
Abstract
Objective
To investigate the correlation between the pain rating index (PRi), which is an index derived from processed electroencephalography signals, and the end-tidal sevoflurane concentration (ETsevo).
Methods
This study involved 50 adults with a body mass index of 18 to 25 kg/m2 who were undergoing elective surgery under general anesthesia. Thyrocricocentesis was performed with 2.5 mL of 2% tetracaine for endotracheal surface anesthesia, and intravenous injections of midazolam, etomidate, and rocuronium were then administered. The patients’ tracheas were intubated and their ventilatory rate was adjusted to maintain the partial pressure of end-tidal carbon dioxide at 30 to 35 mmHg. Anesthesia was maintained with sevoflurane. The ETsevo was adjusted to maintain anesthesia at 0.6, 0.8, 1.0, and 1.2 minimum alveolar concentration for 15 minutes each, and the PRi, mean arterial pressure (MAP), and heart rate were recorded at each concentration.
Results
A negative correlation was found between the PRi and ETsevo (−0.882) and between the MAP and ETsevo (−0.571). A low positive correlation was found between the PRi and MAP (0.484).
Conclusions
The PRi showed a high negative correlation with the ETsevo. Therefore, the PRi can be used to guide the depth regulation of sevoflurane anesthesia.
Keywords
Introduction
Identifying the minimum effective dose of anesthetic drugs under accurate regulation of the anesthetic depth is of interest to anesthesiologists and can help optimize the use of anesthetic drugs, maintain hemodynamic stability, improve the quality of anesthesia, and reduce complications. 1
The minimum alveolar concentration (MAC) is an important indicator of the potency of volatile anesthetics required to produce immobility and avoid intraoperative awareness. Therefore, the MAC has been used as the standard parameter for determining the depth of general anesthesia when using volatile anesthetics.2,3
The pain rating index (PRi) is a new parameter based on wavelet analysis during general anesthesia. 4 Su et al. 5 found that the PRi reflected the change in perioperative nociceptive stimulation and that this change was consistent with the process of nociceptive stimulation during general anesthesia, suggesting that the PRi has guiding significance in the evaluation of a patient’s reaction to nociception while under general anesthesia. Wu et al. 6 suggested that the PRi could be used to predict hemodynamic reactivity after tracheal intubation and skin incision in pediatric patients during general anesthesia. However, no studies have focused on the relationship between the PRi and end-tidal sevoflurane concentration (ETsevo), by which we can more effectively regulate anesthesia. We hypothesized that there is a correlation between the PRi and ETsevo and that the PRi can be used to guide regulation of the anesthetic depth during sevoflurane anesthesia.
Materials and methods
Patients
The present study was approved by the Shanxi Dayi Hospital Ethical Committee (YXLL-2017-005) and was registered in the Chinese Clinical Trial Registry. Written informed consent was obtained from all patients included in this study. Patients were recruited for the study from September 2017 to February 2018. A CONSORT checklist of the patient enrollment and allocation is shown in Figure 1. The inclusion criteria were an age of 40 to 60 years, body mass index of 18 to 25 kg/m2, American Society of Anesthesiology physical status class of I or II, and treatment under general anesthesia. The exclusion criteria were a history of central nervous system or respiratory system disease, problems associated with alcohol or illicit drug abuse, malignant hyperthermia, severe psychiatric problems, and refusal to provide written informed consent.

CONSORT flow diagram.
Monitoring of anesthesia
The standard monitoring procedures included noninvasive blood pressure, pulse oxygen saturation, electrocardiography, partial pressure of end-tidal carbon dioxide, and ETsevo (IntelliVue MX700; Philips, Amsterdam, The Netherlands). The PRi was monitored as follows. First, the skin covering the patient’s forehead and mastoid was degreased with alcohol. Subsequently, electroencephalographic (EEG) electrodes belonging to a multifunction combination monitor (HXD-I; Beijing Easymonitor Technology, Beijing, China) were placed on the forehead 2 cm above the midpoint between the eyebrows. The reference electrodes were placed on the bilateral mastoid. The electrode impedance was kept below 7.5 kΩ as required by the manufacturer to ensure optimal contact.
