
Abstract
Objective:
This retrospective observational study conducted in a general ICU aimed to evaluate the hemodynamic impact of IV paracetamol by monitoring blood pressure, urine output, and core temperature post-administration.
Design:
The study was designed as a retrospective observational study in a general ICU setting.
Setting:
The study was conducted in a general intensive care unit (ICU).
Patients:
Data from 498 patients receiving IV paracetamol in various clinical contexts were analyzed.
Interventions:
Patients received IV paracetamol for analgesia and fever reduction as part of their clinical care.
Measurements and main results:
The study analyzed the hemodynamic effects of IV paracetamol by monitoring blood pressure, urine output, and core temperature post-administration. A significant decrease in mean systolic and diastolic blood pressure values was observed across different patient subgroups, notably 45–60 min post-infusion. An increase in noradrenaline dosage and a decrease in urine output indicated a decline in end-organ perfusion following IV paracetamol administration. Multivariate analysis identified associations between clinical factors (such as general anesthesia and cardiac conditions) and changes in blood pressure.
Conclusions:
While IV paracetamol remains a valuable therapeutic option for pain and fever management, especially in hypertensive patients with specific conditions like traumatic brain injury and cerebral vascular accident, careful monitoring, and individualized dosing strategies are recommended in critically ill patients to maintain hemodynamic stability and optimize clinical outcomes. These findings contribute to enhancing our understanding of IV paracetamol hemodynamic effects and inform evidence-based practices for its use in ICU settings.
Introduction
Paracetamol has analgesic and antipyretic effects on the central nervous system. 1 It is most often given to hospitalized patients, including those in critical care units. 2 Due to its efficacy, fast action, and low risk of side effects, paracetamol is a first line treatment for many in the intensive care unit (ICU) and other high-risk clinical settings. However, despite its efficacy and widespread usage, its mechanism of action is not fully understood. Previously, it was thought that paracetamol induces analgesia by inhibiting the enzyme cyclooxygenase. More recently, it has been suggested that the main analgesic mechanism of paracetamol involves its metabolization to N-acylphenolamine, which then acts on specific receptors in the brain and the spinal cord. 3
Intravenous (IV) paracetamol was first introduced in the hospital setting in 1985 and indicated when enteral administration is not possible. 4 Intravenous paracetamol infusion provides onset of pain relief within 5–10 min after the start of administration. The peak analgesic effect is obtained in 1 h and the duration of this effect is usually 4–6 h. Fever is reduced within 30 min after the start of administration, with a duration of the antipyretic effect of at least 6 h. 5
Recently, in the context of critical illness, emerging clinical data has suggested that IV paracetamol may cause hypotension. This may have important clinical implications in critically ill patients where adequate maintenance of hemodynamics reduces the risk of morbidity. Post-IV paracetamol hypotension has been reported in a few small studies. In one study, which included 38 patients in medium care units and ICU, hypotension following IV paracetamol was reported in 22% and 33% after 15 and 30 min after infusion started. 6 Post-IV paracetamol hypotension was also described in cardiac surgery patients. 7 It has also been observed in subarachnoid hemorrhage (SAH) patients when given as an antipyretic agent, 8 and even in healthy volunteers. 9 Another study, conducted with neuro-critically ill patients, demonstrated hypotension induced by IV paracetamol. 10 The findings also indicated that older age and fever are among the risk factors associated with these events. 10 A different study conducted a post hoc analysis to examine the impact of IV paracetamol on postoperative hypoxemia following abdominal surgery and revealed a reduction in mean arterial pressure (MAP) following the IV administration. 11
In one study which included 6 patients monitored by (Picco) pulse contour cardiac output and administrated IV paracetamol showed decreased MAP, decreased cardiac index, and decreased systemic vascular resistance. 12 Additionally, one study of 185 patients in the ICU compared the hemodynamic effect of paracetamol IV and intravenous immunoglobulin (IVIG) in patients with sepsis. They reported that paracetamol induced substantially greater hypotension than IVIG in patients with sepsis (58% and 36.9% respectively). 13 Another study investigated the hemodynamic effects of IV paracetamol in critically ill children, finding that 24% of IV paracetamol doses were associated with an episode of hypotension. 14
Hemodynamic stability is crucial for the safety of critically ill patients. This study aims to assess the hemodynamic effect of IV paracetamol (IV paracetamol) by monitoring changes in blood pressure, urine output, and core temperature after drug administration in an ICU patient population. The findings of this study set the groundwork for enabling clinicians to establish suitable dosing protocols, consider alternative analgesic strategies if needed, and effectively manage patients’ overall hemodynamic status. We anticipate that our study will guide future research in this field and contribute to the formulation of guidelines or recommendations for the use of IV paracetamol in intensive care settings, allowing for better treatment strategies for this at-risk patient population.
