
Abstract
Purpose
To perform a narrative review of the literature regarding the discharge of patients directly to home (DDH) from the intensive care unit, and to identify patient characteristics and clinical outcomes associated with this practice.
Methods
We searched MEDLINE and EMBASE from 1946 to present. We also manually searched the references of relevant articles. A two-step review process with three independent reviewers was used to identify relevant articles based on predetermined inclusion/exclusion criteria.
Results
Four studies were included in the final review. Two studies were retrospective and two studies were prospective that shared data from the same patient cohort. All were single center studies. Two of the four studies outlined clinical outcomes associated with DDH.
Conclusions
This study highlights the relative dearth in the literature regarding the increasingly common practice of DDH, underscores the importance of further studies in this area, and identifies future important foci of research.
Keywords
Introduction
Traditionally, patients discharged from the intensive care unit (ICU) have been transferred to either an intermediate care unit or directly to the ward. This traditional transition of care model is under pressure, largely due to hospital ward capacity pressures, causing the critical care community to increase their number of discharges directly to home (DDH) from the ICU. 1 There may be a risk of adverse events associated with DDH if it is not executed carefully. ICUs are not typically equipped with the personnel, resources, follow-up clinics, and discharge protocols that have been in place on the wards for decades. In addition, ICU survivors have prolonged recovery times that sometimes extend beyond hospital discharge and are clearly some of the sickest, most complex cases in the hospital. Conversely, if DDH is performed safely, it can shorten a patient’s length of stay and subsequently abrogate untoward iatrogenic morbidity, improve healthcare resource allocation and utilization, and reduce costs in an already strained healthcare system. Beyond these benefits, a recently published study has also demonstrated high patient satisfaction associated with this practice. 2
There are reports of chronically ventilated and palliative patients being discharged directly home from the ICU.3–6 These populations differ from the traditional ICU patients recovering from a critical illness that are the focus of our narrative review.
The expanding prevalence of DDH has yet to be matched by a well circumscribed body of literature supporting its safety and efficacy. Furthermore, DDH is not rigorously defined, with wide variations in definitions and practices existing in the critical care community.
We present a narrative review of the literature reporting patient discharges to home from ICUs or high dependency units. We go on to describe the process of direct discharge to home: highlighting its benefits, its potential risks, and shedding light on areas that merit further research.
Materials and methods
Search question, population, inclusion, and exclusion criteria
The objective of our narrative review was: “To identify the existing literature describing the practice of DDH, with respect to the patient populations and/or outcomes associated with this practice.”
Our inclusion criteria encompassed all prospective and retrospective studies in critically ill adults. Scoping reviews, systematic reviews, and meta-analyses were included. Eligible articles evaluated the transition of critically ill patients from an ICU or high dependency unit to home. ICU was defined as a distinct unit in the hospital that provided invasive monitoring, invasive and non-invasive mechanical ventilation, and administration of vasoactive agents to critically ill patients. A critically ill patient was defined as any patient admitted either electively or non-electively, requiring invasive monitoring, invasive and non-invasive mechanical ventilation, or administration of vasoactive agents. We classified high dependency units or step-down units as ICUs. Home was defined as any place of residence that was a non-healthcare facility or a facility that did not routinely have healthcare personnel available to care for residents (e.g. complex care, rehabilitation facility, nursing home). In this context, patients discharged to home from the ICU in conjunction with additional healthcare services were included.
We excluded all experimental/animal and pediatric studies. Studies pertaining to patients on chronic mechanical ventilation as well as patients discharged directly to home for palliation were excluded. Non-research and conference abstracts were excluded.
