
Abstract
This study reports the preliminary results of a technique for redistributing muscles at the wrist in the stump of hand amputees by suturing the tendons to the dermis. The technique has the potential to improve control of hand prostheses by detecting movement intentions.
Although intelligent bionic prosthetic devices for the hand have rapidly evolved during the past few decades, current prosthetic limbs are unable to replicate the complex functions of the hand because of the lack of an ideal interface between the prosthesis and residual limb (Semasinghe et al., 2019). Most myoelectric prosthetic hands identify human motion intentions by collecting surface electromyography (sEMG) signals and then control the movements of the prosthesis. For patients with wrist-level amputation, although the muscle–tendon units that control important motions (such as the units in the thumb and index fingers in the forearm stump) are intact, these muscles are small in size and located deep within the forearm muscle layer; thus, it is impossible to accurately acquire their EMG signals.
Limb surface deformation signals have been used for the recognition of human motion intentions in recent years. Studies have shown that intelligent prosthetics can detect limb surface deformation, decode human motion intentions and accurately control the movements of the prosthesis through capacitive sensors (Grushko et al., 2020; Zheng and Wang, 2017).
Combining the anatomical characteristics of the forearm and previous study findings regarding the deformation signals reflecting human motion intentions, we designed a muscle redistribution technique (MRT) for patients with wrist-level amputation. MRT involves transferring the tendons of muscles that control the thumb and index finger in the forearm and suturing the tendons to the dermis of the stump. When the muscles contract, the tendons pull the skin to form a distinct depression deformation. The skin deformation signals can be detected, decoded and analysed by a contact sensor, allowing the prosthetic hand to acquire the motion intentions and complete more complex and delicate hand movements.
Since 2016, we have completed six MRT procedures for patients with wrist-level amputation. A fish-mouth or L-shaped incision was made on the stump. The flexor pollicis longus (FPL) and flexor digitorum profundus of the index finger (FDPII) were explored on the palmar side, and the extensor longus pollicis (EPL) and extensor indicis proprius (EIP) on the dorsal side. The tendons and muscles were freed proximally, taking care to protect the neurovascular bundles. The tendons were sutured 3–4 cm from the limb stump, and the distance between the centres of the suturing points was more than 3 cm. The tendon of FPL was sutured on the palmar side of the radius, FDPII on the palmar side of the ulna, EPL on the dorsal side of the radius and EIP on the dorsal side of the ulna. After the position at which the tendons would be sutured was determined, the subcutaneous tissue was incised to expose the dermis. The musculotendinous units were pulled slightly distally, and the tendons firmly sutured to the dermis using 2-0 Ethibond (Johnson & Johnson, New Brunswick, NJ, USA) suture. The local skin depression depth was usually 1 mm after suturing (Figure 1).
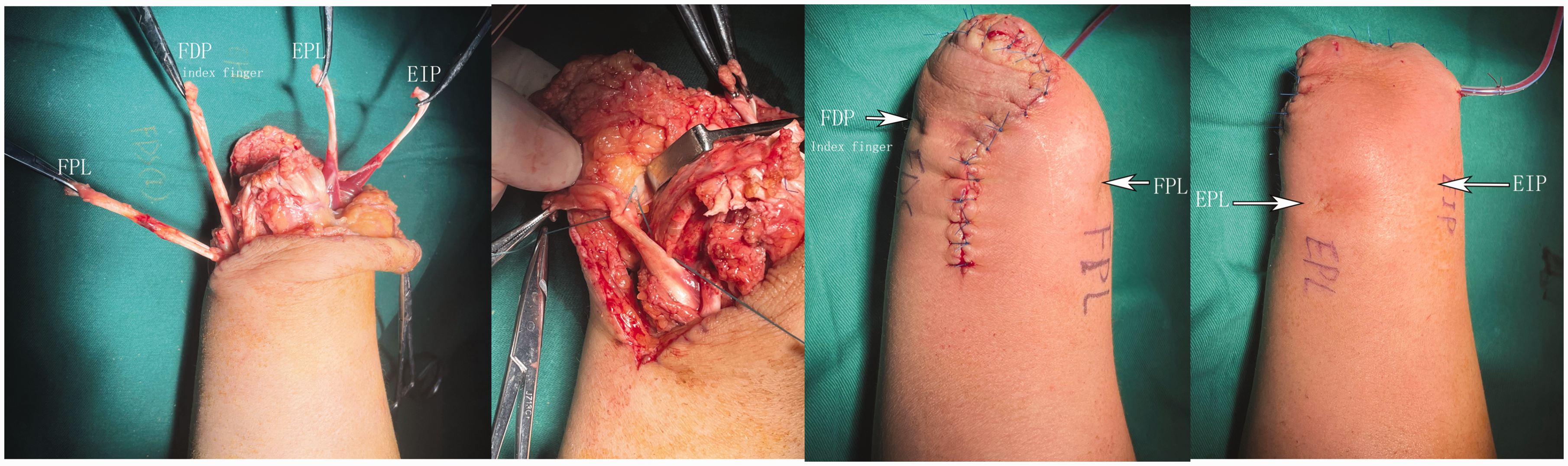