Methods
Study design and participants
This retrospective observational study was conducted at the general ICU at Soroka Medical Center in Israel, including patients who received 1 GR fixed dose of Paracetamol 10 mg/ml for various indications in the ICU. The study period spanned from 01/01/2020 to 01/12/2022 and data was accessed for research purpose from 15/03/2023 to 01/03/2024. Inclusion criteria comprised patients aged 18 years and above who received IV paracetamol during their ICU stay. Exclusion criteria included patients with contraindications to IV paracetamol, incomplete data, or those receiving other antihypertensive medications affecting hemodynamics during the study period.
Data collection
Clinical and demographic data were collected from electronic medical records. Variables included age, gender, reason for ICU admission, and pre-existing medical conditions. IV paracetamol prescriptions were identified, and relevant information such as dosage, timing, and indication for administration were recorded.
Hemodynamic monitoring
Blood pressure measurements were obtained using invasive methods, including arterial line records at regular intervals pre- and post-IV paracetamol administration. Systolic and diastolic blood pressures were recorded at time points of interest at 15, 30, 45, and 60 min post-administration. Indirect hemodynamic parameters, including noradrenaline dosage and urine output pre and an hour post-IV paracetamol administration, were recorded.
Statistical analysis
Statistical analysis was performed using SPSS software (ver. 26.0 for Windows; SPSS Inc., Chicago, IL, USA). Baseline characteristics of the study population were summarized using descriptive statistics. Changes in blood pressure were analyzed using analysis of variance (ANOVA) with repeated measurements. Changes in indirect hemodynamic parameters were analyzed based on their distribution. A paired t-test was used for normally distributed variables, such as temperature, while the Wilcoxon rank-sum test was applied to non-normally distributed variables, including urine output and noradrenaline dose. Normality was assessed through visual inspection of distribution plots and formal testing using the Kolmogorov-Smirnov test. Potential baseline and clinical factors associated with hypotension after IV paracetamol treatment were analyzed using multivariate mixed linear models. The selection of variables for inclusion in the multivariate analysis was based on clinical and statistical significance. For all tests, a p value of <0.05 was considered statistically significant.
Ethics approval
This retrospective observational study titled “Thehemodynamic effects of IV paracetamol in intensive care patients” was approved by the Soroka Medical Center Institutional Review Board (approval number: 0293-22-SOR) on October 25, 2022. All data were fully anonymized and authors had no access to information that could identify individual participants after data collection.
The study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Study population
The cohort included a total of 498 patients who received IV paracetamol. Clinical and demographic characteristics of the study population are shown in Table 1. The primary reason for admission to the ICU was to facilitate ongoing treatment and close monitoring following general surgical intervention, observed in 319 (64.1%) of the patients. 305 (61%) of patients were male. The average age of all patients was 53.24 ± 20.06.
Demographics of study population (n = 498).
