
Abstract
Accurate estimation of right atrial pressure (RAP) is crucial in cardiogenic shock, yet echocardiographic surrogates are often unreliable. In this exploratory analysis of 43 patients with ischaemic cardiogenic shock, pulmonary artery catheter–derived RAP was compared with right heart echocardiographic indices. Only right ventricular e’ velocity demonstrated a weak correlation with RAP (rho = 0.31, p = 0.04), but did not significantly discriminate elevated pressure. Other Doppler and morphometric measures showed no meaningful associations. Echocardiographic parameters correlated poorly with invasive RAP, indicating that conventional indices cannot reliably substitute for pulmonary artery catheterisation in assessing venous congestion in this population.
Keywords
Introduction
Accurate assessment of right atrial pressure (RAP) is central to the management of cardiogenic shock, in which systemic venous congestion worsens renal perfusion, impairs organ recovery, and leads to adverse outcomes. Current echocardiography guidelines recommend the inferior vena cava (IVC) diameter and its respiratory variation as surrogate markers of RAP. 1 However, IVC dimensions are inaccurate, particularly in mechanically ventilated patients, and in some cases, the IVC cannot be adequately visualised.2,3 Right ventricular (RV) diastolic Doppler profiles have been proposed as alternative RAP surrogates, with correlations ranging from strong to poor.4–7 However, their performance in ischaemic cardiogenic shock remains unclear. Establishing a robust correlation between these parameters and invasive RAP could provide a practical, non-invasive alternative. We therefore evaluated the correlation between pulmonary artery catheter (PAC)-derived RAP and RV diastolic Doppler echocardiographic parameters, as well as the right atrial area, in ischaemic cardiogenic shock.
Method
In this exploratory post hoc analysis of a recent study, 8 we examined the correlation between RAP measured via a clinically indicated PAC and simultaneously obtained transthoracic echocardiography parameters in 43 patients with ischaemic cardiogenic shock. The echocardiograms were performed by experienced, accredited critical care physicians (British Society of Echocardiography – BSE, Level 2 or equivalent) in accordance with the BSE guidelines. 9 An experienced, accredited (National Board of Perioperative Echocardiography) critical care physician (AS), blinded to PAC and clinical results, analysed the echocardiograms offline. Echocardiographic measurements were recorded from a typical beat with a stable signal. RAP was measured via PAC as previously described 10 and recorded at the time of echocardiography. 8 Given the exploratory nature of the analysis and the use of non-parametric data, Spearman’s rank correlation was chosen to assess associations between echocardiographic parameters and RAP. Receiver operating characteristic (ROC) analysis was conducted to investigate the accuracy of echocardiographic parameters for detecting RAP at 10 mmHg, consistent with previous studies, and to explore thresholds 2 mmHg above and below this value.4–7 The study was conducted with institutional review board approval.
Results
The cohort’s median age was 61 years (52–67), and 36 (84%) were male. Mechanical ventilation was required in 37 patients (83%), mechanical circulatory support in 22 (52%), and renal replacement therapy in 14 (33%). The median PAC-derived RAP was 12 mmHg (9–15). RV e’ velocity demonstrated a weak but statistically significant correlation (rho = 0.31, p = 0.04, Table 1). No significant correlations were observed for RV E wave (rho = –0.10, p = 0.54), RV A wave (rho = 0.24, p = 0.14), RV E/A ratio (rho = –0.15, p = 0.36), RV E/e’ ratio (rho = –0.25, p = 0.12), RV a’ (rho = –0.13, p = 0.43), or right atrial (RA) area (rho = 0.15, p = 0.37). Despite the weak correlation, RV e’ exhibited no significant discriminatory ability at any RAP threshold. The areas under the curves and confidence intervals for detecting RAP above 8, 10, and 12 mmHg were 0.66 (0.4349–0.8941, p = 0.12), 0.67 (0.4732–0.8729, p = 0.10), and 0.64 (0.4704–0.8166, p = 0.12), respectively.
Echocardiographic parameters and their correlation with pulmonary artery catheter (PAC)-derived right atrial pressure (RAP) in patients with ischaemic cardiogenic shock.