Search strategy
Unrestricted searches in MEDLINE and EMBASE were performed from 1946 to present to identify relevant articles. A combination of the following terms was used: ICU, critical care, patient discharge, home. A health information specialist performed the search with appropriate wildcards to take into account plurals and variations in spelling. The references of retrieved articles were screened for additional relevant articles. The full search strategy is available in online Appendix 1. We restricted our search studies to adults (defined as age 18 or older) and to those published in English. The searches encompassed both conference abstracts and non-research articles, which included editorials, correspondence letters, and textbook excerpts. Reference lists of relevant articles were manually searched to identify additional relevant articles.
Study selection and data extraction
Covidence® software was used to facilitate the review. Articles were assessed through a two-stage process to determine inclusion. In the first stage, two reviewers independently reviewed the titles and abstracts and relevant articles were selected for full text review (JB and JL). A third reviewer resolved disagreements (VL). In the second stage, conference abstracts or non-research studies were excluded. Two reviewers independently reviewed the full texts of the articles selected in the first stage (JB and JL). Disagreements between reviewers were discussed in conjunction with a third reviewer (VL) in order to reach agreement. Reviewers were not blinded to the author nor to the journal that the article was published in. In situations where it was unclear if the patient population was discharged from the ICU to home for any given study, the corresponding authors were contacted for further clarification.
Two reviewers independently extracted data in duplicate through a standardized form. We included study design, number of patients, ICU type (medical, surgical, etc.), patient demographics, ICU and hospital characteristics, and outcomes.
Results
Description of the articles
Our search strategy identified 106,029 studies. From these, 86,430 duplicates were removed by Covidence®, leaving 19,599 studies for review. A review of the titles and abstracts yielded 229 full text articles in English. The full texts of these studies were fully reviewed and 225 citations were excluded (Figure 1). The major reasons for exclusions included incorrect patient population, non-relevant articles, and non-research studies.
PRISMA flow diagram. PRISMA indicates preferred reporting items for systematic reviews and meta-analyses.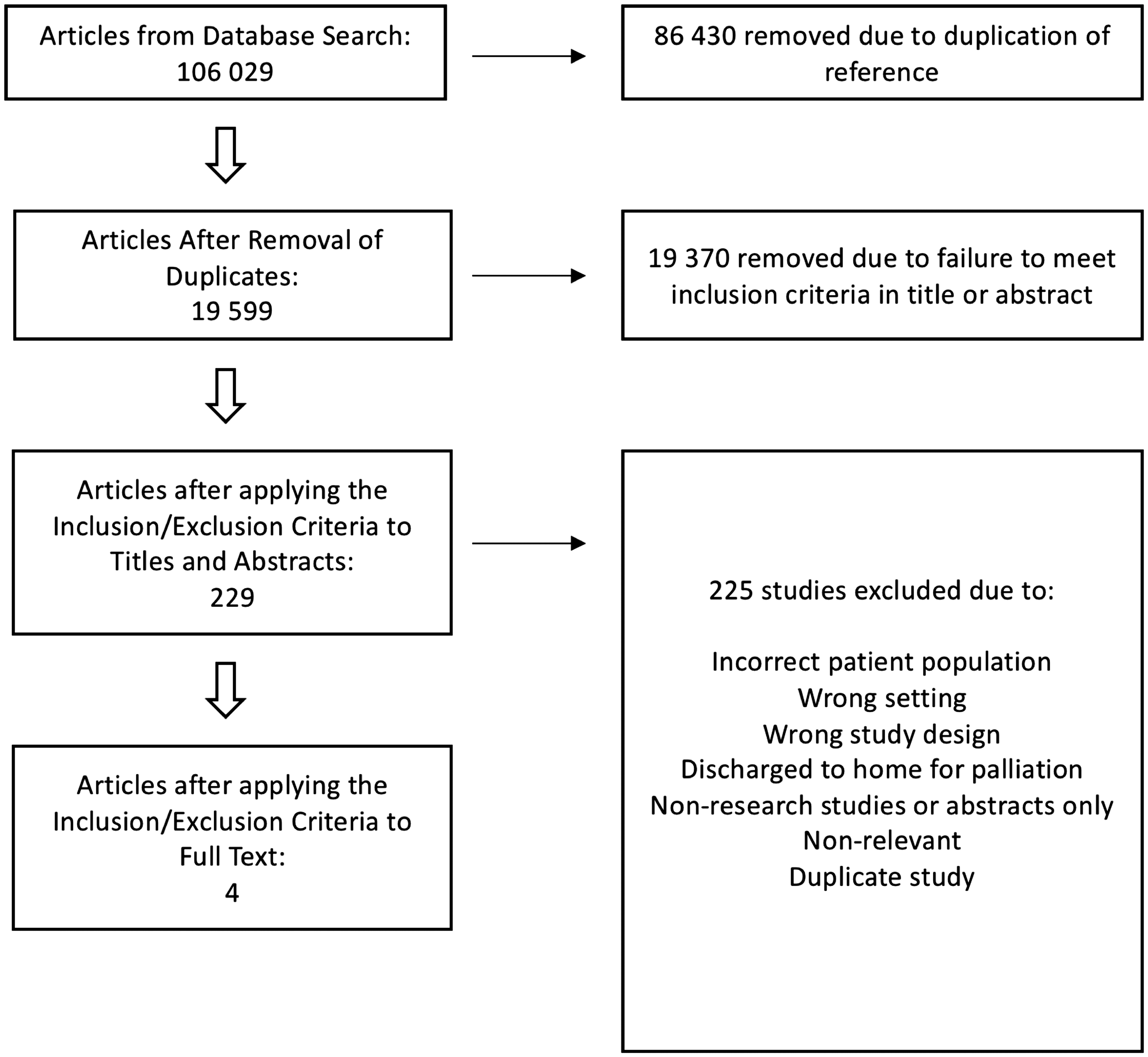
