
Abstract
Laparoscopy is widely used because it induces minimal postoperative pain and facilitates rapid recovery. However, carbon dioxide (CO2) embolism is a rare but potentially fatal complication of laparoscopic surgery. Earlier reports have shown that decreased end-tidal CO2 (ETCO2) and increased partial pressure of CO2 might be useful indicators of CO2 embolism. We herein report a case of CO2 embolism after the freed bladder neck was released during laparoscopic radical prostatectomy. Sudden hemodynamic disorder and increased ETCO2 combined with immediate arterial blood gas analysis led us to suspect CO2 embolism, which was confirmed by the aspiration of foamy blood from the central venous catheter. The patient was successfully resuscitated and recovered well. This case illustrates that hemodynamic collapse accompanied by increased ETCO2 can indicate CO2 embolism.
Keywords
Introduction
Laparoscopy is widely used in the diagnosis and treatment of gynecological and intra-abdominal diseases. Advantages of this technique include minimal postoperative pain and rapid recovery. However, a serious complication of this technique is gas embolism caused by insufflation, which has a high mortality rate of approximately 28%. 1 A small amount of carbon dioxide (CO2) may enter the circulation through any opening in the injured vessels either at the abdominal wall or the operative site during laparoscopic surgery. Previous reports have shown that decreased end-tidal CO2 (ETCO2) and increased partial pressure of CO2 (PaCO2) might be useful indicators of gas embolism under general anesthesia. 2 We herein report a case of CO2 embolism with hemodynamic collapse as an initial sign during laparoscopic radical prostatectomy. The complication was diagnosed rapidly and managed appropriately.
Case report
A 71-year-old man with a body mass index of 19 kg/m2, American Society of Anesthesiologists physical status of II, medical history of hypertension well managed with nifedipine, and no surgical history was scheduled to undergo laparoscopic radical prostatectomy in March 2018. His echocardiogram showed slight bicuspid and tricuspid regurgitation and decreased left ventricular systolic function. His electrocardiogram showed that the electrical axis had shifted to the left and that the ST-T segment had changed. Other preoperative examinations, including hematological and serum biochemical studies, chest radiography, and pulmonary function tests, revealed no obvious abnormalities.
Therefore, the patient was scheduled for surgery and transferred to the operating room after admission. The radial artery was cannulated and a central venous catheter was placed in the right internal jugular vein. The patient underwent monitoring of his pulse oximetry, tidal volume, airway pressure, body temperature, and urinary output. His blood pressure was 180/80 mmHg and heart rate was 100 beats/minute. The patient was given 1 mg of midazolam intravenously to relieve his anxiety. His blood pressure and heart rate soon dropped to 140/70 mmHg and 90 beats/minute, respectively. General anesthesia was induced with 20 mg of etomidate, 45 µg of sufentanil, and 100 mg of lidocaine; a neuromuscular blockade was achieved with 50 mg of rocuronium bromide. After intubation, the patient received mechanical ventilation under the volume-controlled mode with a respiratory rate of 12 breaths/minute, tidal volume of 6.8 mL/kg, and ETCO2 of 35 to 45 mmHg. Anesthesia was maintained with continuous infusion of propofol (4–7 mg/kg per hour) and remifentanil (0.1–0.2 µg/kg per minute). The patient showed no adverse reactions, and the surgery was initiated.
Several minutes after freeing the bladder neck, the patient’s blood pressure decreased from 140/80 to 100/60 mmHg. Thus, 40 µg of phenylephrine was administered intravenously to improve his blood pressure; however, his hemodynamics remained unstable. The fall in blood pressure was accompanied by tachycardia, with an increase in his heart rate from 80 to 120 beats/minute. Because his ETCO2 remained at 35 mmHg, pulmonary embolism was not taken into consideration. To maintain hemodynamic stability, adrenaline (40 µg) and methylprednisolone (80 mg) were administered intravenously.
