
Abstract
Accurate stroke volume (SV) assessment is crucial in ischaemic cardiogenic shock. While pulmonary artery catheterisation remains the gold standard, its invasive nature necessitates reliable noninvasive alternatives. However, the literature on echocardiographic SV accuracy is inconsistent. This study evaluated commonly used echocardiographic techniques—Doppler-derived and Simpson’s method—against invasive thermodilution in 39 patients. SV by Doppler showed strong correlation (r = 0.91, p < 0.0001) and minimal bias, whereas the Simpson’s method exhibited weaker correlation and more significant underestimation. These findings suggest Doppler echocardiography as the more accurate noninvasive tool for SV estimation, addressing prior discrepancies and enhancing haemodynamic management in critical care.
Introduction
Accurate measurement of stroke volume is crucial for effective diagnosis and management of haemodynamics in cardiogenic shock. Traditionally, pulmonary artery catheterisation has been deemed the gold standard; however, its invasive nature and associated risks have sparked a demand for safer, noninvasive alternatives. In this context, echocardiography is vital for intensive care practitioners, potentially enhancing patient safety and care. Despite this, the reliability of various stroke volume estimation techniques remains inconsistent. Doppler-based estimations have shown a variable correlation with invasive measurements in critically ill patients.1,2 Moreover, our previous studies have highlighted significant discrepancies in stroke volume estimations when comparing the Doppler technique to the modified Simpson’s method of discs. 3 These findings emphasise the urgent need to reassess the accuracy of noninvasive assessments to improve clinical outcomes in this vulnerable population.
Method
In this subgroup analysis of a recent study, 4 we examined the relationship between native stroke volume, measured by thermodilution via a pulmonary artery catheter, and simultaneously obtained left ventricular echocardiographic parameters in 39 patients with ischaemic cardiogenic shock without significant mitral regurgitation (moderate or more)
Details of the method can be found in the original study article. 4
Results
The patients had a median age of 61 years [52, 67], with 32 (83%) males. Mechanical circulatory support was required in 18 (46%) patients. Remarkably, stroke volume measurements obtained through left ventricular outflow tract (LVOT) Doppler and diameter (SVDoppler) demonstrated a strong correlation by Spearman’s coefficient (r = 0.91, p < 0.0001) with the invasive stroke volume (Table 1). This robust relationship is supported by minimal systemic underestimation bias, quantified at only −3.6 ± 8 ml by the Bland-Altman test, and a clinically acceptable percentage error of 28% (Table 1, Figure 1). 5 Conversely, stroke volume derived using Simpson’s method (SVSimpsons) displayed a weaker correlation (r = 0.71, p < 0.0001) with worse underestimation bias (−11 ± 14 ml) and a percentage error nearly doubling that of SVDoppler (44%, Table 1). Furthermore, the ability of SVDoppler to accurately predict invasive stroke volumes below 60 ml, with an area under the curve (AUC) of 0.91 in receiver operator curve analysis, underscores its superior diagnostic performance compared to SVSimpsons (AUC = 0.84; Table 1 and Figure 1). These findings are especially pertinent given that the LVOT velocity time integral and the global longitudinal strain showed moderate correlations with invasive measurements, whereas ejection fraction did not correlate significantly (Table 1).
Echocardiography results and correlation of echocardiography parameters with the native stroke volume by thermodilution via pulmonary artery catheter in patients with ischaemic cardiogenic shock.