The majority of non-relevant studies in the full text review reported on ICU discharge outcomes of patients discharged to the ward first. A few studies noted their experience with discharging ICU patients to home. Two of these studies7,8 were excluded as the discharges were all against medical advice. One citation was excluded based on discharge of chronically ill respiratory patients requiring home mechanical ventilation. 3 Two studies were excluded because they described the discharge of critically ill patients to home for palliation.9,10 One other study reported about ICU discharge of chronic critically ill patients in a very small cohort (2 patients in a cohort of 16) 11 but despite contacting the corresponding authors, we could not determine whether or not they were DDH from the ICU. Ultimately, four studies were selected for data extraction based on our pre-established inclusion and exclusion criteria.1,2,12,13 Among these, two studies utilized the same cohort of patients. Manual review of the references of these studies did not yield additional articles for consideration. The results of our search strategy are summarized in Figure 1.
Patient and ICU demographics and study design
Study design and primary endpoints/outcomes.
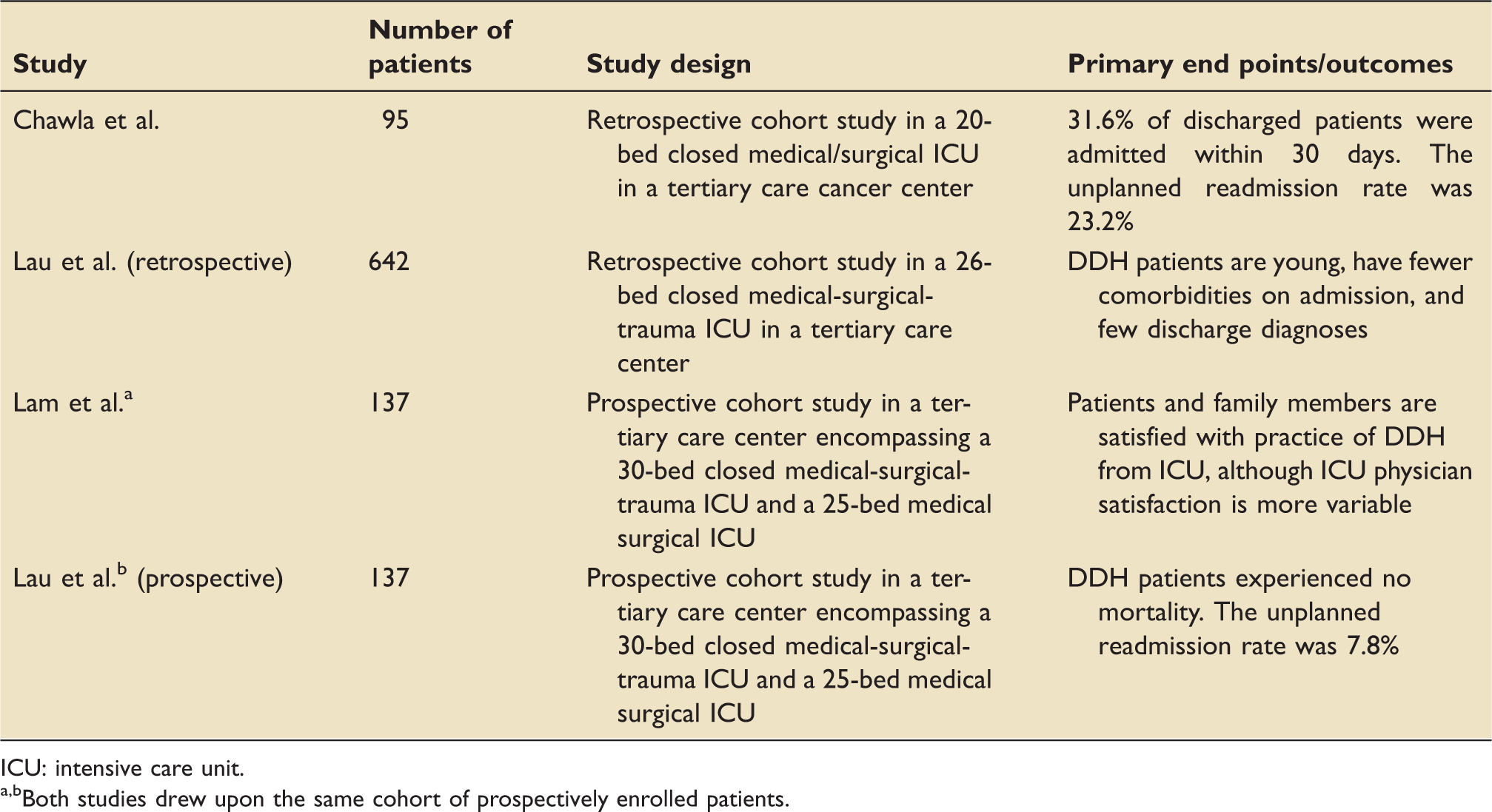
ICU: intensive care unit.
Both studies drew upon the same cohort of prospectively enrolled patients.
Patient demographics and clinical characteristics.