The baseline PRi, mean arterial pressure (MAP), and heart rate (HR) were defined as the average of three consecutive measurements recorded immediately after the patients’ arrival in the operating room and before anesthesia induction.
Calculation of PRi4,7
Under the sampling frequency, sampling accuracy, and time window of the collected EEG signals, a vector set of each waveform signal was generated by discrete processing according to the literature. 4
Method of anesthesia
After the patients entered the operating room, 10 mL/kg of sodium lactate was rapidly injected into a peripheral vein of the upper limb. Thyrocricocentesis was performed with 2.5 mL of 2% tetracaine for endotracheal surface anesthesia, and intravenous injections of midazolam (0.05 mg/kg), etomidate (0.3 mg/kg), and rocuronium (0.6 mg/kg) were administered to induce anesthesia. The patients’ tracheas were intubated, their lungs were mechanically ventilated with a tidal volume of 8 to 10 mL/kg, and the ventilatory rate was adjusted to maintain the partial pressure of end-tidal carbon dioxide at 30 to 35 mmHg.
Anesthesia was maintained with sevoflurane (Maruishi Pharmaceutical Co., Ltd., Osaka, Japan). The PRi, MAP, and HR were recorded at each concentration after ETsevo and were adjusted to maintain anesthesia at 0.6, 0.8, 1.0, and 1.2 MAC for 15 minutes each.
The operation began after the data were collected, and 0.5 μg/kg sufentanil was intravenously injected.
Outcome measures
The primary purpose of this study was to determine whether a correlation exists between the PRi and ETsevo. The secondary outcome was to investigate whether any correlations exist between the MAP or HR and the ETsevo or PRi.
Statistical analysis
Quantitative data are presented as mean ± standard deviation. A Pearson correlation was adopted when the correlation analysis data were normally distributed; otherwise, a Spearman correlation was adopted. The repeated-measure data were compared by analyzing the variance of repeated measurements. A P value of <0.05 was considered statistically significant. The statistical analysis was performed using the statistical software IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Patients’ baseline clinical characteristics
Of 60 patients scheduled for elective general anesthesia, 3 declined to participate and 7 did not meet the inclusion criteria (age of >60 years, n = 2; age of <40 years, n = 1; and body mass index of >25 kg/m2, n = 4). Therefore, 50 patients were initially enrolled in this study. A further three patients were excluded because of a PRi of >70 when adjusting the ETsevo to 1.2 MAC (Figure 1). The demographic and clinical data are shown in Table 1.
Demographic and clinical data.
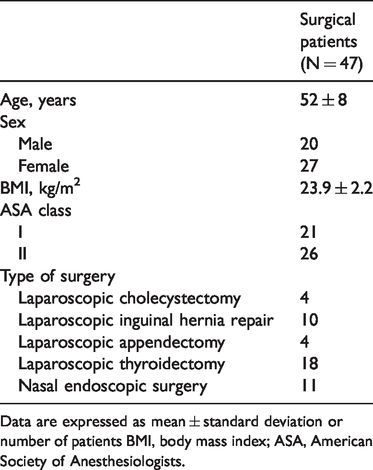
Data are expressed as mean ± standard deviation or number of patients BMI, body mass index; ASA, American Society of Anesthesiologists.
Correlation of PRi, MAP, and HR with ETsevo
The correlation coefficient r between the PRi and ETsevo was −0.882 (P < 0.001), indicating a high negative correlation (Table 2). The correlation scatter plot between the PRi and ETsevo is shown in Figure 2(a).
Correlation of PRi, MAP, and HR with ETsevo.

PRi, pain rating index; MAP, mean arterial pressure; HR, heart rate.