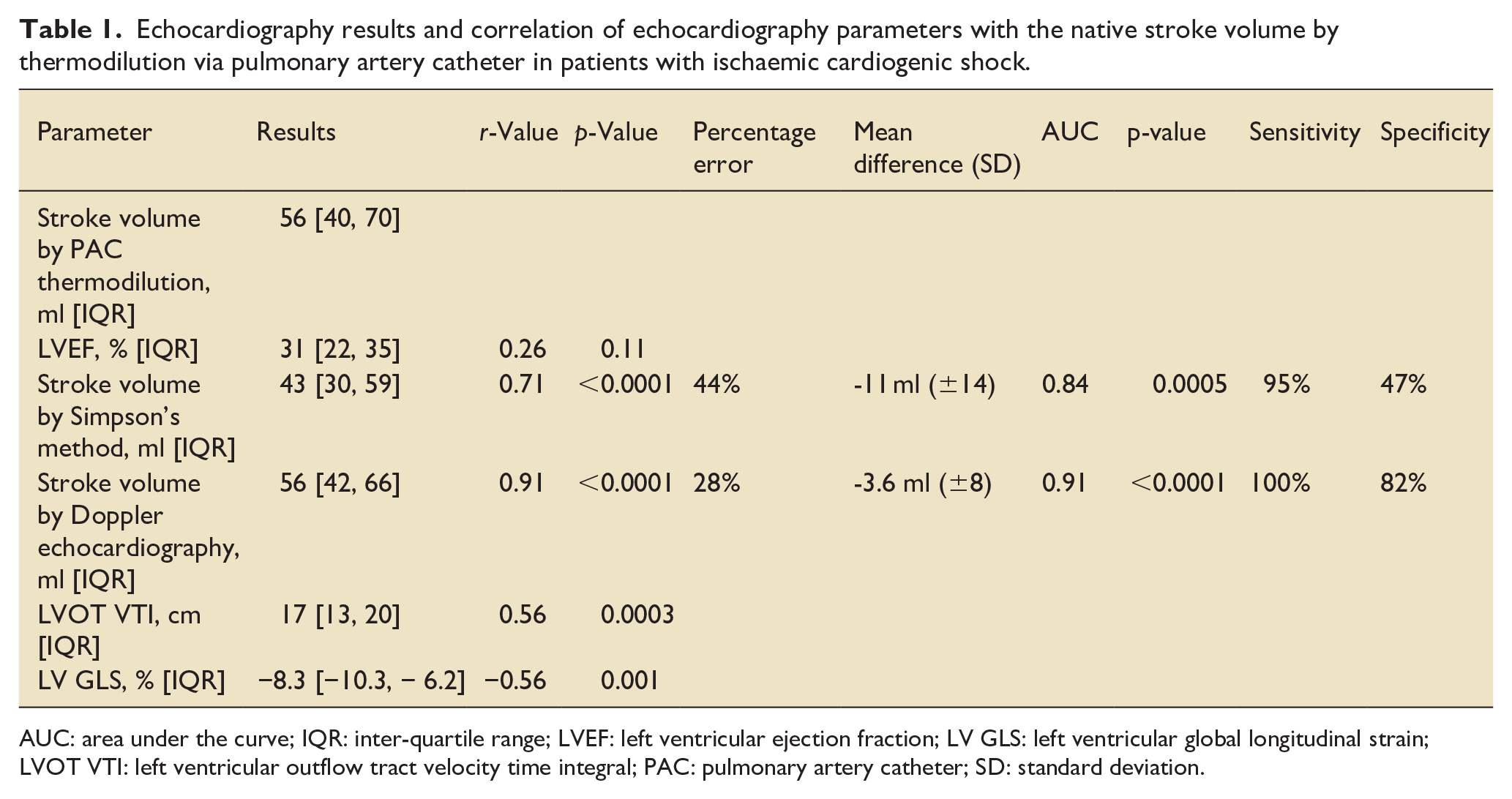
AUC: area under the curve; IQR: inter-quartile range; LVEF: left ventricular ejection fraction; LV GLS: left ventricular global longitudinal strain; LVOT VTI: left ventricular outflow tract velocity time integral; PAC: pulmonary artery catheter; SD: standard deviation.
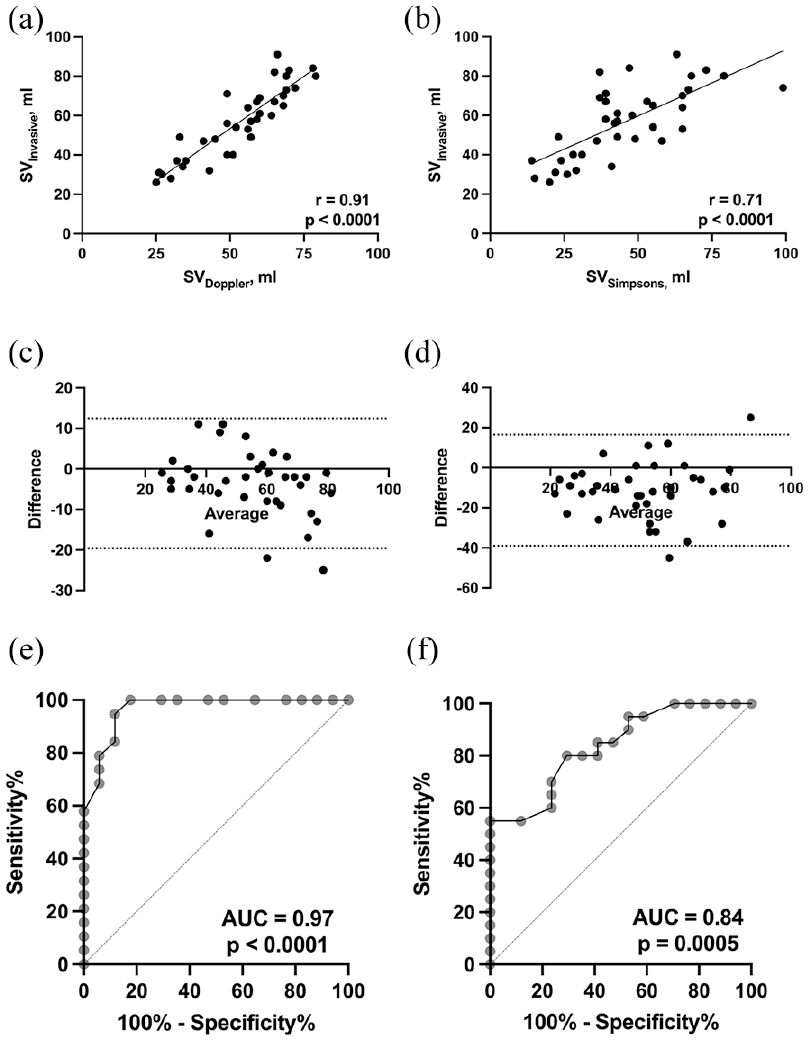
Correlation between invasive stroke volume by thermodilution via pulmonary artery catheter and stroke volume estimation methods by echocardiography in patients with ischaemic cardiogenic shock: (a) correlation between invasive and Doppler stroke volume measurements, (b) correlation between invasive and Simpson’s method stroke volume measurements, (c) Bland-Altman graph for bias of Doppler stroke volume compared to invasive stroke volume, (d) Bland-Altman graph for bias of Simpson’s stroke volume compared to invasive stroke volume, (e) area under the curve (AUC) for Stroke volume by Doppler echocardiography prediction of reduced invasive stroke volume, and (f) AUC for Stroke volume by the modified Simpson’s method of discs prediction of reduced invasive stroke volume.
Discussion
These results consolidate the role of SVDoppler as an accurate, noninvasive tool for clinicians managing patients with ischaemic cardiogenic shock in the absence of invasive monitoring.
It is essential to understand that obtaining accurate SVDoppler readings depends on careful measurements of the LVOT diameter at the insertion points of the aortic valve leaflets, oriented perpendicularly to the long axis of the LVOT. 6 Moreover, the alignment of the Doppler sample volume with less than 20° deviation from the direction of blood flow in the LVOT is vital for precision. By strictly adhering to these technical standards as demonstrated in this study, we can significantly enhance the reliability of SVDoppler readings, ultimately improving outcomes in real-time clinical applications.