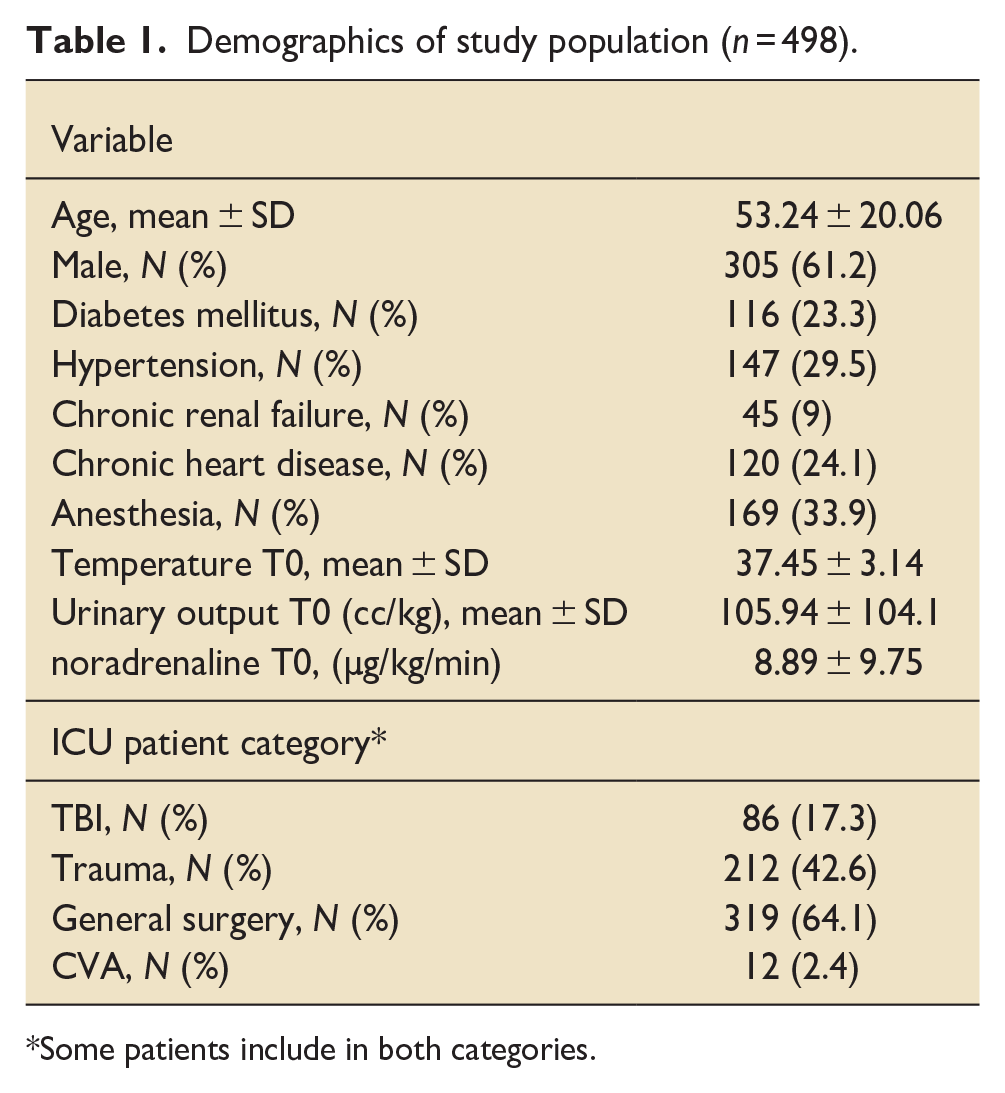
Some patients include in both categories.
Hemodynamic effects of IV paracetamol
Blood pressure evaluation after IV paracetamol administration is detailed in Table 2 and graphically represented in Figure 1(a) to (d), categorized by cohort subgroups.
