
Abstract
Fibromyalgia (FM) is a syndrome characterized by widespread chronic pain and is associated with elevated systemic inflammatory biomarkers, and an elevated innate cellular response. The aim of this study was to determine if fibromyalgia patients have altered ability to release pro-inflammatory chemokines by isolated neutrophils and monocytes. The study participants were women diagnosed with FM (n = 6) and a control group of healthy women (HW) (n = 6). Supernatant concentrations of eotaxin (CCL11), human macrophage-derived chemokine (MDC) (CCL22) and growth regulated-oncogene (GRO-α) (CXCL1) released by both monocytes and neutrophils either resting or stimulated by LPS were determined by ELISA and compared between the FM and HW groups. Both resting and activated monocytes from FM patients released more eotaxin, MDC and GRO-α than those from HW. However, there were no significant differences in the release of chemokines from neutrophils of FM patients and the ones from healthy women. In conclusion, monocytes from women with FM are deregulated, releasing higher amounts of eotaxin, MDC and GRO-α than healthy individuals. This fact does not occur in neutrophils from women with FM.
Introduction
The innate immune system is composed of a humoral and a cellular part, which mainly involves specialized cells known as phagocytes. Among the most important phagocytic cells located in the blood are the neutrophils and the monocytes. Phagocytes, apart from to phagocytose, can contribute to the arrival and activation of a variety of cells through the production of inflammatory mediators. Nevertheless, an over-activation of the innate immune system has side effects—collectively known as inflammation—mainly due to tissue damage of the host. In the long term, the persistent inflammation contributes to the development of inflammatory diseases. 1
Thus, chemokines are among the inflammatory mediators releasing phagocytes. They are cytokines with chemotactic properties that have roles in a wide range of immune and inflammatory responses through the chemoattraction exerted on cells of the innate and adaptive immune response. 2 They selectively control such phenomena as adherence, chemotaxis and the activation of many types of populations and subpopulations of leukocytes, and hence are major regulators of the leukocyte traffic. Furthermore, chemokines appear to be molecules with a role in coordinating nociceptive events associated with injuries. They increase sensitivity to pain by direct action of their receptors expressed in nociceptive neurons, 3 and also serve to regulate the inflammatory response, acting simultaneously on elements of the nervous system,4,5 suggesting an important role in the pathophysiology of autoimmune diseases such as rheumatoid arthritis, multiple sclerosis, systemic lupus erythematosus and fibromyalgia (FM).5–7
According to the American College of Rheumatology (ACR), FM is defined as the presence of widespread pain and tenderness at 11 or more of 18 specific tender point sites. 8 Thus, core symptoms of the FM include pain, fatigue, and mood and sleep disturbances.9–11 Based on the assumption that the origin of all pain is inflammation and inflammatory response, 12 special attention has been placed on the FM inflammatory hypothesis, 13 with the implication of inflammatory cytokine involvement in the syndrome and in the modulation of pain. 14 Thus, high levels of IL-8 have been found in FM.15–18 Nevertheless, the release of chemotactic cytokines, or chemokines, by isolated phagocytes (neutrophils and monocytes) has not been properly analyzed in people suffering FM. Only one study has shown a high release of monocyte chemoattractant protein-1 (MCP-1/CCL2) by isolated monocytes from women affected by FM in relation to healthy women (HW). 18 In the same study a decrease in the production of regulated upon activation normal T-cell expressed and presumed secreted (RANTES/CCL5) by monocytes from FM patients was also observed. 18 Furthermore, we have reported in previous studies a increased chemotactic capacity of neutrophils from FM patients.18,19
As proper functionality of monocytes and neutrophils is essential to carry out a good innate immune response and therefore develop a good global immune response, and also taking into account the fact that in FM it seems that the cellular bases of the innate surveillance are unregulated, we decided to study whether phagocytes (neutrophils and isolated monocytes) of FM patients have impaired ability to release pro-inflammatory chemokines (with chemoattractant capacity on these cells), such as growth-regulated oncogene-α (GRO-α/CXCL1), 20 human macrophage-derived chemokine (MDC/CCL22) and eotaxin (CCL11) with respect to phagocytes from HW.
Materials and methods
Study design and FM patients
Anthropometric, demographic and clinical data.