Correlations among parameters and distribution of PRi. (a) Correlation scatter plot between PRi and ETsevo. (b) Correlation scatter plot between MAP and ETsevo. (c) Correlation scatter plot between PRi and MAP. (d) Distribution of PRi at different ETsevo values.
The correlation coefficient r between the MAP and ETsevo was −0.571 (P < 0.001), indicating a moderate negative correlation (Table 2). The correlation scatter plot between the MAP and ETsevo is shown in Figure 2(b).
The correlation coefficient r between the HR and ETsevo was −0.046, indicating no correlation (Table 2).
Correlation of MAP and HR with PRi
The correlation coefficient r between the PRi and MAP was 0.484 (P < 0.001), indicating a low positive correlation. The correlation scatter plot between the PRi and MAP is shown in Figure 2(c).
The correlation coefficient r between the PRi and HR was −0.074, indicating no correlation.
PRi, MAP, and HR at different ETsevo values
The distributions of the PRi at different ETsevo values are shown in Figure 2(d), and the changes in the PRi, MAP, and HR at different ETsevo values are outlined in Table 3.
Changes in PRi, MAP, and HR at different ETsevos.
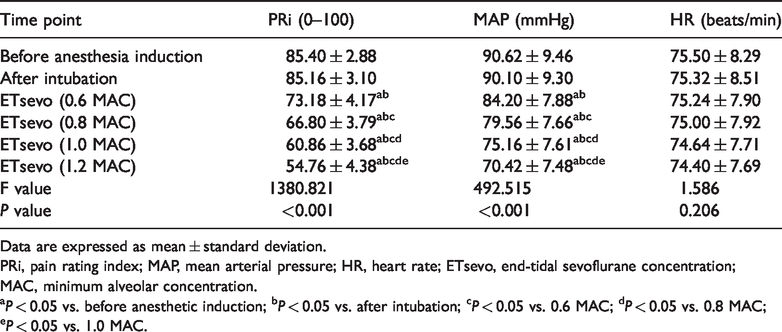
Data are expressed as mean ± standard deviation.
PRi, pain rating index; MAP, mean arterial pressure; HR, heart rate; ETsevo, end-tidal sevoflurane concentration; MAC, minimum alveolar concentration.
aP < 0.05 vs. before anesthetic induction; bP < 0.05 vs. after intubation; cP < 0.05 vs. 0.6 MAC; dP < 0.05 vs. 0.8 MAC; eP < 0.05 vs. 1.0 MAC.
The differences in the PRi between different time points were statistically significant (F = 1380.821, P < 0.001). There was no significant difference in the PRi between before anesthetic induction and after intubation. All PRi values at different ETsevos were lower than before and after anesthetic induction (P < 0.05), though they gradually decreased as the ETsevo increased in the range of 0.6 to 1.2 MAC. There were significant differences in the PRi at different steady-state ETsevos (P < 0.05).
The differences in the MAP between different time points were statistically significant (F = 492.515, P < 0.001). There was no significant difference in the MAP between before anesthetic induction and after intubation. All the MAP values at different ETsevos were lower than before and after anesthesia induction (P < 0.05), but as the ETsevo increased, the MAP gradually decreased. There were significant differences in the MAP at different steady-state ETsevos (P < 0.05).
There were no significant differences in the HR between different time points (F = 1.586).
Discussion
The MAC is an important indicator of the potency of volatile anesthetics and is useful in estimating the depth of volatile anesthetics. Wang et al. 8 showed that ETsevo monitoring during endoscopic surgery reduced the incidence of intraoperative awareness in patients undergoing general anesthesia. The depth of inhalation anesthesia mainly depends on the concentration of the inhaled anesthetics in the brain tissue. When the concentration of the inhaled anesthetics reaches a balance among the alveoli, arterial blood, and brain tissues, the concentration of alveolar gas directly reflects their concentration in the brain tissue. Usually, around 15 minutes are required for the concentration of anesthetics to reach a balance among the alveolar gas, brain tissue, and arterial blood.9,10 Therefore, in the present study, data were only recorded after meeting the steady-state period of ETsevo (defined as the condition in which a constant ETsevo is maintained without vaporizer adjustment for a minimum of 15 minutes) to accurately reflect the anesthetic depth of the inhaled anesthetics.