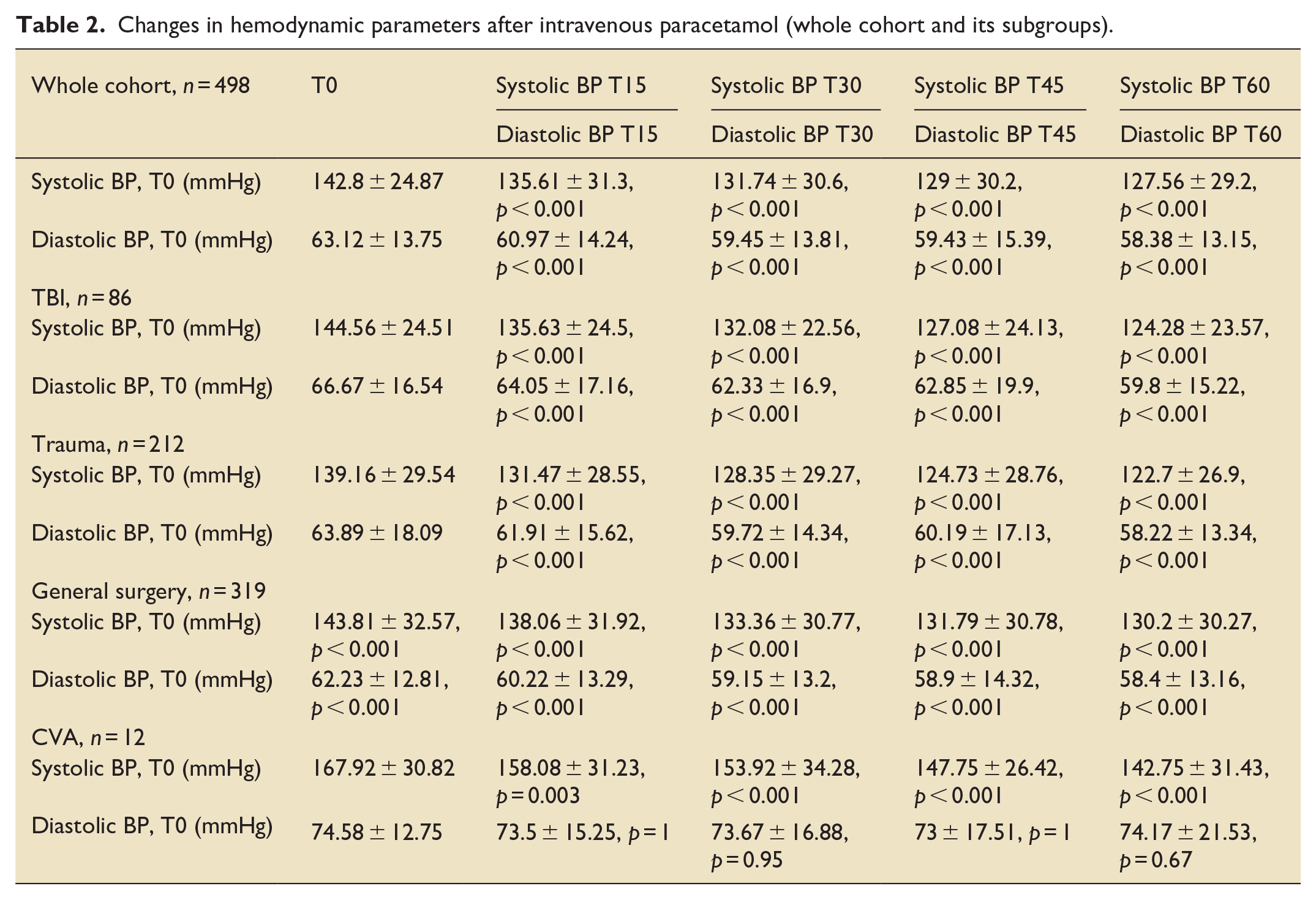
Changes in hemodynamic parameters after intravenous paracetamol (whole cohort and its subgroups).