Other conditions, such as hemorrhage, heart failure, and pneumothorax, were initially considered. However, there was no evidence to confirm their diagnosis. The estimated blood loss was 100 mL and the urine output was 100 mL, whereas the total fluid infusion volume was 2250 mL. Auscultation confirmed bilateral breath sounds.
A sudden increase in the ETCO2 from 35 to 58 mmHg was accompanied by a decrease in the blood pressure to 52/20 mmHg, and the central venous pressure was 25 cmH2O. Rapid arterial blood gas analysis showed that the fraction of inspired oxygen was 60%, pH was 7.14, and PaCO2 was 91.3 mmHg. The partial pressure of oxygen (PaO2) was 423 mmHg, and the base excess was 2 mmol/L. Considering the above findings, the most probable cause of the hemodynamic collapse and tachycardia in this case was CO2 embolism. The patient was immediately turned to the head-down left-lateral position, and 22 mL of foamy blood was aspirated from the central venous catheter, confirming our diagnosis.
Given his hemodynamic instability, the patient was immediately administered 100% oxygen and continuously infused with high-dose epinephrine (0.1–0.2 µg/kg per minute). Pneumoperitoneum was decreased from 14 to 10 mmHg, and the ruptured vessel was promptly closed.
Five minutes later, a stable hemodynamic condition was achieved with a blood pressure of 130/70 mmHg and decreased ETCO2 of 50 mmHg accompanied by central venous pressure of 14 cmH2O. Another arterial blood gas analysis performed at the end of the surgery showed a pH of 7.33, PaCO2 of 52.3 mmHg, PaO2 of 257 mmHg, and base excess of 1.7 mmol/L. The patient’s heart rate, oxygen saturation, ETCO2, and arterial blood pressure before, during, and after resuscitation are shown in Table 1. The patient was then transferred to the post-anesthesia care unit with an improved condition and stable vital signs. He was extubated in the post-anesthesia care unit with no complications.
Heart rate, SpO2, ETCO2, and arterial blood pressure before, during and after resuscitation.
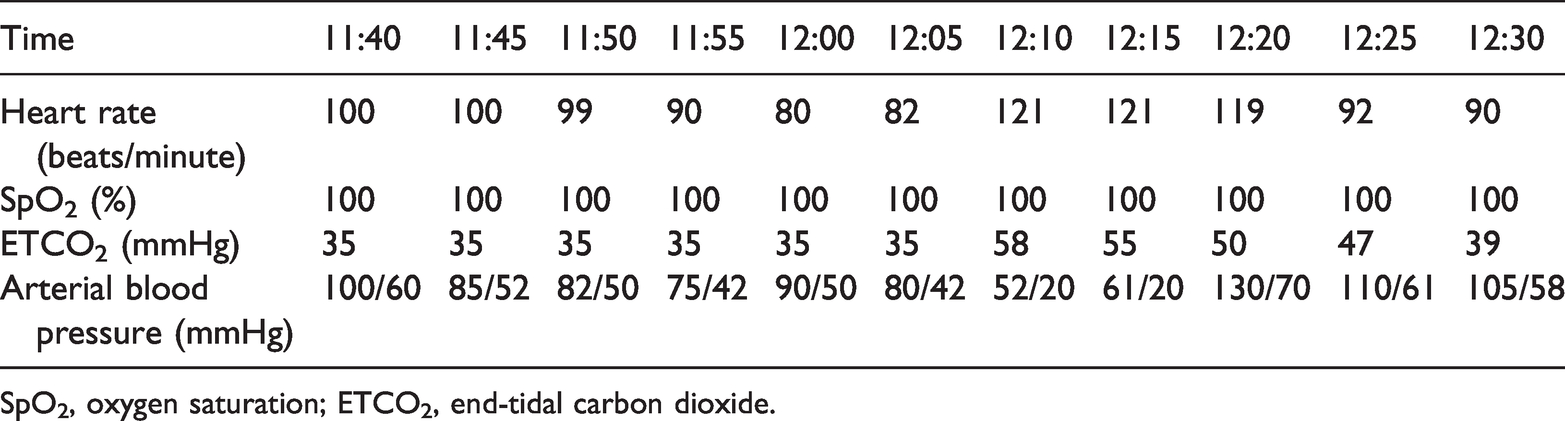
SpO2, oxygen saturation; ETCO2, end-tidal carbon dioxide.
