
Abstract
This service evaluation assessed the accuracy of estimating arterial partial pressure of carbon dioxide (PaCO2) from end-tidal CO2 (ETCO2) in prehospital suspected traumatic brain injury (TBI) patients requiring mechanical ventilation. Thirty-one cases with paired ETCO2 and emergency department (ED) PaCO2 measurements were analysed. Estimated PaCO2 (ETCO2 + 0.5 kPa) significantly underestimated measured PaCO2, with a mean bias of 1.17 kPa and wide limits of agreement. Nearly half of patients were outside the normocapnic range despite apparently acceptable estimated values. Findings highlight the risk of inadvertent hypercapnia when relying on ETCO2-based estimation alone. Lower ETCO2 targets or point-of-care PaCO2 measurement may improve ventilation accuracy and reduce secondary brain injury.
Keywords
Introduction
Traumatic brain injury (TBI) frequently leads to disruption of cerebral autoregulation, rendering cerebral perfusion pressure (CPP) susceptible to the arterial partial pressure of carbon dioxide (PaCO2). 1 Dysregulated PaCO2 can precipitate cerebral vasoconstriction or vasodilation, thereby altering oxygen delivery, intracranial pressure (ICP) and risking secondary brain injury. 2 In the prehospital environment, direct measurement of PaCO2 is possible using point-of-care testing (POCT), but it is rarely available outside of specialist prehospital critical care teams. End-tidal carbon dioxide (ETCO2) monitoring is therefore used as a surrogate, with current guidance recommending a target ETCO2 between 4.0 and 4.5 kPa to achieve normocapnia (i.e. a correction factor of approximately +0.5 kPa). 3 However, previous studies have shown poor correlation between ETCO2 and PaCO2, with wider gradients associated with increased mortality. 4 This service evaluation aimed to evaluate the accuracy of estimated PaCO2 derived from ETCO2 in patients with suspected TBI managed by the Hampshire and Isle of Wight Air Ambulance (HIOWAA).
Methods
A retrospective evaluation of HEMSBASE (MedicOne Systems) records was conducted from July 20, 2023, to July 20, 2024. Patients with suspected TBI and pre-hospital emergency anaesthesia performed by HIOWAA were included if they had a PaCO2 recorded within 30 min of arrival at University Hospital Southampton. These were compared with the last recorded ETCO2 at handover in the ED. Side-stream ETCO2 sampling was used in all patients (Zoll X-Series Monitor – reported accuracy: 0–38 mmHg (0–5.1 kPa): ±2 mmHg (0.3 kPa); 39–150 mmHg (5.2–20.0 kPa): ±5% + 0.08% mmHg > 38).
Results were reported descriptively, and an inferential analysis was undertaken in R-Studio. Estimated PaCO2 (EstPaCO2) was calculated as ETCO2 + 0.5 kPa. Data normality was assessed using the Shapiro–Wilk test. Group means were compared using a paired t-test. Agreement between measures was assessed using the Bland–Altman test. This service evaluation was reported in line with STROBE reporting guidelines.
Results
A total of 146 records were assessed for eligibility. Of these, 70 had suspected TBI, with a further 44 excluded because no PaCO2 was recorded within 30 min of ED attendance. In total, 31 records were used in the final analysis. The median time between paired samples was 17 min (IQR 12–20 min).