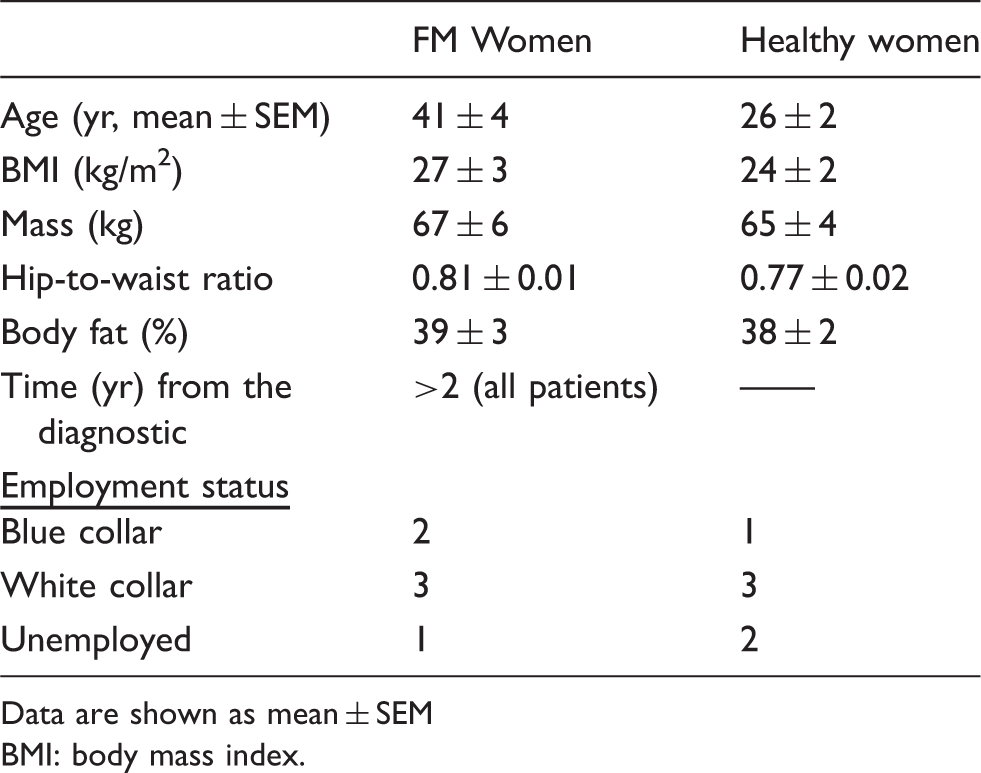
Data are shown as mean ± SEM
BMI: body mass index.
Inflammatory cell isolation
Blood samples were centrifuged in a density gradient (Histopaque; Sigma, St. Louis, MO, USA) obtaining a first halo containing monocytes and lymphocytes and a second one containing neutrophils. These two suspensions were washed in PBS. Isolated neutrophils were adjusted to 106 cells/ml in Iscove Medium (GIBCO, Grand Island, NY, USA) supplemented with 10% FBS, 1% penicillin/streptomycin and 1%
Determination of inflammatory chemokines released by phagocytes
Monocytes and neutrophils were cultured for 24 h at 37℃, 5% CO2 and 100% RH in flat-bottom 48-well cell culture plates (Falcon; Becton Dickinson Labware, Franklin Lakes, NJ, USA) in both the absence (‘resting cells’) and presence of 20 μl bacterial LPS from Escherichia coli 0111:B4 (Sigma) as ‘activated’ samples, yielding a final concentration of 50 µg/ml. Cell viability was checked by the Trypan Blue Exclusion Test, finding at least 98% viable cells. Supernatants were aliquoted in Eppendorf tubes and stored at –80℃ until assay. Both constitutive release by phagocytes (monocytes and neutrophils) and release by ‘activated’ phagocytes of eotaxin/CCL11 (RayBiotech, Norcross, GA, USA), MDC/CCL22 (CUSABIO, Wuhan, China), and GRO-α/CXCL1 (RayBiotech) were evaluated by ELISA, and compared between the FM and HW groups.
Statistical analysis
Values are given as the mean (± SEM). The variables were normally distributed (Kolmogorov–Smirnov test). Student’s t-test was used to compare the results between the HW and FM groups. The significance level was set at P < 0.05. The analyses were performed using GraphPad Prism 5.0.3 (GraphPad Inc., La Jolla, CA, USA).
Results
Figure 1 shows the results relating to the capacity of monocytes to release inflammatory chemokines as eotaxin, MDC and GRO-α. The monocytes from women with FM released constitutively (‘resting monocytes’) more eotaxin (P < 0.001) (Figure 1A), MDC (P < 0.05) (Figure 1C) and GRO (P < 0.05) (Figure 1E) than those from HW. In the same way, activated monocytes by LPS from FM patients also released more eotaxin (P < 0.05) (Figure 1B), MDC (P < 0.05) (Figure 1D) and GRO-α (P < 0.01) (Figure 1F) than those from HW.
