
Abstract
Background:
Due to advancements in three-dimensional printing, custom-made prostheses are becoming more viable options for persons with difficult cases of prosthetic management. The purpose of this article was to develop a custom voluntary-closing, body-powered thumb mechanism for a partial-hand amputee who had amputations of the index finger and thumb on the left, non-dominant hand.
Case description and methods:
The prosthesis model was manufactured using rapid prototype technology and was developed to provide greater force and functionality, and to decrease overall size compared to traditional hand prostheses.
Findings and outcomes:
Following device iterations and occupational therapy sessions, the patient achieved higher functionality in performing daily tasks such as cooking and cleaning, and in completing the Box and Blocks test, though some limitations still precluded full acceptance of the device.
Conclusion:
This case study represents a unique approach in the development of custom-made devices that may increase prostheses acceptance rates among partial-hand amputees.
Clinical relevance
Many partial-hand amputees report experiencing trouble in finding a device that fits their needs. This study highlights the potential of using rapid prototyping technology to design a prosthesis that meets a user’s specific desires.
Background
Despite retaining the ability to use their arm, individuals with partial-hand amputation report having higher levels of perceived disability compared to persons with major unilateral upper-limb amputation. These individuals also often experience decreased strength and range of motion in their residual limb. 1 These limitations, combined with varying levels of amputated digits, can make it challenging to fit clinically available devices that will restore function and fit comfortably while remaining manageable in size. The aim of this case study was to develop and evaluate a custom body-powered device for a patient with a partial-hand amputation. Due to the nature of the patient’s injuries, it was difficult to fit him with traditional body-powered or passive functional prostheses. In order to provide the highest level of patient satisfaction and functionality, we used rapid prototyping technology to iterate on a design following patient and clinician feedback.
Case description and methods
The patient was a 50-year-old male with amputations of the index finger and thumb on the left, non-dominant hand, secondary to trauma. The patient’s residual limb also sustained an injury resulting in no functional flexion, extension, or supination of the wrist, as well as extremely limited active flexion and extension of the remaining fingers (less than 18° at the metacarpophalangeal joint and less than 12° at the proximal interphalangeal joint). The length of his remaining fingers and restricted motion of his limb made it challenging to fit conventional body-powered prostheses. Initially, the patient was fit with a passive silicone restoration, as well as a body-powered Handy Hook Adapter (Fillauer, LLC). The Handy Hook was quickly rejected due to the lack of visual feedback and size (see Figure 1). The patient’s clinical team determined that a custom device may be the best functional solution for this case and engineering support was enlisted.
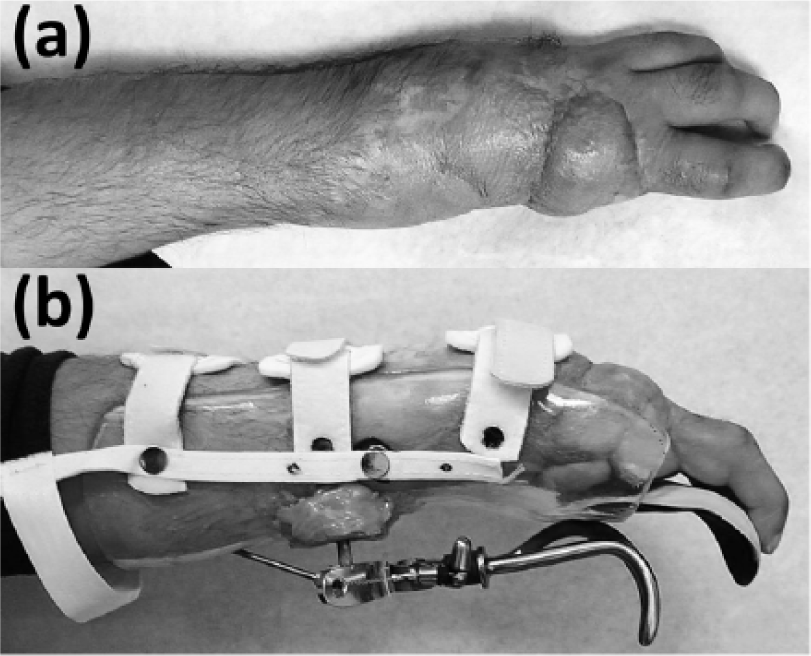
(a) Patient’s residual limb and (b) Handy Hook Adapter.