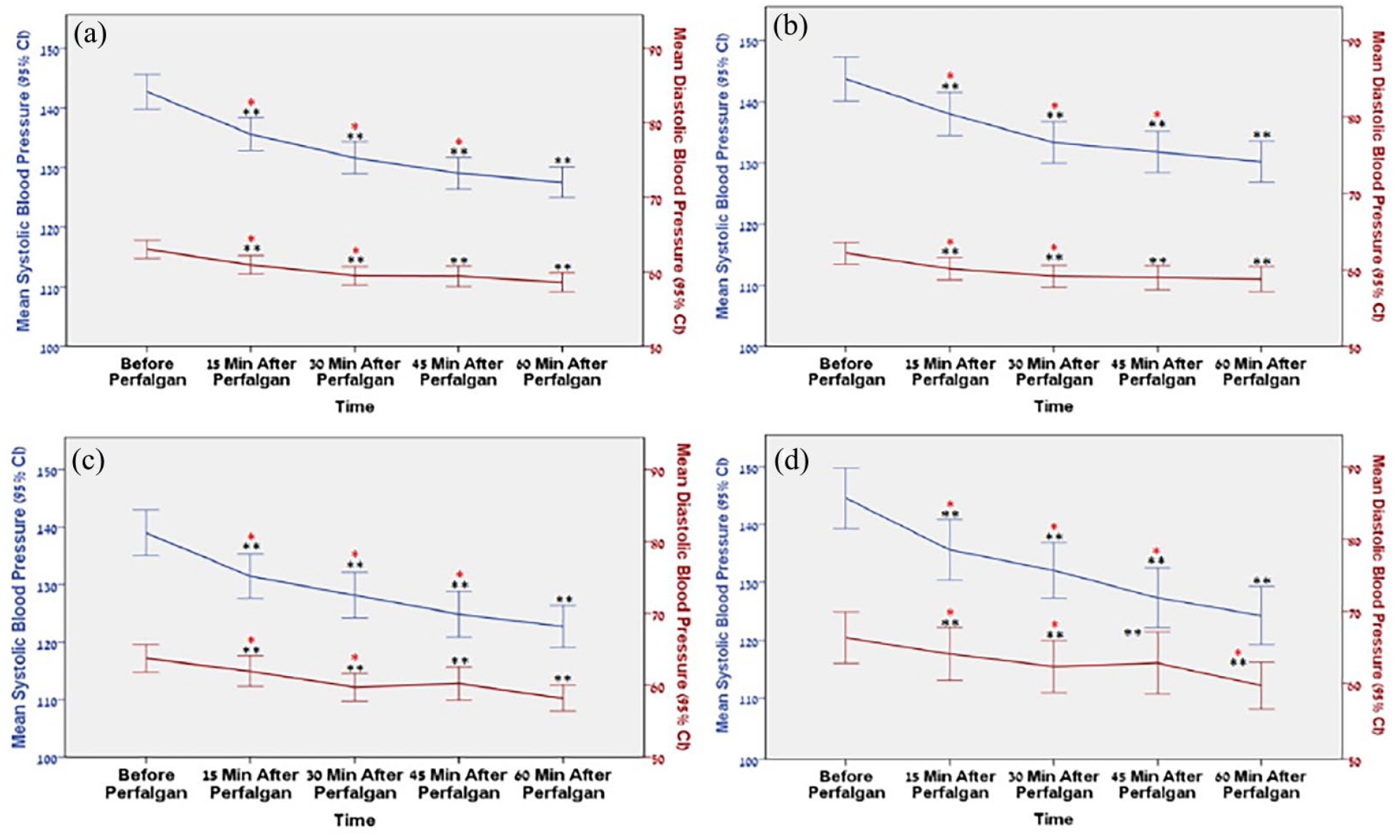
Change in systolic blood pressure (blue) and diastolic blood pressure (red) over time following Perfalgan administration in whole cohort (a), general surgery patients (b), trauma patients (c) and TBI patients (d).
For the entire study cohort (n = 498), a statistically significant decrease in mean systolic and diastolic blood pressure values was observed. The mean systolic blood pressure before the administration of IV paracetamol was 142.8 ± 24.87 mmHg, reaching its lowest value at 127.56 ± 29.2 mmHg 60 min after administration (p < 0.001) and the mean diastolic blood pressure prior to IV paracetamol administration was 63.57 ± 16.29 mmHg, reaching its lowest point at 58.34 ± 13.13 mmHg after 60 min (p < 0.001; Table 2).