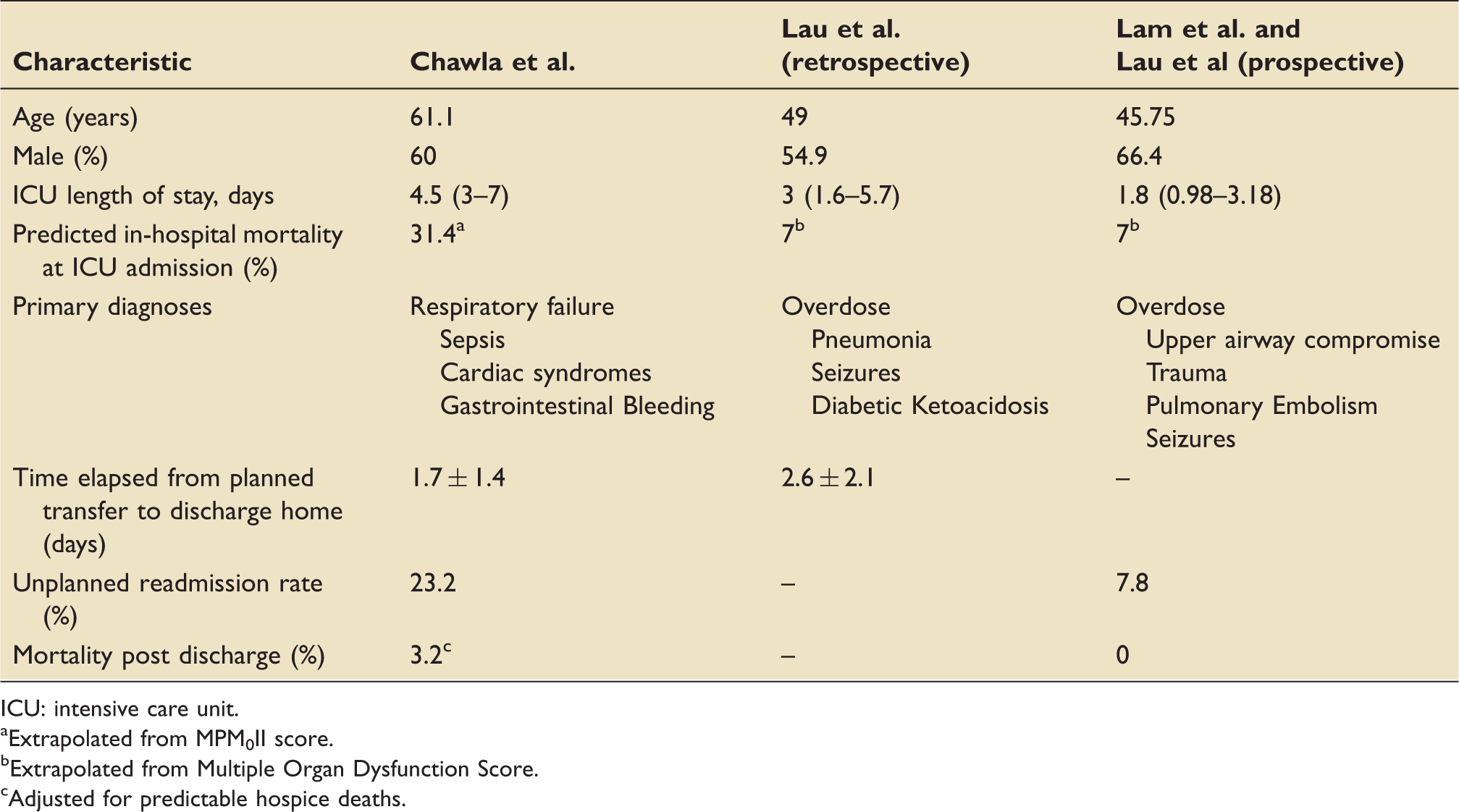
ICU: intensive care unit.
Extrapolated from MPM0II score.
Extrapolated from Multiple Organ Dysfunction Score.
Adjusted for predictable hospice deaths.
Intensive care unit and hospital characteristics.