(a) Eotaxin, (c) MDC and (e) GRO-α released by monocytes (‘resting monocytes’) and by (b, d, f) LPS-activated monocytes (‘activated monocytes’) from healthy women (HW) and from patients with FM. The results are present as the mean value ± SEM of six experiments performed in duplicate (one experiment per volunteers). * P < 0.05, ** P < 0.01 and *** P < 0.001 with respect to HW.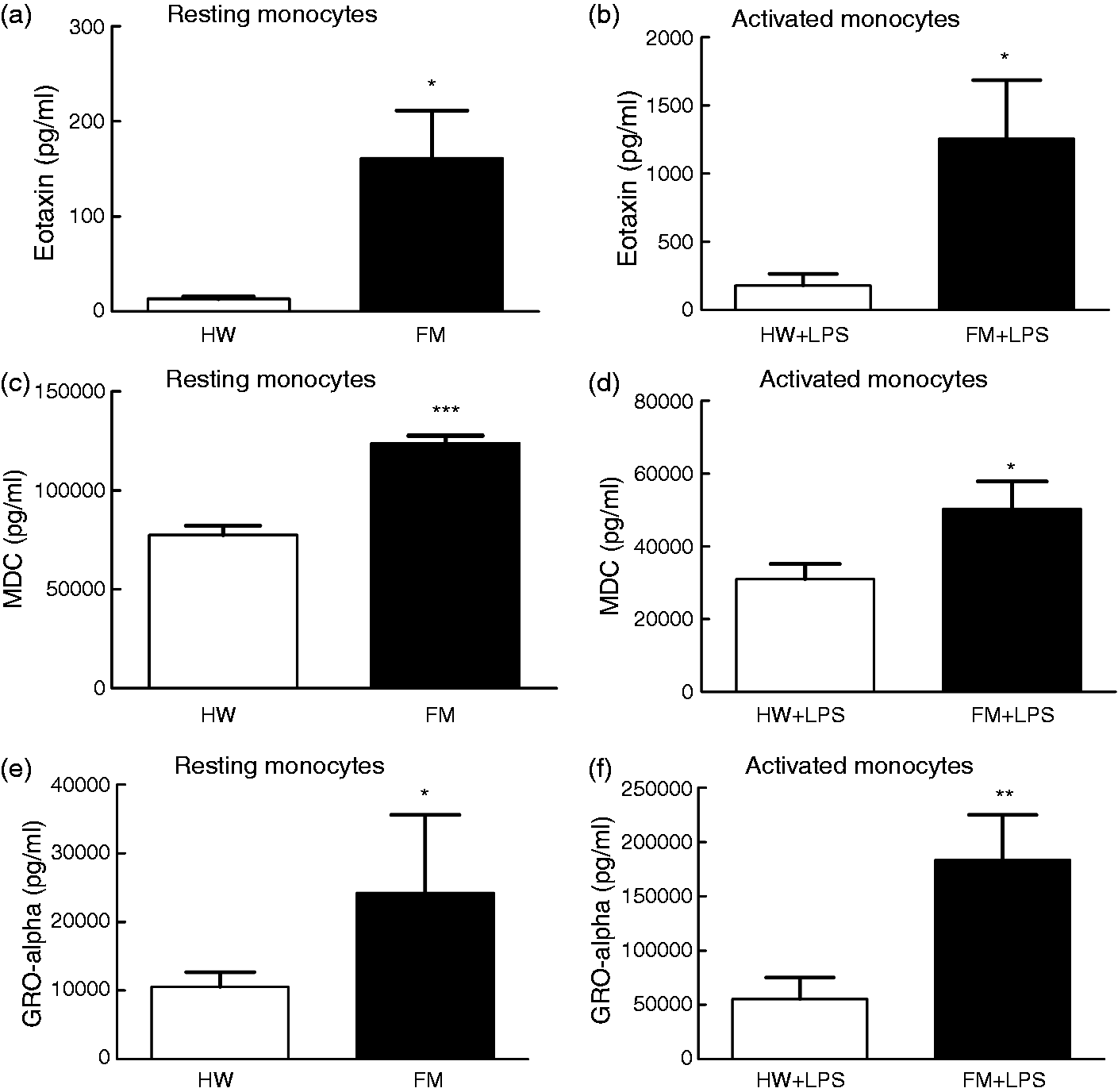
However, as shown in Figure 2, the ability of neutrophils to release these inflammatory chemokines (MDC, eotaxin and GRO-α) was similar (P > 0.05) both in FM patients and healthy women; this behavior was similar in the absence of LPS (‘resting neutrophils’; Figure 2A, C, E) and in the presence of LPS (‘activated neutrophils’; Figure 2B, D, F).