This consistent trend was also evident across subgroups, including patients admitted to the ICU following general surgical intervention (n = 319), trauma (n = 212), traumatic brain injury (TBI; n = 86), and cerebral vascular accident (CVA; n = 12). Within the general surgery subgroup, the mean systolic blood pressure before and 60 min after IV paracetamol administration was 143.81 ± 32.57 mmHg and 130.2 ± 30.27 mmHg, respectively (p < 0.001) and the mean diastolic blood pressure decreased from 62.23 ± 12.81 mmHg before IV paracetamol administration to 58.4 ± 13.16 mmHg after 60 min (p < 0.001). Trauma patients exhibited a mean systolic blood pressure of 139.16 ± 29.54 mmHg before IV paracetamol administration, reaching its lowest value at 122.7 ± 26.9 mmHg 60 min after IV paracetamol administration (p < 0.001), and the mean diastolic blood pressure decreased from 63.89 ± 18.09 mmHg–58.22 ± 13.34 mmHg after 60 min (p < 0.001). In patients with TBI, the mean systolic blood pressure before IV paracetamol administration was 144.56 ± 24.51 mmHg, decreasing to 124.28 ± 23.57 mmHg 60 min post-administration (p < 0.001) the mean diastolic blood pressure decreased from 66.67 ± 16.54 mmHg–59.8 ± 15.22 mmHg after 60 min (p < 0.001). Mean systolic blood pressure in patients with CVA was 167.92 ± 30.82 mmHg before IV paracetamol administration, decreasing to its lowest value at 142.75 ± 31.43 mmHg 60 min after administration (p < 0.001). There was no significant difference in mean diastolic blood pressure measurements among patients with CVA (p > 0.05).
For both the entire cohort (Figure 1(a)) and its subgroups of general surgery (Figure 1(b)), trauma (Figure 1(c)), and TBI (Figure 1(d)), the most notable decrease in mean systolic and diastolic blood pressure occurred 45 min after IV paracetamol administration. No statistically significant difference was noted between the systolic measurements recorded at 45 min and at 60 min post-administration (p = 0.2, p = 0.17, p = 0.36 for the whole cohort, TBI and trauma, and for general surgery, respectively).
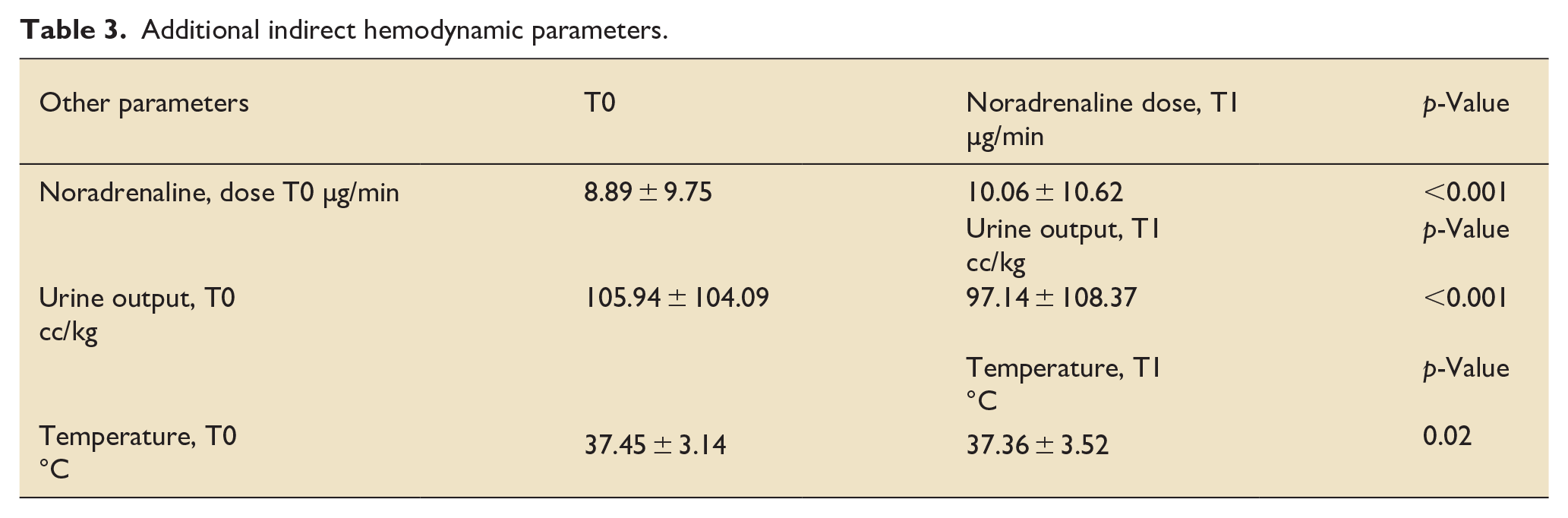
A statistically significant increase in noradrenaline dosage was observed after the administration of IV paracetamol, rising from a median of 7 (IQR: 4–8) µg/min to 8 (IQR: 4–10.5) µg/min (p = 0.02). Similarly, a significant decrease in urine output from a median of 88 (IQR: 40–138) cc/kg to 71.5 (IQR: 39.75–121) cc/kg was noted an hour after IV paracetamol administration, indicating a decline in end-organ perfusion (p < 0.001; Table 3). The multivariable analysis presented in Table 4 identifies clinical factors associated with a decline in systolic and diastolic blood pressure over time following IV paracetamol administration. The findings suggest that general anesthesia is associated with a significant decrease in both systolic (estimated coefficient: −10.77, 95% CI−16.22 to −5.31, p < 0.001) and diastolic blood pressure (estimated coefficient: −7.17, 95% CI−9.59 to −4.74, p < 0.001) over time. Additionally, the analysis indicates that a diagnosis of ischemic heart disease or congestive heart failure is associated with a significant decrease in diastolic blood pressure after IV paracetamol administration (estimated coefficient: −3.58, 95% CI−6.72 to −0.44, p = 0.03).
