
Abstract
Background
The family members of intensive care unit (ICU) patients play a crucial role in modern ICUs. These individuals are predisposed to the development of post-intensive care syndrome in family members (PICS-F), a syndrome experienced by family members of ICU patients in response to critical illness and characterised by new or worsening psychological symptoms. This study sought to evaluate the levels of anxiety and depression exhibited by the family members of patients hospitalised in the ICU. It also aimed to identify the risk factors associated with the experience of PICS-F, which should assist with its prevention in the future.
Methods
The study sample comprised 164 ICU patients and their family members. Sociodemographic data were gathered at the time of ICU admission and 3 months after discharge, and the family members were screened for emotional distress using the Hospital Anxiety and Depression Scale (HADS). Comparison tests were used to test for an association between family/patient characteristics and a positive HADS score. In addition, a multivariable logistic regression model was constructed to identify the independent factors associated with a positive HADS score.
Results
Emotional distress was identified in 24% of the family members 3 months after their relatives had been discharged from the ICU. A number of personal traits were found to be associated with emotional distress in the family members, namely unemployment (p = .008), smoking/drinking habits (p = .036) and personal history of psychopathology (p = .045). In the multiple logistic regression analyses, only unemployment was found to be an independent factor associated with both anxiety and depression in the family members (OR = 2.74, CI 95%: 1.09–6.93). No association was found between the patients’ characteristics and emotional distress in the family members.
Conclusions
The findings of this study indicate an association between emotional distress in the family members of ICU patients and their personal traits, thereby building on the prior literature by suggesting that patient characteristics are less pertinent to the experience of PICS-F. Unemployment may represent a meaningful risk factor for emotional distress in family members (a potential marker of PICS-F), given its relationship with family members’ positive HADS scores post-ICU discharge. These findings should influence preventative strategies concerning PICS-F by illustrating the need to assess family characteristics and demographics early in a patient’s ICU stay and, consequently, allowing for the early identification of at-risk individuals and the prompt implementation of adequate support services.
Introduction
Background/rationale
Advances in intensive care medicine and the associated increased likelihood of patients surviving critical illness, as well as the rising demand for critical care among an ageing population, have increased clinical awareness of the impact of intensive care unit (ICU) hospitalisation on long-term disability and quality of life.1–2
Any new or worsening impairments in terms of patients’ physical, cognitive or mental health status arising after the experience of critical illness and persisting beyond acute care hospitalisation have been described as post-intensive care syndrome (PICS). Importantly, critical illness is associated with significant challenges not only for the surviving patient but also for members of their family, and therefore, PICS can also be experienced by these elements, in whom it is referred to as post-intensive care syndrome in family members (PICS-F). 2 PICS-F concerns the response to a patient’s critical illness on the part of family members and includes the acute and chronic psychological symptoms experienced by them during their relative’s critical illness as well as those that occur following the death or discharge from the ICU of their loved one.1,3–4
Acknowledging family members’ individual needs is fundamental to the work of healthcare professionals in any modern ICU, where the focus has shifted from the provision of patient-centred care to the provision of patient- and family-centred care. Family members participate in decision-making processes; champion the patient’s beliefs, wishes and values; and assume caregiver roles after the patient’s discharge from hospital, as the patient is then frequently physically and cognitively impaired and, therefore, requires help with the activities of daily life.4–5 In addition, the family members of ICU patients have to deal with their own psychological distress in the face of acute and severe illness as well as the uncertainty surrounding outcomes after ICU admission. 3 Emotional distress, the disruption of family dynamics, financial pressures and work overload can all impose significant burdens on family members. 6 It has previously been observed that up to 60% of family members experience the symptoms of post-traumatic stress, anxiety, depression and complicated grief during the first 6 months following their relative’s hospitalisation in the ICU.4,7
A number of tools have been developed to screen for mental disorders in clinical practice, mainly through the use of simple questionnaires that allow for the recognition of such disorders by clinicians not specifically trained in psychology or psychiatry. The Hospital Anxiety and Depression Scale (HADS) was developed by Zigmond and Snaith in 1983 8 to identify anxiety and depression among non-psychiatric patients within a hospital setting, although it has since been validated as a community screening tool for these pathologies.9–10
Hospital Pedro Hispano, located in Matosinhos, Portugal, has a medical-surgical, multidisciplinary ICU. As of 2020, the ICU had 10 beds available for level II and III patients and admitted approximately 350 patients every year. The ICU treatment policy includes paying special attention to family members because they are seen as an extension of patients and an essential element of their wellbeing. The ICU has a flexible policy when it comes to family visits, including extended visiting hours, as it is understood that such an approach can have a positive impact on both patients and their families.11–12
Objectives
The present study sought to evaluate the presence of anxiety and depression symptoms among the family members of ICU patients 3 months after their ICU discharge, as well as to identify risk factors associated with PICS-F. Anxiety and depression were considered manifestations of emotional distress and used as potential markers of PICS-F. It was hypothesised whether personal traits of family members could influence the presence of emotional distress among them 3 months after their relatives’ ICU discharge.