(a) Tendons involved in the muscle redistribution technique; (b) the tension of the transfer tendon is adjusted, and the tendon is sutured to the dermis; (c) appearance of the anterior aspect of the stump after tendon transfer and (d) dorsal appearance after tendon transfer. FDP: flexor digitorum profundus; EIP: extensor indicis proprius; EPL: extensor pollicis longus; FPL: flexor pollicis longus.
Shoulder and elbow joint functional exercises were started immediately postoperatively. Active contraction training of the transferred muscles was started 4 weeks postoperatively, and the frequency, intensity and duration of the exercises was gradually increased. In one patient with an explosion-induced injury of the hand, wound healing was delayed for 5 weeks after operation.
Effective deformation in the present study was defined as the tendon suture point after MRT, simultaneously satisfying two conditions: ≥10-mm maximum diameter and ≥2-mm maximum depth of the depression. The follow-up time was in the range of 6–62 months (mean 36, SD 25). At the final postoperative follow-up, when the muscles contracted, the mean width and depth of deformation were 10.8 mm (SD 3) and 2.3 mm (SD 0.8) for FPL, 9.2 mm (SD 3.4) and 2.0 mm (SD 0.6) for FDPII, 9.7 mm (SD 2) and 2.2 mm (SD 0.4) for EPL, and 6.7 mm (SD 2) and 1.2 mm (SD 0.40) for EIP, respectively. The effective deformation rate was 13/24 transfers, and the number of effective motion signal sources increased by an average of 2.2. Effective deformation occurred for FPL in 5/6 cases, FDPII in 3/6, EPL in 5/6 and EIP 0/6.
We measured the amplitude of the sEMG in the forearm to detect whether the conventional EMG signals are affected by the MRT procedure. Comparing preoperative and postoperative values, the palmar (p = 0.220) and dorsal muscle groups (p = 0.416) showed no significant difference in the amplitude of the sEMG signal during maximal contraction (Table S1).
Significant skin deformations were largely associated with muscle units, which are both independent and have high muscle volume and tendon glide (Korstanje et al., 2012). For muscles that cannot produce effective deformation after MRT, we will consider transferring the whole muscle subcutaneously with the nerve branches and nutrient vessels intact and acquiring the movement intention by collecting its EMG signal.
In summary, MRT transfers the key muscles in the forearm stump, effectively increasing the number of signal sources that express human motion intentions through skin deformation. This has the potential to obtain greater intuitive control of a multi-degree-of-freedom prosthetic hand. However, further study is needed to confirm improved function using intelligent prosthetic hands.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934231196438 - Supplemental material for Muscle redistribution technique for expressing motion intention in patients with wrist-level amputation
Supplemental material, sj-pdf-1-jhs-10.1177_17531934231196438 for Muscle redistribution technique for expressing motion intention in patients with wrist-level amputation by Yong Yang, Qining Wang and Qipei Wei in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This work was carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. The study was approved by Beijing Jishuitan Hospital (No. 201803-21).
Funding
This work was supported by the National Natural Science Foundation of China (81972131) and Beijing Institute of Trauma Orthopedics Foundation (PXM2021_026275_000004).
Informed consent
All patients provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.