This study showed that the PRi gradually decreased as the ETsevo increased in the range of 0.6 to 1.2 MAC. Furthermore, there were significant differences in the PRi at different steady-state ETsevos. In the trend analysis of the correlation scatter plot between the PRi and ETsevo, the points were relatively densely distributed. More points were distributed on or around the fit line, which indicated a high correlation between the PRi and ETsevo. The Spearman correlation analysis showed a high negative correlation (r = −0.882) between the PRi and ETsevo. These results suggest that the PRi can be used to guide the depth regulation of sevoflurane anesthesia.
The PRi is a new parameter for assessing nociception based on wavelet analysis during general anesthesia. 4 The PRi mainly extracts EEG metadata of repeatable and regular changes in high- and low-frequency rhythms associated with pain signals and specifically reflects the degree of tolerance to pain stimulation in the cerebral cortex and subcortical center.4,11–13
Age is the principal factor influencing the MAC.
14
The MAC decreases with age. The MAC of sevoflurane is 2.1% at the age of 40 years, 1.7% at 60 years, and 1.4% at 80 years.
15
In light of this, the MAC of sevoflurane was adjusted using the following formula in the present study16–18:

Perioperative surgical stimulation is the main factor involved in PRi fluctuation. In this study, data were collected without surgical stimulation to ensure that the operative conditions were closer to the ideal conditions for estimating the relationship between the ETsevo and PRi.
Endotracheal intubation can cause a high stress response with extensive catecholamine secretion, which results in a series of hemodynamic changes such as hypertension and tachycardia.19,20 Opioids are routinely administered to inhibit the stress response of endotracheal intubation during anesthetic induction. The use of opioids can affect the anesthetic depth measurement and has significant synergism with sevoflurane.21–24 Therefore, opioids were not used during anesthetic induction in the present study, and thyrocricocentesis for endotracheal surface anesthesia was performed to inhibit the stress response to endotracheal intubation. We found no significant differences in the PRi, MAP, or HR before anesthetic induction and after intubation, allowing us to rule out the interference of anesthetic induction and endotracheal intubation on the PRi and hemodynamics.
This study has several limitations. First, the PRi changed greatly and transiently, limiting its use in guiding clinical drug regulation. This also affects the clinical application of the PRi in regulation of the anesthetic depth; thus, continuous improvement in monitoring parameters is required. Second, this study was an exploratory single-center study with a small sample size, and the generalizability of the findings is unknown. Well-designed multicenter clinical trials are needed to evaluate the application value of the PRi. Third, we only explored the correlation between the PRi and ETsevo under nonsurgical stimulation. Subsequent studies should evaluate the feasibility of using the PRi for depth regulation of sevoflurane anesthesia under surgical stimulation.
In conclusion, the PRi showed a high negative correlation with the ETsevo. Therefore, the PRi can be used to guide the depth regulation of sevoflurane anesthesia.
Footnotes
Acknowledgements
The authors acknowledge and thank the anesthesiologists, surgeons, operating room staff, and recovery room staff of the Shanxi Bethune Hospital, Taiyuan, Shanxi, China for their assistance in this research. The authors also thank Yongliang Feng, MD and Ruifeng Liang, MD of Shanxi Medical University, Taiyuan, Shanxi, China for their assistance with the statistical analysis. Beijing Easymonitor Technology, Co., Ltd. (Beijing, China) provided the HXD-I multifunctional monitor but had no role in the study design, data collection, or data analysis.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key Research and Development (R&D) Projects of Shanxi Province, Taiyuan, China (201803D31135).