Prototype development
The custom prosthesis developed in this study was a voluntary-closing, body-powered thumb mechanism which was mounted to the palmer side of a socket to oppose the patient’s residual fingers much like a sound hand. The main objective in developing a custom device was to create a mechanism that would interact with the patient’s residual fingers to provide force and tactile feedback. We were also able to improve the line of sight when using the device, which was the cause for the rejection of the Handy Hook. A voluntary-closing device was preferred, allowing the patient to adjust the pinch force of the device through force input of the cable harness. The alternative, voluntary-opening, would result in a constant pressure force being applied to the fingers, which may have felt uncomfortable or even caused wounds with time.
The design goal for this body-powered thumb was to be lightweight (equal to or less than that of the Handy Hook), low profile, and rugged while maintaining a simple design layout. 2 These specifications made it easy and cost effective to perform maintenance when needed. The design consisted of four primary features: a mounting bracket, tong, cable interface, and thumb as shown in Figure 2. A simple bolt pattern was used to attach the mounting bracket to the socket with standard 6–32 screws. The spring that biased the device to the open position was a Hosmer hook ring, and the cable attachment interface was designed to mate with any clinically available 9/32″ ball terminal. The original shape of the thumb was designed to be anthropomorphic to provide some level of cosmesis. The final weight of the device (not including socket) is an estimated 250 g, comparable in weight to a Hosmer model 5 and Handy Hook mounting hardware.
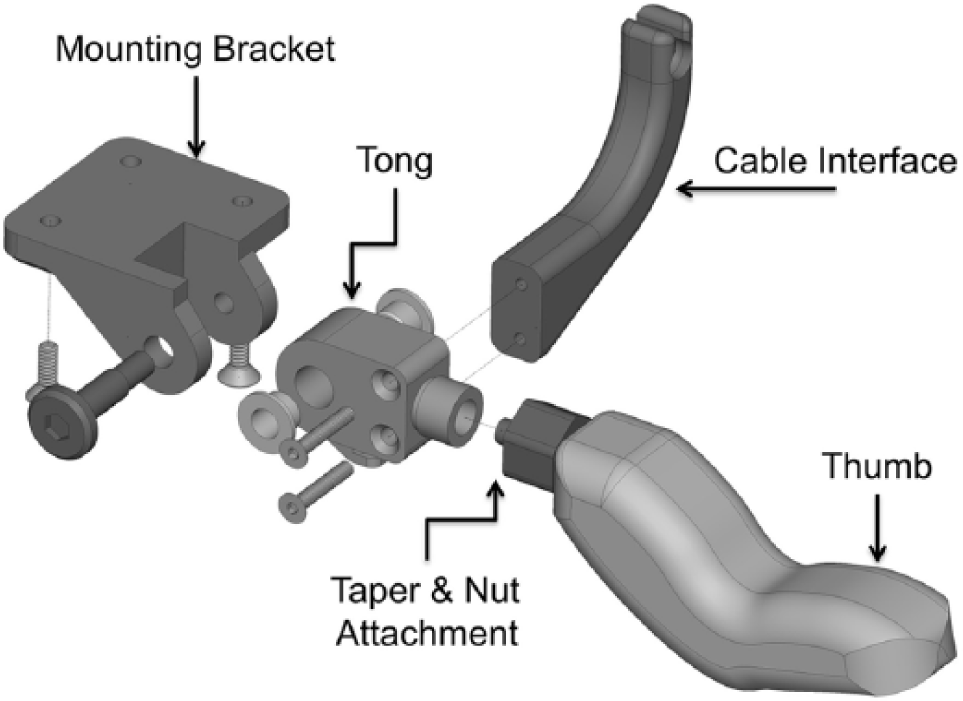
CAD representation of initial prosthesis design.
The design of this prosthesis was an iterative process which made use of easy-to-adapt materials to enable user- and clinician-driven prototype development with fast turnaround. Each prototype was designed using Solidworks CAD software and manufactured using a Stratasys uPrint SE Plus 3D Printer with Fused Deposition Modeling style printing and ABS Thermoplastic. The thumb was mounted to a Vivak test socket and fabricated using standard prosthetic techniques for patient training and evaluation. These materials made it possible for the prototype to be easily sanded down, re-shaped, or re-printed quickly. For minor alterations, changes could be made during the occupational therapy sessions to quickly evaluate the function of new features. The final mechanism was fabricated for delivery out of 7075-T6 aluminum metal (see progression of prototype development in Figure 3). This material was chosen for its strength, wear and corrosion resistance, light weight, and ease of manufacturing as compared to steel. The mechanism was mounted to a laminated carbon socket with a pelite lining for protection to the arm and hand. Due to limitations in wrist and finger strength, and impaired sensation, the socket was designed to extend up the forearm and contain most of the fingers.
