 is composed of the p40 and IL-12-specific p35 subunits. 66 IL-23 p40/p19 binds to the IL-23 receptor, which comprises IL-23R and IL-12RB1. 66 Dermal DCs and monocytes are major sources of IL-23 production. 67 At least 10 biologics have been used in clinics or in ongoing clinical trials, including anti-TNF-α (etanercept, infliximab, adalimumab), anti-IL-23 (ustekinumab, guselkumab, tildrakizumab, risankizumab), and anti-IL17 (secukinumab, ixekizumab, brodalumab) Abs. 19 Clinical efficacy is assessed by measuring reductions in the Psoriasis Area and Severity Index (PASI) after 12 or 16 wk of treatment. The PASI90 (the percentage of patients who achieved greater than a 90% reduction in their PASI score) for the anti-TNF-α agents (25.7–54.5%) is similar to or slightly less than the PASI90 for the anti-IL-23 agents (37–77%). 19 The PASI90 for the anti-IL-17 agents (59.2–70.9%) is comparable to the PASI90 for the anti-IL-23 biologics. 19 Thirty-to-forty percent of patients with moderate-to-severe psoriasis experience a clearance of skin lesions in response to treatment with some of these anti-IL-23 or anti-IL-17 biologics. 19 These results indicate a central role of the TNF-α/IL-23/IL-17A axis in the pathogenesis of psoriasis.
Auto-Ags in psoriasis
In psoriasis, IL-17A-producing Th17 cells and Tc17 cells emerge during DC/T cell Ag presentation in a TNF-α/IL-23-dependent fashion.63,68 As a major histocompatibility Ag, HLA-C*0602 is strongly associated with a genetic predisposition to psoriasis, and several laboratories have focused their attention on autoantigens that are restricted to HLA-C*0602 and induce IL-17, leading to autoimmunity in psoriasis.48,50 HLA-C*06:02 is present in more than 60% of psoriasis patients and is associated with an 8.9-fold increased risk in heterozygous carriers and a 23.1-fold increased risk in homozygous carriers, as well as an earlier onset of disease and a more severe disease course. 69 Although the auto-Ags that are responsible for the development of psoriasis are not fully understood, at least four have been identified in psoriasis, namely, LL-37 (cathelicidin), A disintegrin and metalloprotease domain containing thrombospondin type 1 motif-like 5 (ADAMTSL5), keratin 17, and lipid Ags that are generated by phospholipase A2 group IV D (PLA2G4D).48–52
LL-37 (cathelicidin)
LL-37 is an anti-microbial peptide of human cathelicidin that is produced when keratinocytes are injured by a broad range of bacteria. 70 The released LL-37 binds to the infiltrated neutrophils. 70 Neutrophils are a rich source of extracellular DNA due to their neutrophil extracellular traps. 71 Upon stimulation with complexes of host DNA and LL-37, plasmacytoid DCs produce large amounts of IFN-α. 72 Notably, LL-37 induces the proliferation of circulating CD3+ T cells in 24 out of 52 psoriasis patients (46%). 50 LL-37-reactive CD3+ T cells include both CD4+ and CD8+ T cells and express the skin-homing receptor cutaneous lymphocyte Ag. 50 LL-37 peptides bind to HLA-DR in DCs and are presented to CD4+ T cells, while LL-37 peptides and HLA-C*0602 complex has been demonstrated to activate CD8+ T cells. 50 The majority of LL-37-reactive CD3+ T cells produce IL-17 and the capacity of their IL-17 production is associated with disease severity. Interestingly, the LL-37-specific IL-17-producing T cells are exclusively CD4+ whereas the LL-37-specific CD8+ T cells do not produce IL-17. 50
A disintegrin and metalloprotease domain containing thrombospondin type 1 motif-like 5 (ADAMTSL5)
Intraepidermal CD8+ T cells have been the focus of several research groups in psoriasis.48,73–75 The intraepidermal CD8+ T cells are oligoclonal and use a restricted set of T cell receptor β chains. 73 The majority of epidermal CD8+ T cells also co-express α1β1 integrin. 74 In a xenotransplantation mouse model, the xenotransplanted nonlesional skin from a psoriasis patient gradually develops psoriatic lesions at 35 d posttransplant. The onset of the psoriatic epidermal changes occurs in parallel with the appearance of epidermal T cells expressing α1β1 integrin. 74 Additionally, the blockade of α1β1 integrin by specific Abs inhibits the immigration of epidermal T cells and the development of psoriatic lesions in the xenotransplantation model. 74
