
Abstract
Intensive Care Unit staff deal with potentially traumatic cases throughout their careers. We designed and implemented a ‘Team Immediate Meet’ (TIM) tool, a communication aid designed to facilitate a two-minute ‘hot debrief’ after a critical event, provide the team with information about the normal reaction to such an event and signpost staff to strategies to help support their colleagues (and themselves). We describe our TIM tool awareness campaign, quality improvement project and subsequent feedback from staff who reported that the tool would be useful for navigating the aftermath of potentially traumatic events and could be transferable to other ICUs.
Introduction
It is inevitable that staff working in intensive care units (ICUs) will encounter difficult cases. 1 Trauma Risk Management (TRiM) is a peer support tool developed by the UK Armed Forces to help troops prepare for and recover from potentially traumatic events.2,3 Although we introduced TRiM in Bath in 2012 following an ICU fire, 4 it was not used to its full potential. 5 We therefore designed and implemented a communication aid for use immediately after a critical event 5 with the following aims: first, to assist and empower staff to lead a short ‘hot debrief’, even if affected by cognitive overload; second, to record names of all staff involved immediately to facilitate supportive follow up, as it is difficult to do this after the event; third, to encourage TRiM referrals to be made using full names and email addresses of staff involved; fourth, to provide staff with information about common feelings and suggested actions - based on the Principles of Psychological First Aid, advocated by the World Health Organisation, 6 and the ‘PIES Principles of Cooperative Learning.’ 7
Following implementation of the first version in 2020,