(a) Eotaxin, (c) MDC and (e) GRO-α released by neutrophils (‘resting neutrophils’) and by (b, d, f) LPS-activated neutrophils (‘activated neutrophils’) from healthy women (HW) and from patients with FM. The results are present as the mean value ± SEM of six experiments performed in duplicate (one experiment per volunteer).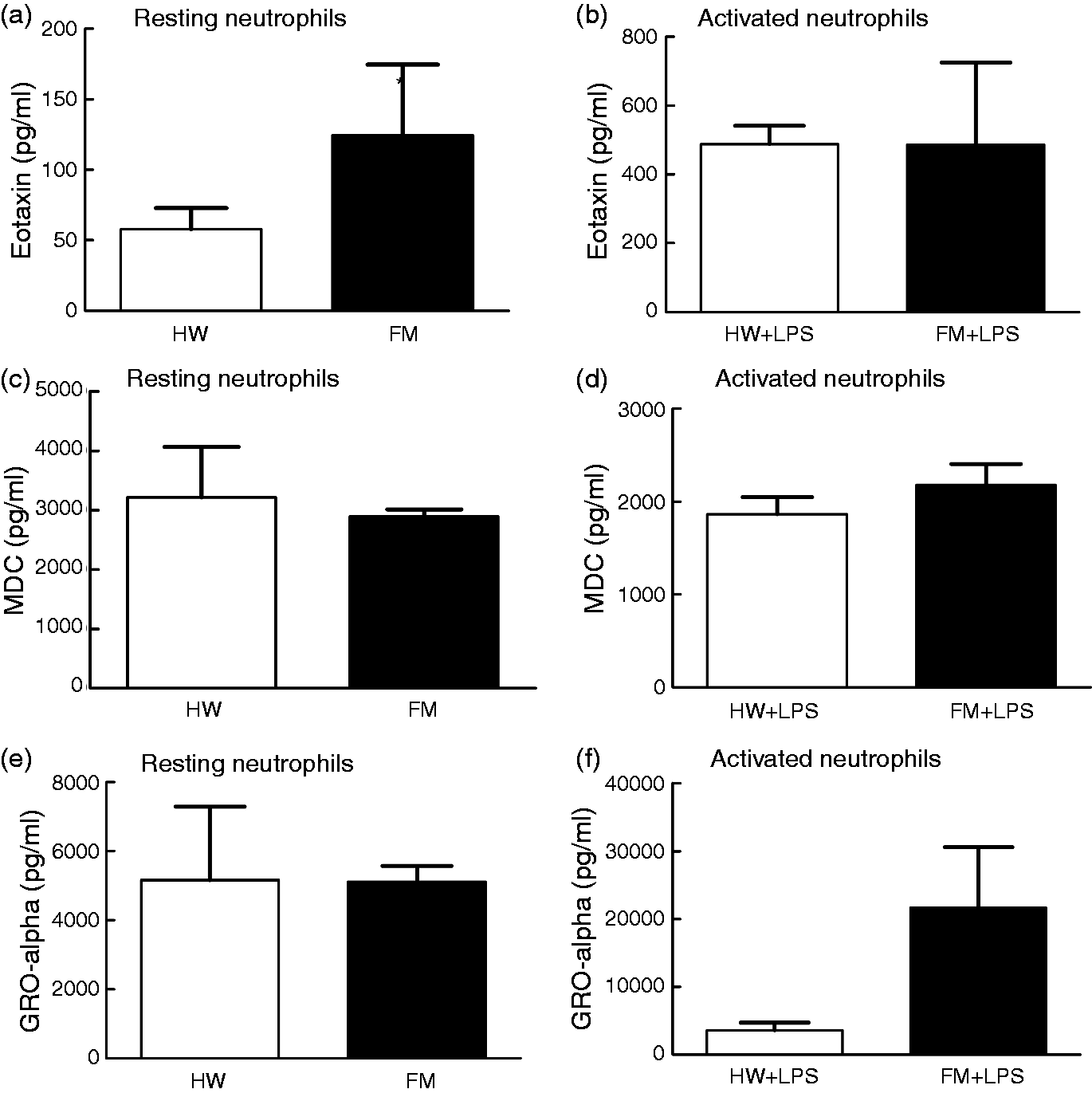
Discussion
It has always been believed that something must be bound by a receptor (either specific or non-specific, ‘self’ or ‘non-self’) of a phagocyte (monocyte/macrophage and/or neutrophil) for it to be activated, triggering an innate immune response. If this response does not achieve the removal of the response activator, then it will trigger an adaptive immune response. According to Janeway and Medzhitov, 22 innate immunity is behind most of the inflammatory responses, all of which are activated in the first instance by monocytes/macrophages, polymorphonuclear leukocytes and mastocytes by means of its innate immunity receptors. Furthermore, according to Omoigui,12,13 who hypothesized that the origin of all pain is the inflammation and the inflammatory response, it makes sense to think that pain that characterizes FM is provoked, at least in part, by the inflammatory component present in this syndrome, which has already been established by different studies.5,15–19,23,24 According to Janeway and Medzhitov, 22 who determined that any inflammatory process has behind it an activation of the innate immunity, in FM a functional activation of the neutrophil phagocytic process is taking place, showing these cells have a higher chemotactic capacity, a higher phagocytic capacity than Candida albicans and a higher microbicide capacity,18,19,24 along with a higher level of oxidative stress. 25 With respect to monocytes from women with FM, it has been described that these cells show some deregulation regarding the release of pro-inflammatory cytokines, such as TNF-α, IL-1β, IL-6, IL-18 and MCP-1,8,19,23 and anti-inflammatory cytokines such as IL-10. 23 However, this increased release of cytokines by monocytes from FM patients is not correlated with the higher systemic levels of IL-8, IFN-γ, MDC, I-TAC, eotaxin and MIG found in previous studies of FM patients.5,17,18 In the present study, it is confirmed that the monocyte deregulation shown by patients with FM, featuring a higher release of inflammatory chemokines (GRO-α, MDC and eotaxin), occurs in both a spontaneous way and after antigenic stimuli (with LPS). This fact was not observed on the neutrophils. GRO-α/CXCL1 belongs to the group of chemokines (CXC) that contains in their structure the ELR motif (ELR+), which predominantly performs stimulating and chemotactic activities towards the neutrophils.20,26–29 The role of CXC ELR+ chemokines is to promote the adherence of the neutrophils towards the endothelial cells and the subsequent migration. 20 Hence, GRO-α has chemotactic effects upon neutrophils,30,31 and may also stimulate the production of O2– by means of these same phagocytic cells in order to increase its microbicide capacity. 