
Abstract
In this exploratory analysis of 35 patients with ischemic cardiogenic shock, we evaluated the correlation between tricuspid regurgitation velocity (TRV) and pulmonary artery catheter-derived pressures. TRV correlated best with pulmonary artery mean pressure (r = 0.54, p = 0.0009), more than with systolic or diastolic pressures. A TRV threshold of 2.3 m/s identified mean pressure >25 mmHg with 81% sensitivity and 62% specificity. These findings suggest that TRV may serve as a non-invasive indicator of elevated pulmonary pressure in critically ill patients when invasive monitoring is unavailable. Further validation in larger, diverse cohorts is needed.
Keywords
Introduction
Tricuspid regurgitation velocity (TRV) is routinely used to estimate pulmonary artery systolic pressure (PASP) and screen for pulmonary hypertension, with a guideline-endorsed threshold of greater than 2.8 m/s indicating elevated pulmonary pressure. 1 However, TRV represents a peak systolic gradient and may diverge from invasively measured pulmonary haemodynamics in critically ill patients. In cardiogenic shock, where the acuity of illness, low stroke volume, elevated right atrial pressure, and the need for mechanical circulatory support may distort Doppler estimates, the reliability of TRV warrants reevaluation. We conducted a subgroup analysis of patients with pulmonary artery catheters to assess the correlation between TRV and invasive pulmonary pressures and resistance.
Method
In this exploratory subgroup analysis of a recent prospective study, 2 we examined the correlation between pulmonary artery pressures and vascular resistance measured via a clinically indicated pulmonary artery catheter (PAC) and simultaneously obtained TRV by continuous-wave Doppler transthoracic echocardiography in patients with ischaemic cardiogenic shock. The echocardiograms were performed by experienced, accredited critical care physicians (British Society of Echocardiography – BSE, Level 2 or equivalent) in accordance with the BSE guidelines. 3 An experienced, accredited (National Board of Perioperative Echocardiography) critical care physician (AS), blinded to PAC and clinical results and not involved in data collection, analysed the echocardiograms offline. Tricuspid regurgitation (TR) severity was assessed by colour flow Doppler. TRV was available in 35 patients. The highest value, recorded from any suitable echocardiographic window, was used for analysis. Pulmonary artery pressures and vascular resistance were measured as previously described 4 and recorded at the time of echocardiography. Further details of the method can be found in the original study article. 2
Results
The cohort’s median age was 62 years (IQR, 50–67), with 86% of participants being male. Additionally, 49% of patients required mechanical circulatory support. The results are summarised in Table 1. Two patients had moderate or severe TR, while none experienced torrential regurgitation. Using Spearman’s rank correlation, TRV showed statistically significant associations with pulmonary artery systolic pressure (PASP) (r = 0.49, p = 0.004, Figure 1(a)), mean pressure (PAMP) (r = 0.54, p = 0.0009, Figure 1(b)), and diastolic pressure (PADP) (r = 0.47, p = 0.006, Figure 1(c)). The correlation between TRV and pulmonary vascular resistance (PVR) was weaker and non-significant (r = 0.29, p = 0.11, Figure 1(d)). Receiver operating characteristic analysis for detecting pulmonary hypertension (PAMP > 25 mmHg) 1 yielded an area under the curve of 0.72 (p = 0.03). A TRV threshold of 2.3 m/s provided 81% sensitivity and 62% specificity.
Hemodynamic parameters and their correlation with tricuspid regurgitation velocity (TRV) in ischemic cardiogenic shock.