Additional indirect hemodynamic parameters.
Baseline and clinical factors associated with hypotension: a multivariate linear mixed model.
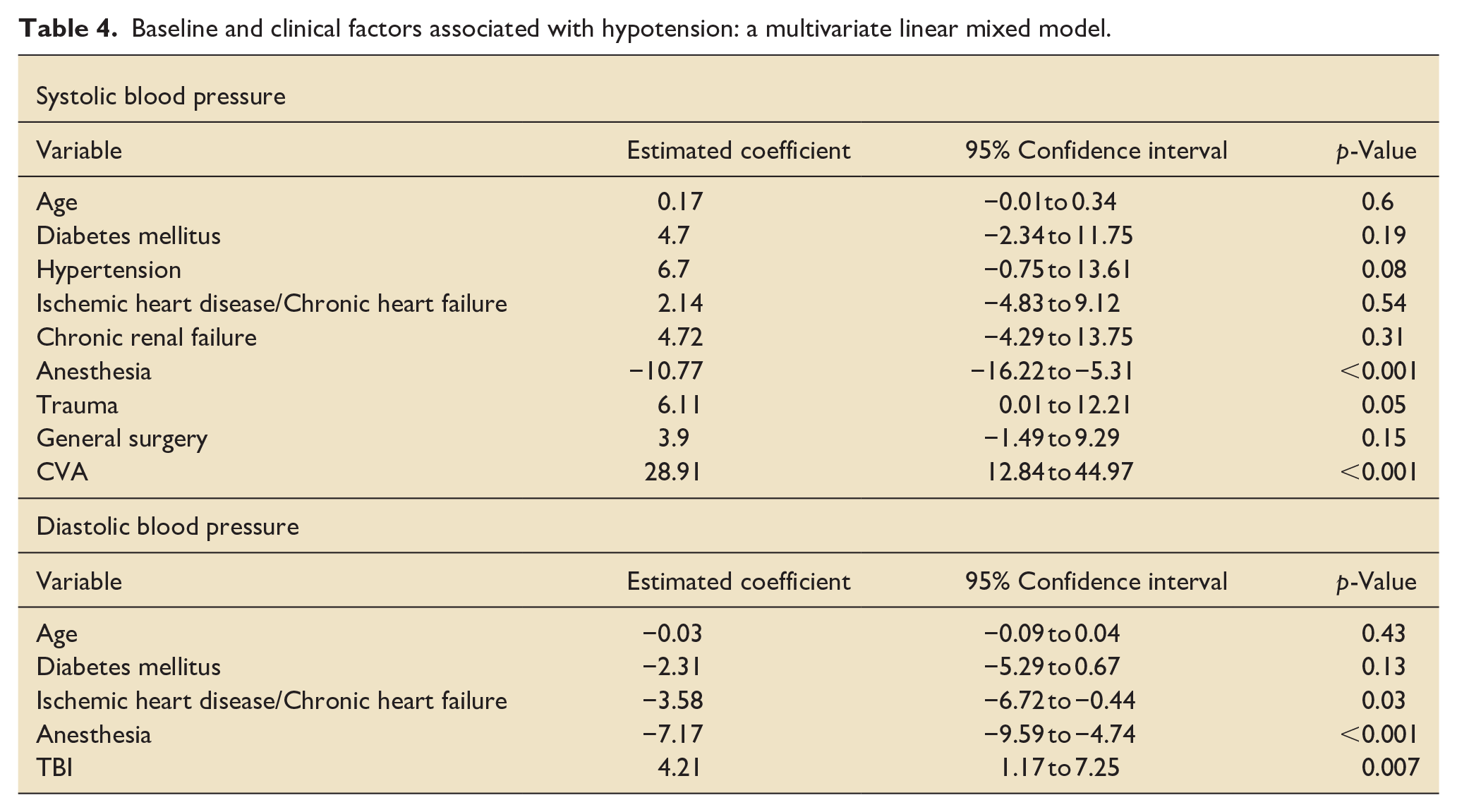
Conversely, there was a statistically significant association between CVA and an increase in systolic blood pressure (estimated coefficient: 28.91, 95% CI 12.84–44.97, p < 0.001) and between TBI and an increase in diastolic blood pressure (estimated coefficient: 4.21, 95% CI 1.17–7.25, p = 0.007).
Discussion
The observed hemodynamic effects of IV paracetamol in our study raise important considerations regarding its clinical implications, particularly in the context of critically ill patients admitted to the ICU. Our investigation into the systolic blood pressure changes following IV paracetamol administration revealed a statistically significant decrease in mean values across the entire study cohort and its subgroups, consisting of patients undergoing general surgery, trauma, TBI, and CVA. The most pronounced decline occurred 45 min after IV paracetamol administration, suggesting a temporal relationship between drug administration and the onset of hemodynamic effects at 45–60 min that is consistent with previous studies.3 –5
Similarly, our findings regarding diastolic blood pressure demonstrated a significant decrease in mean values after IV paracetamol administration, with the most prominent decline observed 30 min post-administration. This trend was consistent across general surgery and trauma subgroups, indicating a uniform effect on diastolic blood pressure in different clinical contexts.
The observed increase in noradrenaline dosage post-IV paracetamol administration underscores the clinical need for vasopressor support to maintain hemodynamic stability. This finding suggests that IV paracetamol may contribute to a hemodynamic compromise necessitating additional interventions, particularly in critically ill patients who may already have compromised cardiovascular function.
Our multivariate analysis indicates a higher probability of a decrease in both systolic and diastolic blood pressure among patients administered general