Methods
Study design and setting
This prospective observational cohort study was conducted in the medical-surgical ICU at Hospital Pedro Hispano over a period of 32 months (April 2017 to December 2019).
Family members’ characteristics.
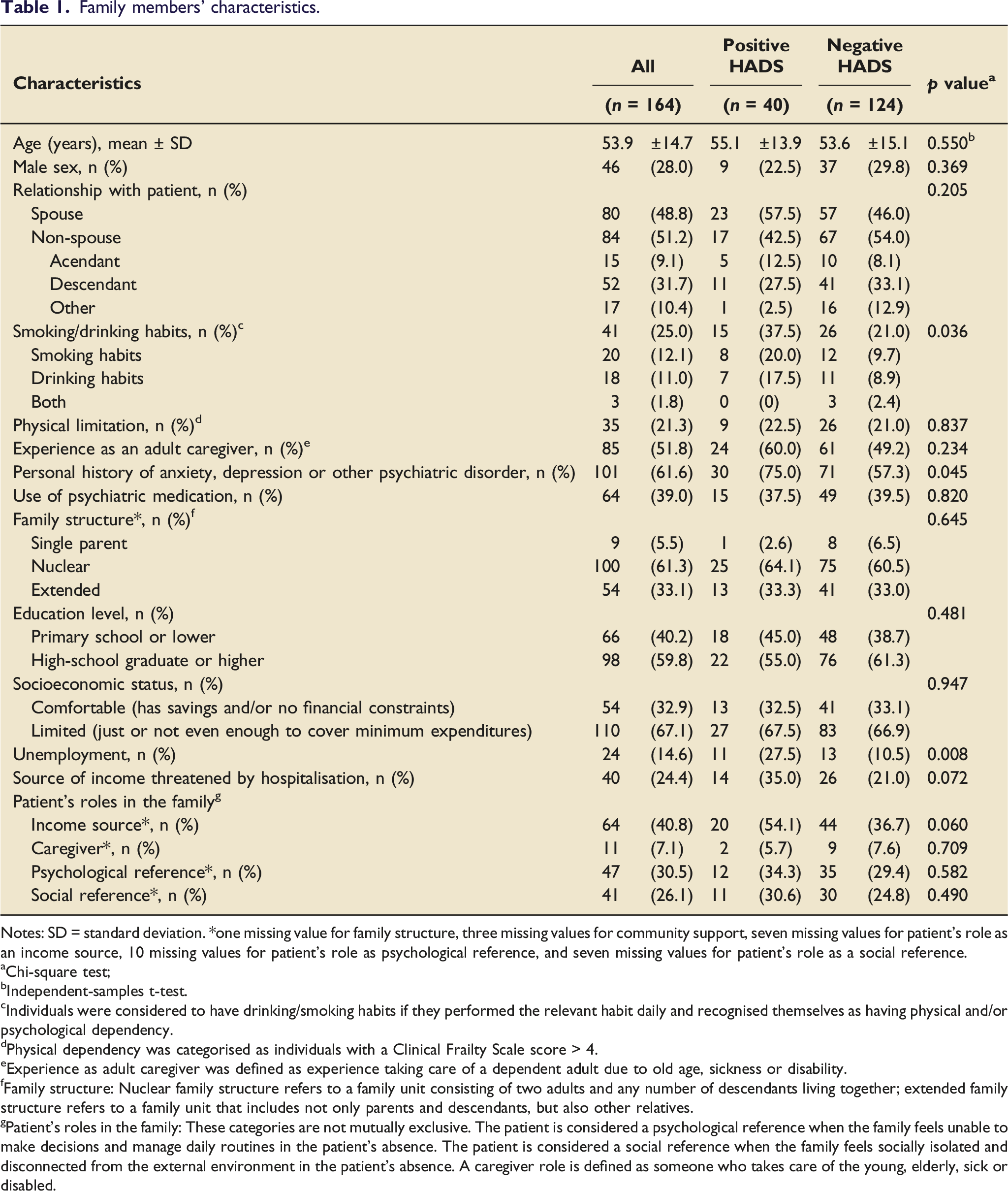
Notes: SD = standard deviation. *one missing value for family structure, three missing values for community support, seven missing values for patient’s role as an income source, 10 missing values for patient’s role as psychological reference, and seven missing values for patient’s role as a social reference.