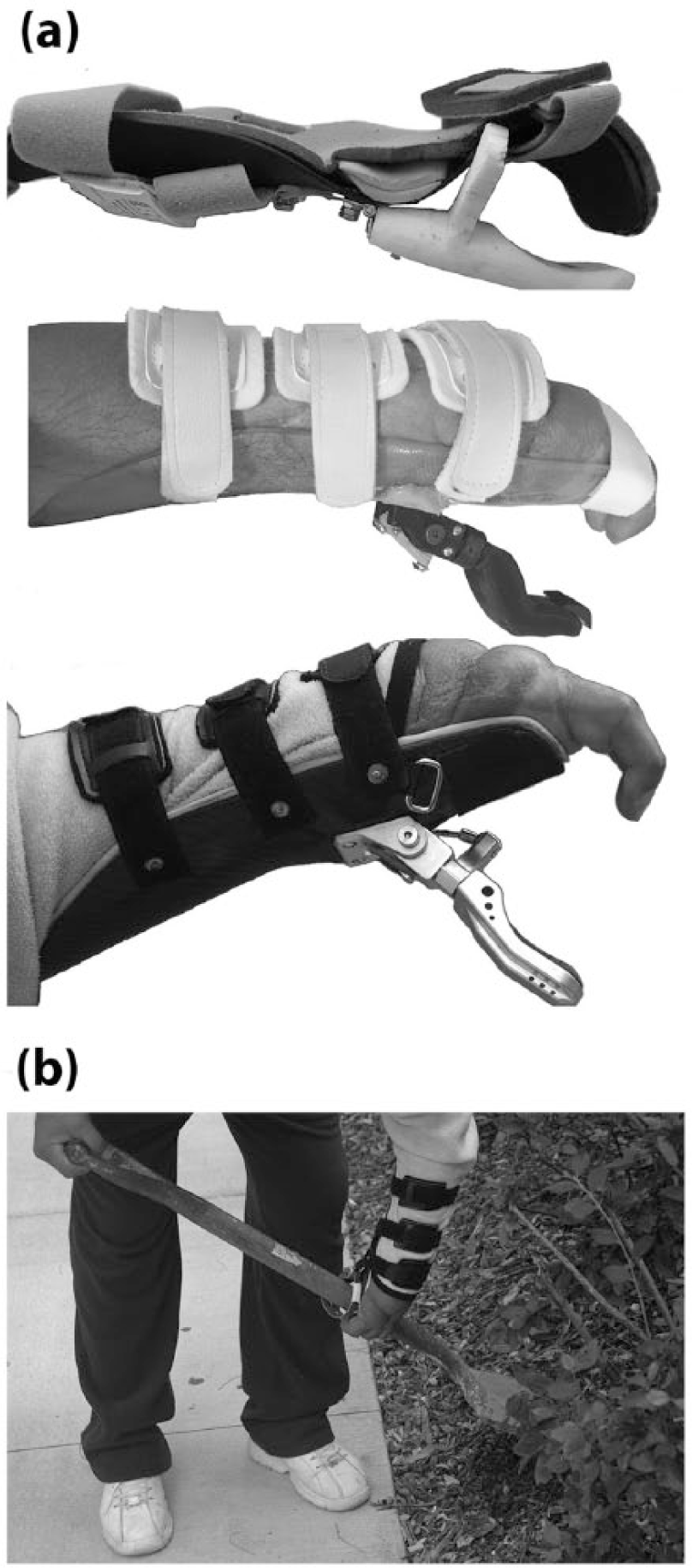
(a) Progression of prototype development and (b) custom hook in use.
Findings and outcomes
Patient application and outcomes
Delivery and training with each new prototype allowed for further refinement of the design aimed at optimal functionality specifically tailored for this patient. The original contour of the thumb did not have an ideal finger pad shape for holding objects as it was too rounded and stiff. This was replaced with a more compliant fingertip material made from RTV Urethane (Smooth-On Vytaflex® 30 Shore A) which was custom molded using three-dimensional (3D) printing technology. The new urethane fingertip allowed for a more frictional gripping surface and compliance which more accurately replicated the compliant behavior of a fingertip. The proximal bend in the original thumb made it difficult to grasp cylindrical objects because it did not provide enough surface area. This shape was removed and replaced with a scoop shape (see Figure 3). The taper and nut attachment at the tong and thumb interface allowed for fine rotational positioning of the thumb, a feature which allowed the patient to rotate the thumb passively to achieve the best grip on a variety of items. A Sure-Lock Cable System (TRS, Inc.) and a TRS rapid adjust buckle were added to the harness system to better accommodate the patient’s use of the device.