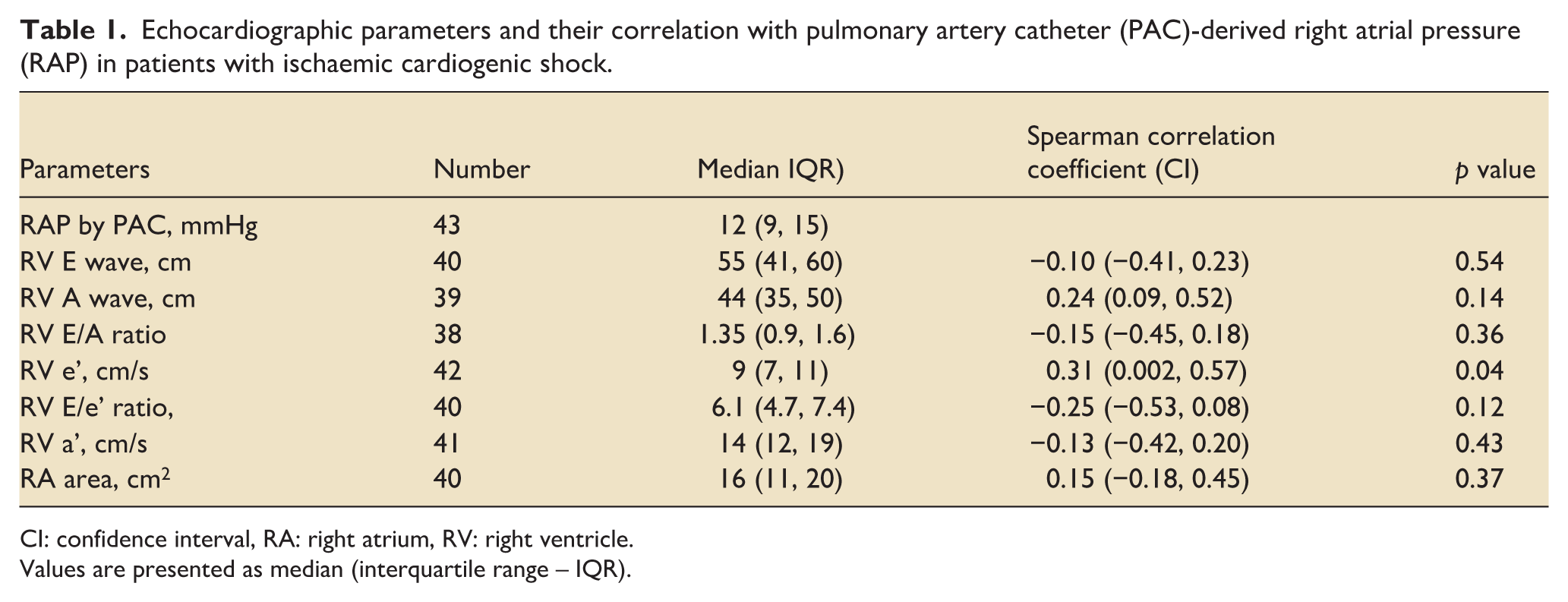
CI: confidence interval, RA: right atrium, RV: right ventricle.
Values are presented as median (interquartile range – IQR).
Discussion
RV diastolic Doppler echocardiographic parameters correlated poorly with PAC–derived RAP in cardiogenic shock. RV e’ velocity showed a weak association with RAP and had non-significant discriminative ability to identify elevated RAP.
Previous studies involving patients with sepsis and non-critically ill patients observed that RV E/e’ and other RV diastolic Doppler echocardiography parameters closely correlated with central venous pressure (CVP), which serves as a surrogate for RAP.4,5 However, in patients with left ventricular dysfunction, these parameters did not correlate with PAC-derived RAP. 6 Similarly, no meaningful correlation was observed in our cardiogenic shock cohort, likely reflecting differences in underlying pathology and measurement technique.
This was a single-centre, post hoc analysis of data originally collected for another study, with PAC insertion guided by clinical need rather than protocol. Advanced echocardiographic parameters, including right atrial strain, 3D volumetry, and splanchnic venous Doppler, were not assessed. IVC imaging was limited by interference from the extracorporeal circuit. Patients were not stratified by RV systolic function due to the small sample size, although variability in RV performance may independently influence RAP. Finally, RAP is a static measure and does not capture dynamic haemodynamic responses, limiting the physiological interpretability.
In this exploratory study, RV diastolic Doppler echocardiographic parameters correlated poorly with PAC–derived RAP in ischaemic cardiogenic shock. Further research is needed to identify reliable non-invasive surrogates for venous congestion in this setting.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.