32 Moreover, CC-type chemokines (i.e. MDC/CCL22, eotaxin/CCL11, MCP-1/CCL2) mainly attract monocytes, eosinophils, basophils and lymphocytes. Nevertheless, they may also attract neutrophils under certain conditions. 33 Based on the above, in our opinion increased functional activity of neutrophils in FM could well be due, at least in part, to the increased release of GRO-α, MDC and eotaxin by isolated monocytes from women with FM.18,19,24 This increase in the release of MDC and eotaxin also corresponds with the high plasmatic levels of these chemokines observed in patients with FM. 5 This increase of the chemokines, at the local level, produced by monocytes from FM patients would be stimulating the sensation of pain in these patients because chemokines increase pain sensitivity by directly acting on their receptors (which are present along the entire pathway of pain in the peripheral nerves, the sites of nerve damage, the dorsal root ganglia and the spinal cord 3 ), as most of these chemokines are molecules that mediate both inflammatory and neuropathic pain.4,34,35
In summary, monocytes from women with FM show an alteration in the release of inflammatory chemokines (eotaxin, MDC and GRO-α). These chemokines may be mediating both the stimulation of the neutrophil phagocytic process and pain in FM patients. Thus, non-lethal malfunctions of the innate immunity could be occurring in FM which would provoke low-grade inflammation, where monocytes may play a prominent role. In conclusion, monocytes from women with FM women are deregulated, releasing higher amounts of eotaxin, MDC and GRO-α than monocytes of healthy individuals. This does not occur in neutrophils from FM patients.
Potential limitations of the investigation
Although the conclusions of the present pilot study are based on statistical analysis between volunteers with FM (n = 6) and healthy women as controls (n = 6), a limitation could be the small size of the sample. In any case, in our opinion, it can open further clinical investigations with a greater number of patients. Another limitation of the present study could be the difference in age between patients with FM and HW. Although, to the best of our knowledge, there are no published data reporting age-associated (range 20–60 yr) changes in the concentration of the chemokines determined in the present investigation. And in our previous experience, we did not find variations in the release of inflammatory cytokines from women of the same range of age (‘adult women’).
Footnotes
Acknowledgements
We thank the Fibromyalgia Associations of Badajoz, Spain, for its invaluable collaboration. We would like to thank to D. César González, director of Kent House School, and Dr. Pedro Reyes for language revision. This work was supported by grants PRIS10019 (FUNDESALUD) and PRI09A003 (Junta de Extremadura-FEDER).
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.