An absolute difference between estimated PaCO2 values and measured PaCO2 values of 1.2 kPa was found (p < 0.001; Table 1). A paired boxplot was used to visually demonstrate the difference between individual values (Figure 1).
Descriptive statistics for estimated PaCO2 (ETCO2 + 0.5 kPa) and measured PaCO2.

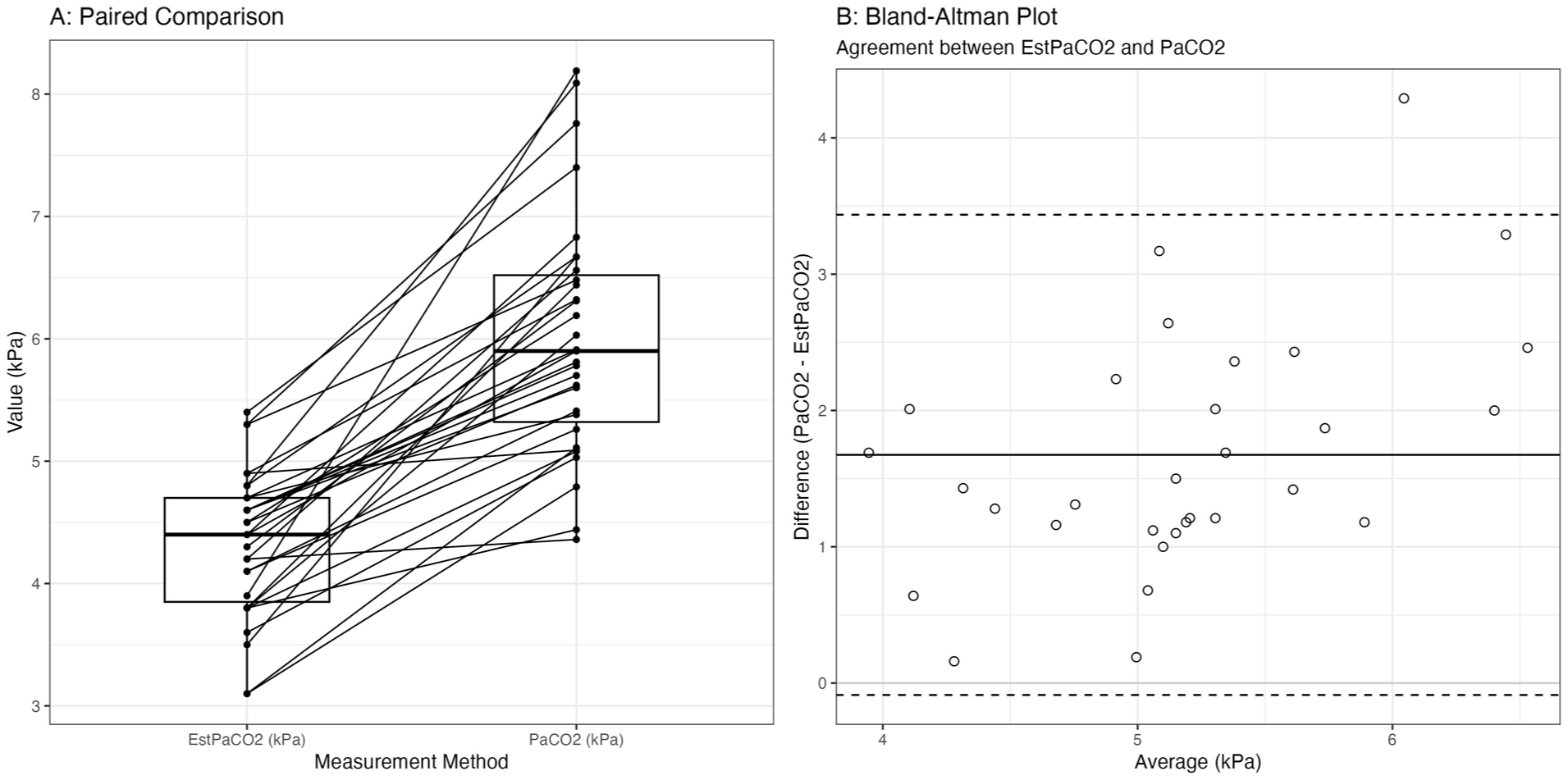
(A) Paired boxplot comparing estimated PaCO2 (EstPaCO2) with measured arterial PaCO2. (B) Bland-Altman plot comparing agreement between EstPaCO2 and PaCO2.
The Bland–Altman bias between EstPaCO2 and measured PaCO2 was 1.17 (95% Limits of Agreement (LOA) 0.84–1.50; Figure 1). The differences are mostly above zero, so measured PaCO2 is, on average, higher than the estimated PaCO2 and shows moderate to wide scatter, with occasional large underestimations.
Discussion
In this study, prehospital ETCO2 significantly underestimates PaCO2 in suspected TBI patients requiring mechanical ventilation, highlighting the potential for unrecognised hypercapnia. Even mildly hypercapnic patients (arrival PaCO2 > 6.53 kPa (49 mmHg)) have been shown to demonstrate worse outcomes in mild to moderate traumatic brain injury. 5 Nearly half (13/31) of patients demonstrated values that were outside the normocapnia range (4.5–6.0 kPa), despite their estimated PaCO2 being within acceptable limits. Given that the measured PaCO2 was on average 1.17 kPa higher than the estimated PaCO2, one option may be to increase the correction factor from +0.5 kPa to a higher value, in the prehospital setting. However, discordance is not linear across all patients, so this may inadvertently cause hypocapnia in those with lower values, which may also be harmful. 6 Only two patients in our study were overestimated (by 0.31 and 0.34 kPa). Factors such as increased dead space ventilation, acidosis, chest trauma and hypotension may contribute to this variation.7–10 Although our evaluation did not account for individual patient characteristics or accompanying injuries, it is possible that these factors contribute to some of the observed variation between Estimated PaCO2 and measured PaCO2. Our study did not examine haemodynamic data, temperature, ventilator settings or changes made during transitions of care, and is also limited by a small sample size (multiple exclusions due to delays in PaCO2 measurement). Nonetheless, the mean bias (>1 kPa) observed is clinically significant. Further work comparing prehospital ETCO2 and PaCO2 using point-of-care testing may better define their relationship in these patients.
Conclusion
ETCO2-derived estimation of PaCO2 may underestimate arterial values in suspected TBI patients in the pre-hospital setting. Lower ETCO2 targets or point-of-care arterial analysis may be required to optimise ventilation prior to arrival at hospital and prevent secondary brain injury.
Footnotes
Acknowledgements
The authors thank Hampshire and Isle of Wight Air Ambulance crews and University Hospital Southampton staff for data access and support.
Ethical considerations
This study met criteria for service evaluation under Hampshire and Isle of Wight Air Ambulance governance and did not require formal ethical approval.
Consent to participate
This study met criteria for service evaluation under Hampshire and Isle of Wight Air Ambulance governance and did not require consent for use of anonymised data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.