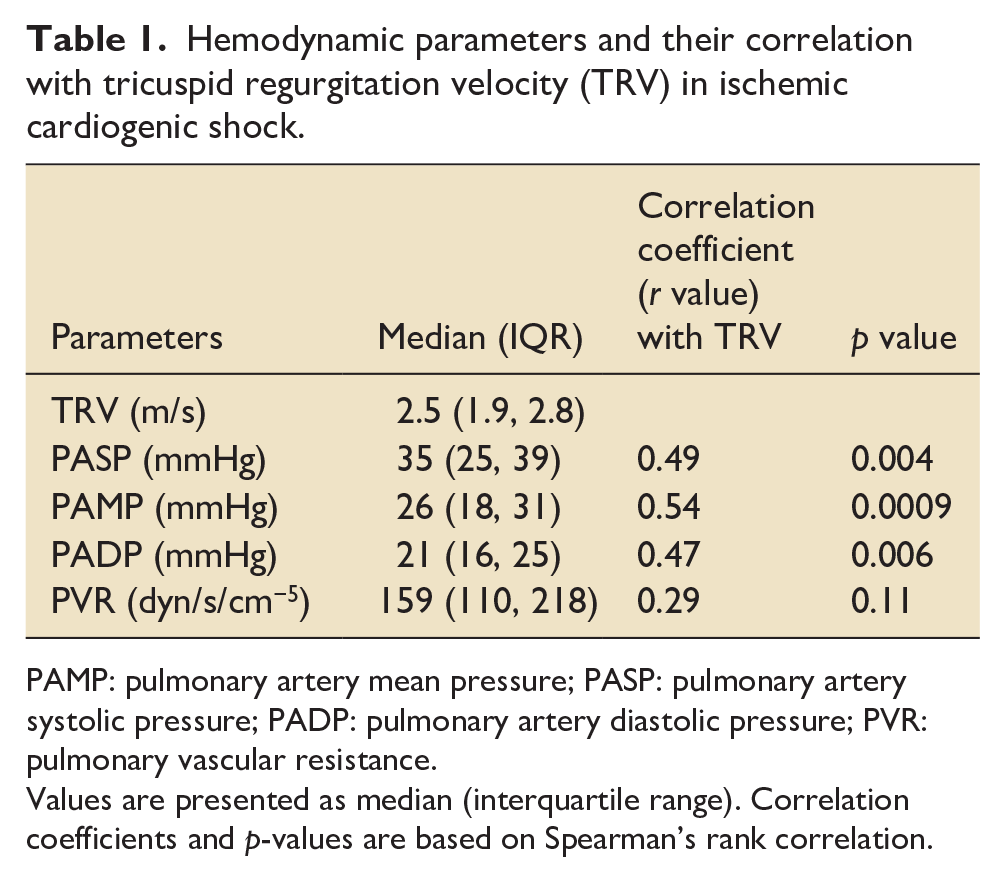
PAMP: pulmonary artery mean pressure; PASP: pulmonary artery systolic pressure; PADP: pulmonary artery diastolic pressure; PVR: pulmonary vascular resistance.
Values are presented as median (interquartile range). Correlation coefficients and p-values are based on Spearman’s rank correlation.
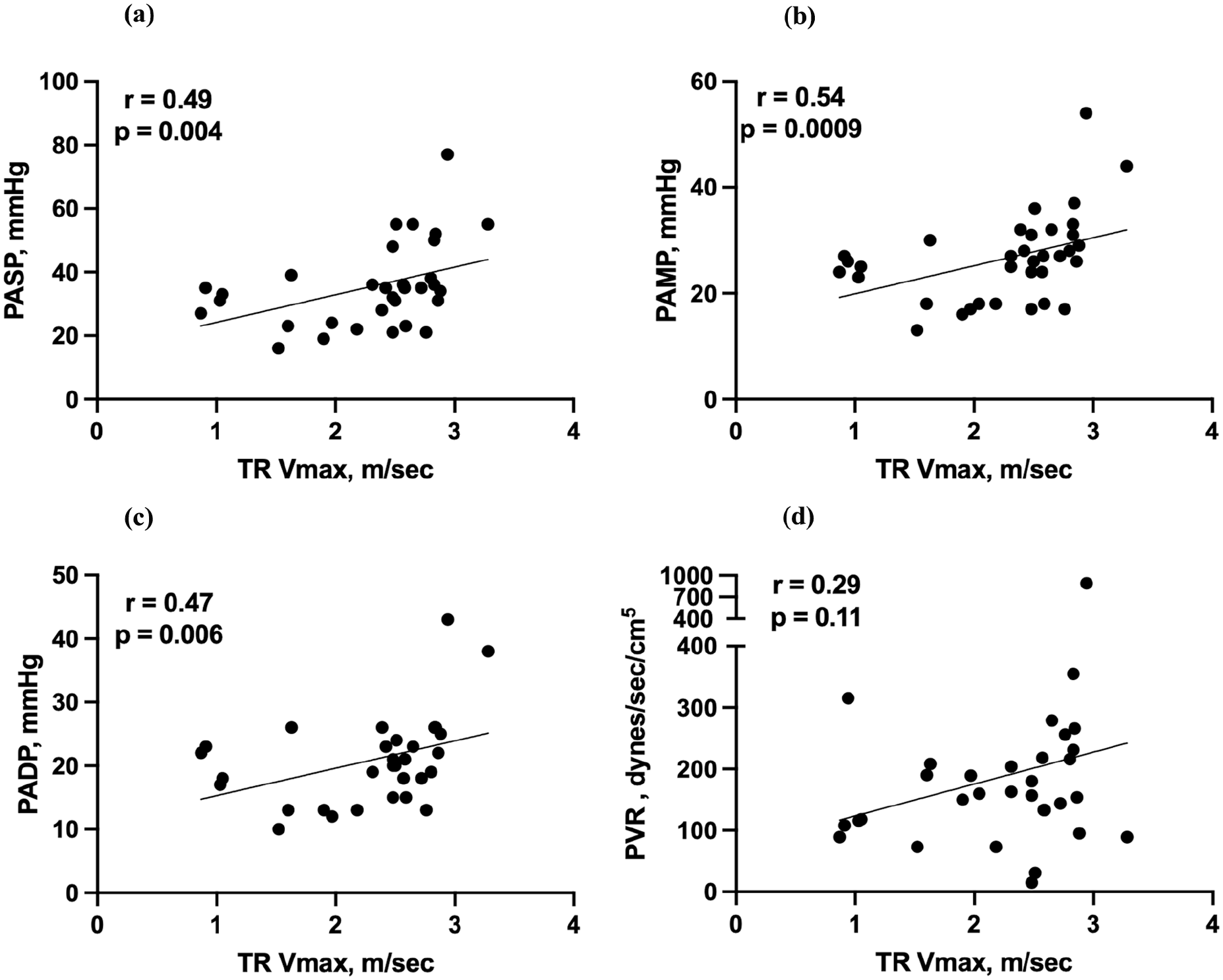
Correlation between tricuspid regurgitation velocity (TRV) and invasive pulmonary artery catheter measurements. Scatter plots demonstrate the relationship between TRV and (a) pulmonary artery systolic pressure (PASP), (b) pulmonary artery mean pressure (PAMP), (c) pulmonary artery diastolic pressure (PADP), and (d) pulmonary vascular resistance (PVR), with Spearman correlation coefficients and p-values shown.
Discussion
This exploratory analysis suggests that TRV in ischemic cardiogenic shock correlates best, albeit moderately, with PAMP, rather than systolic or diastolic pressures. A TRV threshold of 2.3 m/s identified elevated PAMP > 25 mmHg with reasonable accuracy. These findings support the cautious use of TRV as a non-invasive marker of elevated pulmonary pressures in patients with cardiogenic shock when invasive monitoring is unavailable.
The stronger association with PAMP over PASP raises questions about TRV’s conventional interpretation as a surrogate for PASP. In this setting, TRV may reflect post-capillary pulmonary hypertension, shaped predominantly by elevated pulmonary capillary wedge pressure (PCWP) and right atrial pressure (RAP), rather than precapillary resistance. The lower TRV threshold identified here (2.3 m/s) compared to guideline thresholds (2.8 m/s) likely reflects this altered physiology. Elevated RAP in cardiogenic shock reduces the trans-tricuspid pressure gradient, compressing the TRV signal even in the presence of high pulmonary pressures. These observations highlight the limitations of applying outpatient-derived thresholds to critically ill patients.