In addition, our multivariate analysis suggests a reduced likelihood of hypotensive episodes in the CVA group. Given that CVA patients typically require lowering of blood pressure and active management of hypertension, this medication is likely considered safe in that population and can aid in reaching their targeted blood pressure levels.
These results should be carefully considered when administering IV paracetamol to critically ill and hemodynamically unstable patients, as the medication may lead to additional hemodynamic compromise, a reduction in systemic vascular resistance, and a decrease in cardiac output. 10 Conversely, our findings also support IV paracetamol as a promising therapeutic option for pain relief and fever reduction in hypertensive patients, particularly in cases of TBI, intracranial hemorrhage, and CVA, for whom hypertension can contribute to comorbidities.
While the hemodynamic effects observed in our study provide valuable insights, several limitations warrant consideration. The retrospective nature of our analysis and the absence of a control group limit our ability to establish definitively a causal relationship between IV paracetamol administration and hemodynamic changes. Additionally, individual patient variability, pre-existing comorbidities, and concurrent medications may have an influence on the observed outcomes.
Conclusion
In conclusion, our study highlights the significant impact of IV paracetamol on systolic and diastolic blood pressure, necessitating careful consideration in the clinical management of unstable critically ill patients. Our conclusions support the use of IV paracetamol in hypertensive patients, particularly in cases of TBI, intracranial hemorrhage, and CVA. These findings contribute to the evolving understanding of the effects of IV paracetamol in critically ill populations and will inform clinical decision-making in the administration of this widely used analgesic and antipyretic medication.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.