5
we collaborated with Intensive Care Society staff to optimise the wording, layout and design of this tool. We produced a second version, re-named the ‘Team Immediate Meet’ (TIM) tool (Figure 1), including our hospital TRiM team email address. Other hospitals could potentially personalise the TIM tool by adding their own staff follow-up email address. Team Immediate Meet tool - RUH Bath version.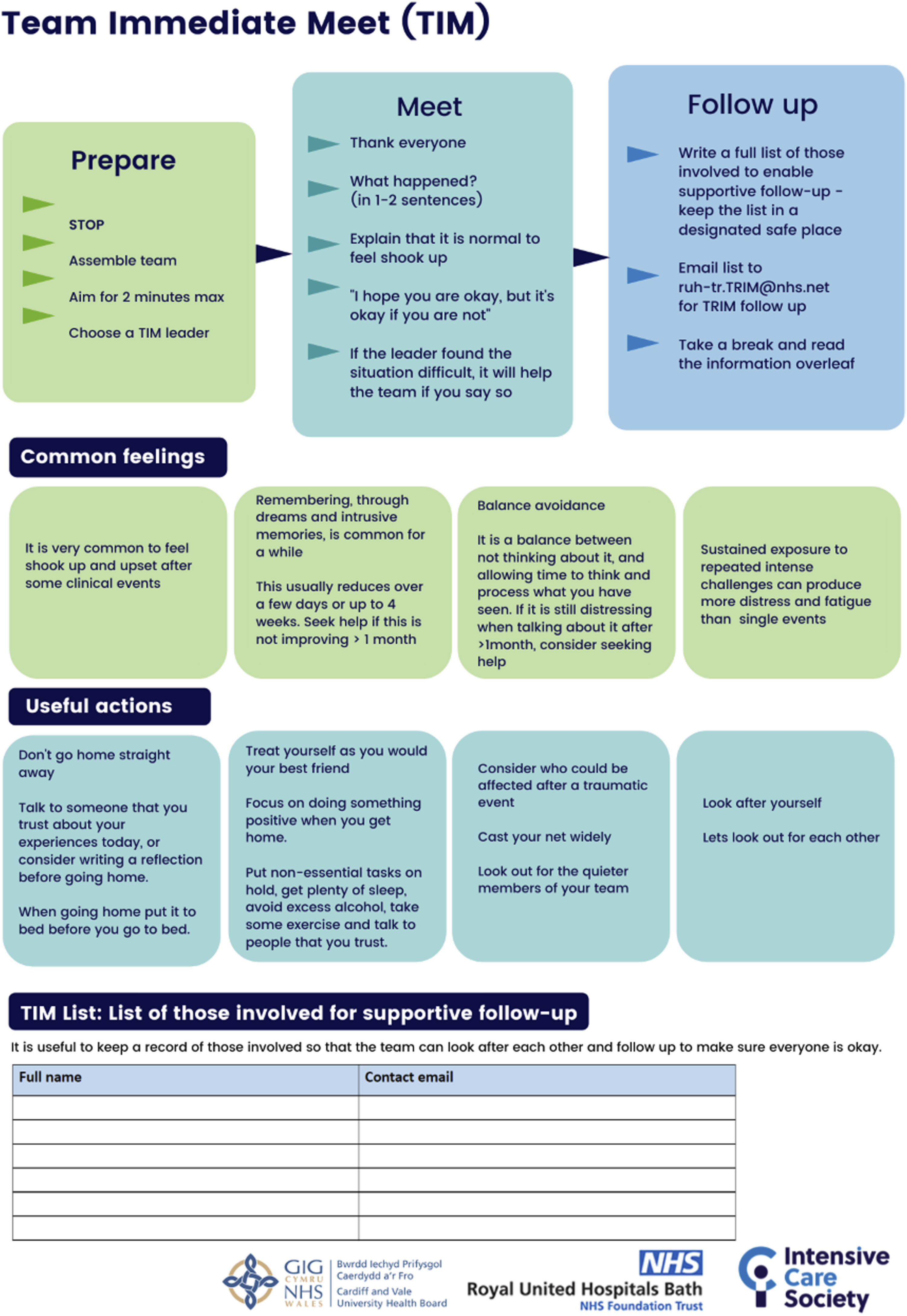
Methods
Laminated copies of the TIM tool were displayed in ICU central locations and staff coffee rooms. We designed and delivered an education and awareness programme for our ICU multidisciplinary team in 2021, using the ‘Tea Trolley’ training method, 8 and comprising 5–10 min ‘bite sized’ bedside teaching sessions: these covered the TIM tool’s purpose, location and when and how it should be used. Immediately after teaching, participants completed a short questionnaire rating their perceived confidence in using the tool and its potential benefit, plus an opportunity to share situations when this tool may have been useful.
Staff feedback was used to drive further improvements with a third version (Figure 1) launched in September 2021. To assess implementation, we analysed the hospital’s TRiM team’s records to measure the number and completeness of TRiM referrals and surveyed ICU and TRiM team staff.
Results
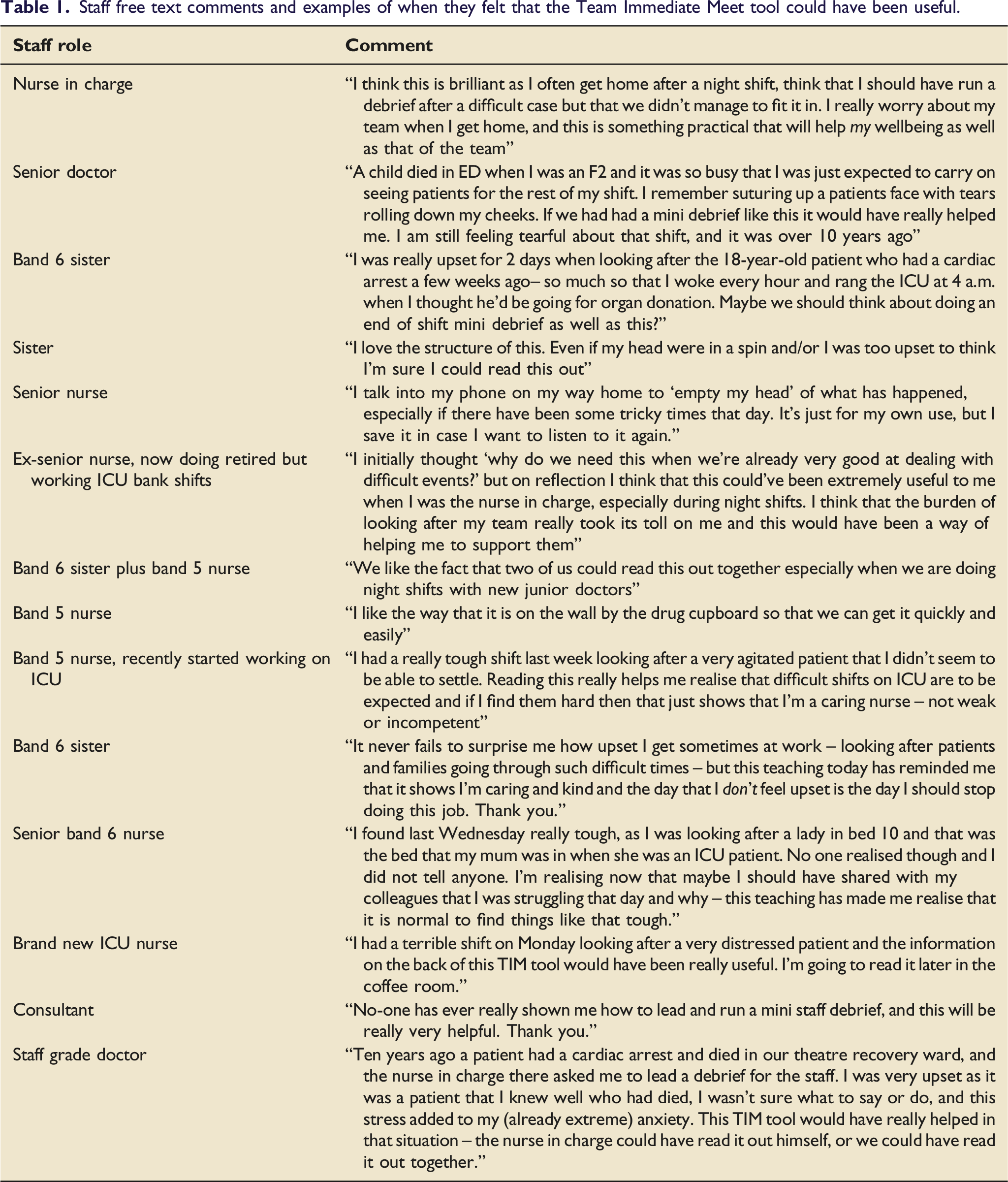
Staff free text comments and examples of when they felt that the Team Immediate Meet tool could have been useful.
Following the launch of the third version, the hospital TRiM team reported the following improvements to TRiM referrals: increased numbers; made by a wider range of staff and more quickly after an event; less time required to chase full names of staff involved. Four multidisciplinary