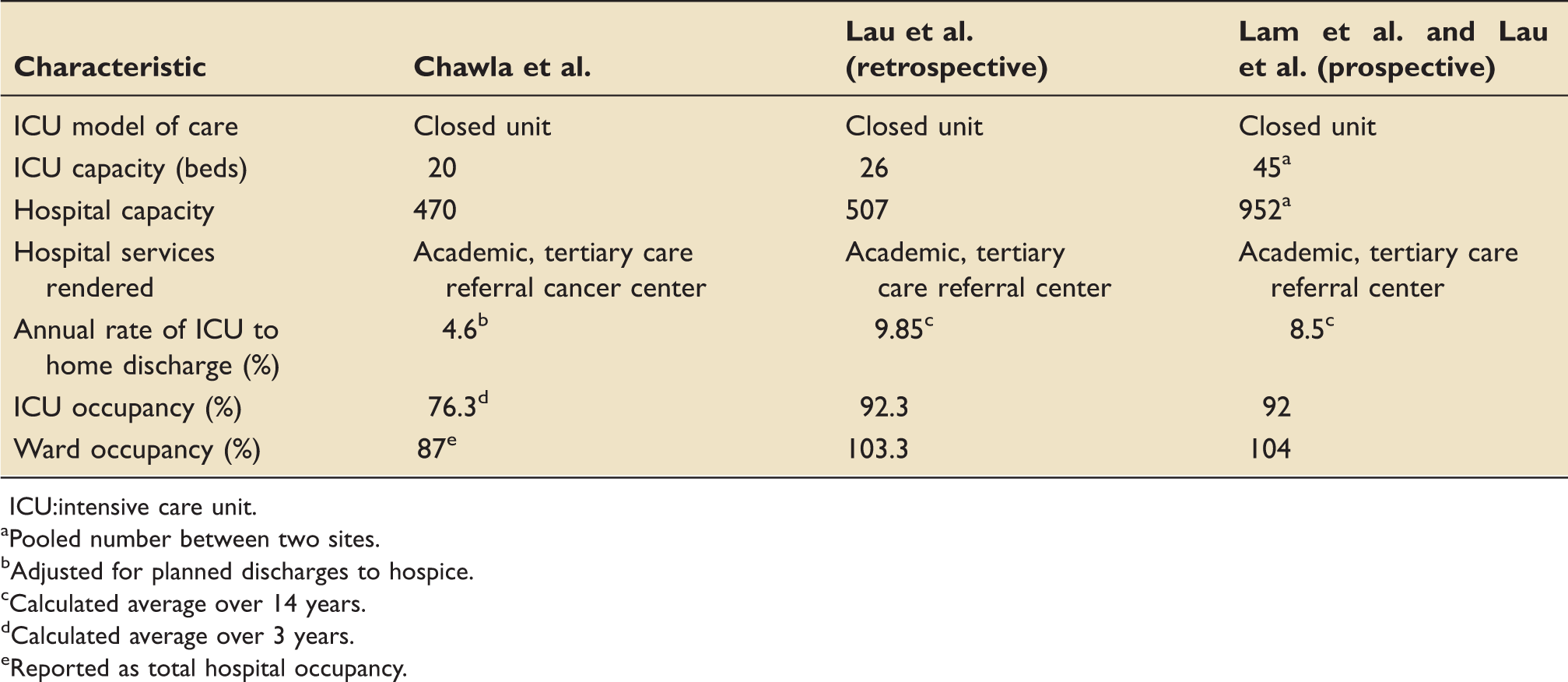
ICU:intensive care unit.
Pooled number between two sites.
Adjusted for planned discharges to hospice.
Calculated average over 14 years.
Calculated average over 3 years.
Reported as total hospital occupancy.
Discussion
We initially sought to perform a systematic review, but only four studies were identified that described the patient demographics and/or outcomes associated with DDH: all of which were single center and two of which were retrospective studies. While the cohorts shared some similarities such as a low acuity of illness and shorter length of stay, there were stark differences in the demographics of the patient population and in the interplay between occupancy rates of the ICU and the ward. The heterogeneity among the studies makes it challenging to draw definitive conclusions but highlights the importance of further prospective research in this area.