Our findings align with prior analyses in this cohort, where TRV correlated with PCWP, and a TRV > 2.3 m/s indicated PCWP > 15 mmHg. 5 Additionally, PAMP and PADP were both shown to correlate with PCWP, 6 supporting the interpretation of TRV as an indirect marker of post-capillary RV afterload. This aligns with the physiology of ischemic cardiogenic shock, where pulmonary hypertension is typically passive and driven by elevated left-sided filling pressures rather than pulmonary vasoconstriction.
The study’s limitations include being conducted at a single centre, potential selection bias due to clinical PAC implantation favouring sicker patients, and the absence of TRV measurements in some cases. Two patients in this group exhibited significant tricuspid regurgitation, which could underestimate the pressure gradient between the right ventricle and atrium and influence the correlation results.
In conclusion, TRV offers a readily accessible tool for approximating pulmonary pressure in the absence of invasive monitoring. Its utility in ischemic cardiogenic shock depends on context-specific interpretation, underscoring the need for nuanced application and continued investigation in critically ill populations.
Footnotes
Author contributions
Hazem Lashin: Conceptualisation; Data Curation; Formal analysis; Writing the original draft. Olusegun Olusanya: Conceptualisation; Data Curation: Writing review and editing. Andrew Smith: Conceptualisation; Data Curation; Writing review and editing. Sanjeev Bhattacharyya: Conceptualisation; Supervision; Writing review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.