team ICU staff who had used the TIM tool following a critical event in the preceding month participated in the follow-up survey, with all reporting that the TIM tool would ‘definitely’ or ‘maybe’ result in the following: help staff lead a hot debrief; provide a prompt to make a TRiM referral; make the TRiM referral process easier; and provide a prompt to include a full list of all staff involved. All recommended the TIM tool to other hospitals.
Discussion
The TIM tool was well received by our multidisciplinary ICU team, who reported that it would increase their confidence to lead a ‘hot debrief’ and help the team following a potentially traumatic event. Preliminary feedback one month after implementation was very positive.
Staff stories suggest that staff may benefit from a hot debrief in many situations: the TIM tool is a simple and inexpensive strategy that may assist ICU teams in doing so, and in improving staff wellbeing following a critical event we may also improve patient safety. We believe that this tool would be easily transferable to and reproducible in other ICUs, plus other areas of the hospital. It is currently being trialled in Cardiff ICU, with the ICU clinical psychologist’s email address used to provide supportive follow up.
A limitation of the TIM tool is that it does need to be associated with a formal governance system to follow up staff involved in a critical event, such as a TRiM team or a clinical psychologist working as part of an ICU team.
Footnotes
Acknowledgements
We thank Drs T. Johnson, F. Millinchamp, M. Osborn, S. Shatwell, K. Herneman and S. Gouldson, Ms Simona Hanson and the Intensive Care Society graphic design team for their work and contributions towards the development of the TIM tool.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.