Proponents of DDH claim that its value lies in curtailing the volume of ward transfers, yielding both patient centered and system centered benefits. Patients who await ward transfer and experience transfer delays out of the ICU have the potential to suffer iatrogenic morbidity, including disturbances in sleep and delirium14,15 and increased risk of nosocomial infections. 16 A recent multicenter study demonstrated that patients experiencing an ICU discharge delay of more than 6 h had longer hospital length of stay and were more likely to be discharged after hours. 17 This increase in hospital length of stay may be the result of ward teams needing time to familiarize themselves with patients prior to hospital discharge. When faced with delays in ward transfer due to census issues, patients who could otherwise be discharged directly home from the ICU may be transferred to the wards after-hours. After-hours transfers from the ICU are well known to be associated with higher in-hospital mortality.18,19
Handover is known to be a high-risk period of patient care with the potential to cause adverse events.20,21 The transition of care from the ICU to the ward requires handover of a patient with a complex course from one care team to another. In some cases, opting to discharge a patient to home instead of conforming to historical transition-to-ward models can reduce the number of handovers and spare the patient undue morbidity.22,23 Based on Lau et al’s prospective study, ICU patients discharged directly to home had less unplanned return visits and readmission rates than those who were transferred to the ward and subsequently discharged within 24 h. A future trial randomizing ICU patient expected to need short ward stays to either DDH or ward transfer is required to definitively answer the question of which course is better for patient outcomes.
The practice of DDH can be a valuable tool in the management of ICU census and capacity. Several studies have shown a positive association between mortality and ICU occupancy rate.24–26 This phenomenon can be independent of patient acuity, as demonstrated by one study which showed that peak occupancy and the ratio of occupied to appropriately staffed beds were most strongly associated with mortality, even after controlling for acuity. 27 These data suggest that DDH candidates awaiting ward beds can adversely affect the management of other ICU patients.
Chawla et al.’s study reported a 23.2% unplanned readmission rate, while Lau et al.’s study reported a 7.8% unplanned readmission rate in. The glaring difference in outcomes between these studies is a testament to the tremendous potential for DDH. These two studies highlight two contrasting cohorts: one is older, with an established diagnosis of malignancy, higher predicted mortality at ICU admission, and longer ICU length of stay; while the other is younger, with a lower predicted mortality at ICU admission, and a shorter ICU length of stay. We feel that the stark contrast in unplanned readmission rates between the two major studies demands further work in this area, in the form of a multi-center, randomized trial, and the derivation and validation of a prediction model to guide clinicians in their selection of patients that may be safely discharged directly home.
Current admission triage and discharge guidelines do not provide any recommendations on the practice of DDH, 28 leaving clinicians to use their own judgment when planning the disposition of a critically ill patient. Discharge planning requires medication reconciliation, arrangement of home supports, and scheduling outpatient appointments as demonstrated in Chawla et al.’s study. We feel that the increasing rates of DDH should serve as a call to empower ICUs to develop the infrastructure required to discharge patients safely – which can include streamlining the discharge process for these complex individuals or to have pre-emptive ICU follow-up to mitigate bounce-backs. It also highlights that future research should evaluate the economic sequelae and the net effect this practice has on the healthcare system. Future direct discharge home guidelines would be well served by the incorporation of a randomized control trial, clinical prediction model, and economic analysis of DDH. This scientifically derived evidence could improve the confidence of ICUs who currently have much lower DDH rates than those in this review (9.9% over 12 years in Lau et al.’s study), empowering them to increase their DDH rates.
Conclusion
Our review identified four single center DDH studies, two of which drew upon the same prospectively enrolled cohort of patients. We confirm the scarcity of data describing the practice of DDH, describe benefits of the practice as well as some well-founded reservations, and suggest future avenues of research to better character should address clinical and economic outcomes associated with DDH in a prospective and multicenter fashion, as well as the development a clinical prediction model and clinical practice guidelines to better inform the safe practice of DDH.
Supplemental Material
Supplemental material for Lessons learned and new directions regarding Discharge Direct from Adult Intensive Care Units Sent Home (DISH): A narrative review
Supplemental material for Lessons learned and new directions regarding Discharge Direct from Adult Intensive Care Units Sent Home (DISH): A narrative review by John Basmaji, Vincent Lau, Joyce Lam, Fran Priestap and Ian M Ball in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.