A recent study by Arakawa et al. demonstrated that intraepidermal CD8+ T cells recognize ADAMTSL5 on melanocytes in association with HLA-C*06:02. 48 In the epidermis, ADAMTSL5 is only expressed by the melanocytes. 48 Contact is observed between melanocytes and, on average, 37.2% of the intraepidermal CD8+ T cells in psoriasis. A synthetic ADAMTSL5 peptide increases the frequency of CD8+ T cells expressing IL-17A and IFN-γ in the peripheral blood mononuclear cells (PBMCs) in psoriasis patients, but the same effect is not found in healthy individuals. 48 Approximately one-third of psoriasis patients are HLA-C*06:02 negative, yet PBMCs from both HLA-C*06:02-positive and HLA-C*06:02-negative patients react similarly to ADAMTSL5 peptide stimulation, which suggests that HLA class I molecules other than HLA-C*06:02 may present ADAMTSL5 and promote melanocyte-specific autoimmunity. 48
Keratin 17
The onset of acute guttate psoriasis is frequently associated with throat infections by group A β-hemolytic streptococci. 76 The streptococcal M-protein is a surface molecule of Streptococcus that has extensive amino acid sequence homology with human keratin 17. 77 The keratin 17 peptide induces a significantly higher number of IFN-γ-producing T cells in psoriasis patients than it does in healthy controls. This T cell response to the keratin 17 peptide is much stronger than its response to the M-protein peptide. 77 Shen et al. have confirmed that the keratin 17 peptide is a potent stimulator of IFN-γ production in the T cells of psoriasis patients, 78 which further indicates a molecular mimicry of the keratin 17 peptide by the streptococcal M-protein. 79 However, it is still not known if keratin 17-reactive T cells have the ability to produce IL-17A.
Yunusbaeva et al. have also demonstrated that the proliferative response to full-length keratin 17 and its peptides is significantly increased in psoriasis patients when compared to healthy controls. 51 In their case series, the positive ratio of the HLA-C*06:02 allele is 53.85% in psoriasis patients and 14.29% in healthy controls. The HLA-C*06:02 allele dose is strongly associated with the T cell proliferative response to keratin 17 peptides. 51 In addition, endogenous proteins other than keratin 17, such as maspin, ezrin, PRDX2, hsp27, and potentially keratin 6 have been previously shown to act as auto-Ags in both the streptococcal-induced autoimmune response and in psoriasis. 80
Neolipid Ags generated by PLA2G4D
PLA2G4D is found in psoriatic lesions but is absent in normal skin. 81 Mast cells are known to be the primary cellular source of PLA2G4D. 52 In patients who are comorbid with psoriasis and eczema, PLA2G4D expression is up-regulated in psoriatic lesions when compared to eczematous lesions. 82 PLA2 contributes to the generation of lipid metabolites such as arachidonic acids. 83 Cutaneous DCs, such as Langerhans cells, express CD1a and present lipid Ags to autoreactive T cells. 84 Bee venoms and house dust mites contain exogenous PLA2 activity and are known to activate CD1a-restricted T cells.85,86
In psoriasis, the number of CD1a-restricted autoreactive T cells in the blood is increased when compared to healthy controls. 52 Psoriatic skin lesions harbor increased numbers of these autoreactive T cells compared to nonlesional skin in psoriatic patients and healthy control skin. 52
These autoreactive T cells respond in CD1a-dependent manner to fatty acids and lysophospholipids, all of which are generated by PLA2G4D. 52 These CD1a-restricted neolipid Ag-reactive T cells produce IL-17A, IFN-γ, and IL-22. Mast cells are the major cellular source of PLA2G4D and mast cell-derived exosomes deliver PLA2G4D to DCs. 52 These results suggest that lipid Ags may also be meaningful auto-Ags in the development of psoriasis.
Conclusion
Psoriasis is a TNF-α/IL-23/IL-17A-driven inflammatory skin disease that is significantly affected by genetic (e.g., HLA-C*06:02) and environmental factors. 27 While the antigenic properties that lead to the development of psoriasis remain elusive, auto-Ags such as LL-37, ADAMTSL5, keratin 17, and neolipids are promising candidate molecules. Autoreactive T cells to these self-Ags are partly restricted to HLA-C*06:02 or CD1a. Moreover, the autoreactive T cells appear to include IL-17A-producing T cell clones. In a particular circumstance, the production of IL-17 may possibly occur in the very early post-presentation phases of the Ag and not always under the compulsory influence of IL-23. Considering a diverse plasticity of Th17 cells, the primed Th17 cells may differentiate into other types of helper T cells in different cytokine milieu in autoimmunity. 87 Further studies are required to elucidate the precise role of these auto-Ags in the pathogenesis of psoriasis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by grants from The Ministry of Health, Labour, and Welfare, Japan (H30-Shokuhin-Shitei-005) and The Leading Advanced Projects for Medical Innovation, Japan (LEAP).