To evaluate the effectiveness of the device, the patient participated in the outcome measurements of the Box and Blocks Test and the Patient-Specific Functional Scale (PSFS). The PSFS is used to measure a person’s ability to perform specific self-identified tasks. Patients rate their ability to perform a task on an 11-point scale. Zero means they are unable to complete the task, and 10 means they perform the same as they did prior to their change in function. At initial evaluation, the patient identified the goals of gardening with a shovel, holding items during cooking, and cleaning, specifically wringing a mop. He rated all these items at zero (unable to perform). After three therapy sessions and modifications to the device, the patient rated all as five (moderate difficulty). This indicates a clinically significant improvement of upper extremity function. 3
The Box and Blocks Test assesses manual dexterity by counting the number of blocks a patient can move from one side of a box, over a barrier, to the other side of the box. 4 Using the device, the patient was able to move 23 blocks in the 1-min time allowance. Prior to receiving the device, the patient was unable to be tested using the Box and Blocks test due to the inability to grasp items with that hand. Additionally, the patient expressed a desire to return to fishing, which was addressed by providing a build-up of foam on the fishing rod handle. Many of the patient’s goals remained difficult to perform due to lack of strength in his remaining fingers, making continuous grasping of heavier objects challenging. We were able to find a solution by attaching another hook to the device for ease of use with handle-shaped objects. This additional component could be easily strapped on when needed for these heavier duty tasks and removed when not needed. The use of the adaptive hook allows for more efficient work outdoors with the shovel, a rake and a wheelbarrow, as shown in Figure 3.
Discussion
Individuals with partial-hand amputation are in need of more innovative and customized interventions in order to return to the highest level of function possible. Rapid prototyping and 3D printing technology has become more accessible, which makes it easier to iterate a design and provide custom solutions for patients with difficult cases of prosthetic management. However, 3D-printed plastic was not strong enough for the final device which was made out of aluminum.
In this case, a key element of our design was that the patient could feel what he was grasping with his fingertips. The lack of sensory feedback is one critical element for the rejection of a prosthetic device. 5 With the PSFS test, the patient rated his ability to perform his chosen tasks at zero when using only his impaired hand. Using the new prosthetic thumb, he could do these tasks, but still rated them as moderately difficult. Based on the simple outcome measures we tested, the patient demonstrated an improvement in function, but it is difficult to quantify the improvement in this case since the patient, understandably, rejected the traditional Handy Hook prosthesis. Thus, we had no device with which to compare the Box and Blocks Test, and he could not move blocks without a device.
Our iterative approach was necessary to both optimize the design and better understand the patient’s needs. The ability to rapidly build functional plastic models was critical to the process as many changes were made to this novel thumb design.
As we entered the final development stages of the design with the patient, it became clear that our patient may still not have fully understood his needs for the device, specifically the need for holding heavier objects that his remaining fingers were unable to support physically. Though this device did meet some of the patient’s needs, the fact that the patient had never used a prosthetic device, combined with cultural and language barriers, may have contributed to a general lack of understanding of the patient’s expectations. Although the custom thumb prosthesis proved to be durable and reliable, the patient no longer uses the device due to the lack of strength of his residual fingers. He has since been fit with an i-digits system (first finger and thumb) from Touch Bionics, which provides a more secure grasp used for holding items during household tasks such as cooking and sweeping. However, the heavier duty tasks (shoveling, using a wheelbarrow, etc.) are still challenging due to the physical limitations of his residual limb.
Conclusion
Access to 3D printing processes, as well as a diverse design team, can aid in the development of a custom prosthesis in difficult cases of prosthetic management such as partial-hand amputation. Custom prostheses are becoming more readily available due to easy access to open-source models on platforms such as GrabCAD and the growing popularity of 3D printing. Rising popularity of these prototyping machines not only allows for easier manipulation of a design or mechanism, but the materials available for 3D printing have also become more varied and useful. Combining this easy-to-adapt design process with a diverse treatment team allows for device improvement simultaneous with training, therapy, and patient feedback, which may lead to increased use and higher acceptance of the device.
Footnotes
Author contribution
All authors contributed equally in the preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.