Our study deliberately excluded patients with significant mitral regurgitation to uphold the integrity of our measurements and avoid discrepancies between the invasive stroke volume recorded in the right ventricle and the noninvasive measurements obtained through SVDoppler in the left ventricle. Notably, differences between these measurements can provide critical insights into mitral regurgitation volume, significantly enhancing the diagnostic capability of this noninvasive tool and aiding in the identification of cardiogenic shock resulting from severe mitral regurgitation, where invasive stroke volume may appear adequate, yet left ventricular output remains compromised.
SVSimpsons exhibited a weaker correlation with invasive measurements than SVDoppler. This difference may arise from SVSimpsons’ reliance on image quality, which declines with the severity of cardiogenic shock. 7 Furthermore, SVSimpsons concentrates solely on specific regions of the left ventricle. Additionally, the underlying formula assumes that the left ventricle is ellipsoidal. 8 However, this assumption often does not always apply in the context of ischaemic cardiogenic shock, 9 underscoring a significant limitation of this method.
In conclusion, our findings reveal that SVDoppler not only correlates strongly with invasive stroke volume measured by thermodilution through pulmonary artery catheterisation in patients experiencing ischaemic cardiogenic shock without significant mitral regurgitation but also suggests its potential as a vital therapeutic target for enhancing haemodynamic management in this critically ill patient population. This paves the way for further exploration of SVDoppler’s capabilities in tailoring interventions in complex clinical scenarios.
Footnotes
Author contribution
Hazem Lashin: Conceptualisation; Data Curation; Formal analysis; Writing the original draft. Olusegun Olusanya: Conceptualisation; Data Curation: Writing review and editing. Andrew Smith: Conceptualisation; Data Curation; Writing review and editing. Sanjeev Bhattacharyya: Conceptualisation; Supervision; Writing review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.