Discussion
Laparoscopic techniques are widely used in radical prostatectomy. However, such techniques can damage Santorini’s venous plexus and the blood vessels on the side of the bladder during the surgery, providing access for CO2 to enter the systemic circulation. Thus, laparoscopic surgery may result in CO2 embolism. 3 In 2009, Kim et al. 4 reported the incidence of CO2 embolism during total laparoscopic hysterectomy using transesophageal echocardiography (TEE). The authors observed gas emboli in all patients, and 37.5% of these emboli occupied more than half the diameter of the right atrium, right ventricle, and right ventricular outflow tract. 4 Moreover, many cases of CO2 embolism have been reported in the past,5–7 indicating an underestimated incidence of CO2 embolism by anesthesiologists and surgeons.
CO2 embolism obstructing the right chamber of the heart and pulmonary artery can be a potentially fatal anesthetic complication during laparoscopic surgery. The clinical manifestations of CO2 embolism depend on the rate and volume of CO2 entrapment and the patient’s condition. According to case reports of accidental intravascular air delivery, the lethal volume for adults is 200 to 300 mL or 3 to 5 mL/kg. Additionally, as shown in this case, the heart might be able to withstand a larger quantity of air over a prolonged period as long as the entrainment is slow. 8
Indicators of gas embolism during general anesthesia are decreased ETCO2, hypoxemia, hypercapnia, high airway pressure, and hemodynamic change. The initial manifestation in the present case was hemodynamic deterioration and tachycardia; however, the ETCO2 did not simultaneously decrease. Therefore, CO2 embolism was not initially considered. A significant increase in PaCO2 detected by arterial blood gas analysis leads to a rapid and accurate diagnosis of CO2 embolism and appropriate hemodynamic management.
CO2 embolism can occur during peritoneal insufflation in laparoscopic radical prostatectomy. Embolization should always be suspected when CO2 insufflation is followed by abrupt hemodynamic disorder and increased PaCO2, regardless of any change in ETCO2 (which may initially increase). The monitoring is nonspecific. 9 Furthermore, the changes in ETCO2 can be easily missed in the operating room because they occur rapidly within a short duration. 10 Apart from ETCO2 monitoring, TEE is the most sensitive method for detecting CO2 embolization. 11 TEE can detect a minimum of 0.02 mL/kg of intravenously injected CO2. 12 Additionally, in patients with cardiac diseases or hemodynamic instability, a central venous catheter should be inserted to monitor hemodynamics and remove gas emboli from the right atrium when suspected. 13
Prompt diagnosis and accurate treatment are imperative to improve the prognosis in cases of CO2 embolization. The basic treatments include immediate cessation of CO2 insufflation, hyperventilation with an inspired oxygen fraction of 1.0, and inotropic support of hemodynamic function. 14
In conclusion, this case shows that co-occurrence of severe hypotension and tachycardia may indicate CO2 embolism even if the ETCO2 does not decrease. Hence, we recommend intraoperative arterial blood gas analysis in cases of hemodynamic collapse and tachycardia during laparoscopy. Prompt diagnosis and accurate treatments are imperative for improving the prognosis if CO2 embolism occurs.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
The patient provided written informed consent, and the study was approved by the First Affiliated Hospital, Zhejiang University, School of Medicine.
Funding
This work was supported by the Bethune Charitable Foundation (BCF-RF-WSQZTZJ-202011-031) and the National Key Research and Development Program of China (Grant No. 2018YFC2001905).