Chi-square test;
Independent-samples t-test.
Individuals were considered to have drinking/smoking habits if they performed the relevant habit daily and recognised themselves as having physical and/or psychological dependency.
Physical dependency was categorised as individuals with a Clinical Frailty Scale score > 4.
Experience as adult caregiver was defined as experience taking care of a dependent adult due to old age, sickness or disability.
Family structure: Nuclear family structure refers to a family unit consisting of two adults and any number of descendants living together; extended family structure refers to a family unit that includes not only parents and descendants, but also other relatives.
Patient’s roles in the family: These categories are not mutually exclusive. The patient is considered a psychological reference when the family feels unable to make decisions and manage daily routines in the patient’s absence. The patient is considered a social reference when the family feels socially isolated and disconnected from the external environment in the patient’s absence. A caregiver role is defined as someone who takes care of the young, elderly, sick or disabled.
All surviving patients who had been treated in the ICU for at least 3 days during the study period were summoned for a follow-up consultation alongside their family member. This consultation took place 3 months after each patient’s ICU discharge and was conducted by an ICU physician and a nurse. As part of the consultation, the patients were evaluated for the development of both physical and non-physical PICS, while the family members were assessed with regard to their burden and emotional distress. During the follow-up consultation, in the presence of the ICU nurse, the family members were screened for anxiety and depression using the Portuguese version of the HADS. 13 The HADS is a self-report questionnaire designed to assess how the individual has felt during the previous week. It is composed of 14 questions, seven concerning anxiety and seven concerning depression. Each question is answered on an ordinal scale ranging from 0 (none) to 3 (maximum). According to the authors of the HADS, a score between 0 and 7 for either subscale is regarded as ‘normal’, a score between 8 and 10 as being ‘suggestive of the presence of anxiety/depression’ and a score of 11 or higher as indicative of the ‘probable presence of the mood disorder’. 14 In this study, a score of 11 or higher on either subscale was regarded as a positive HADS score, which was considered to be representative of emotional distress.
Information regarding the patients was collected 3 months after their ICU discharge. More specifically, basic sociodemographic data (age and sex) and data regarding the hospitalisation (length of ICU and hospital stay) were collected from the clinical records. Additional data were collected during the follow-up consultation.
Each patient’s fitness and frailty status were evaluated using the Clinical Frailty Scale (CFS) 15 at the time of ICU admission and during the follow-up consultation. A CFS score ≤4 was used in the present study to distinguish patients who could manage the activities of daily life independently from those who could not.
The severity of each patient’s illness was classified according to the Simplified Acute Physiology Score (SAPS II). 16 Other data collected during the follow-up consultation were also included, particularly regarding the patient’s physical status (ICU Mobility Scale <10 and/or receiving physiotherapy) and psychological status (HADS anxiety and/or depression subscale score ≥11). Finally, it was also noted whether a patient diary was created during the ICU stay.
Participants
During the study period, all family members who met the inclusion criteria were approached and invited to participate in the study. The term ‘family member’ was defined as indicating someone who shares an emotional and affectionate relationship with the patient, not implying cohabitation, a legal relationship or consanguinity with the patient. Paid caretakers were not included within this definition.
The inclusion criteria for this study were as follows: family member’s age >18 years, patient’s ICU stay
Primary outcome
The primary outcome in this study was emotional distress on the part of the family member 3 months after their relative’s ICU discharge. Emotional distress was indicated by a score of 11 or higher for either the HADS anxiety subscale or the HADS depression subscale. Emotional distress was regarded as a potential marker of PICS-F.
Statistical analysis
A descriptive analysis of all the collected data was conducted. The categorical variables were presented as frequencies and percentages, while the continuous variables were expressed as means and standard deviations (or medians and interquartile ranges for those variables with skewed distributions). The normality of the distribution was checked using both skewness and kurtosis.
Comparison tests were performed to test for an association between family/patient characteristics and a positive HADS score. The categorical variables were compared using chi-square tests, while the continuous variables were compared using either Student’s t-test or the Mann-Whitney U test, depending on the normality of the distribution. A multivariable logistic regression model was constructed to identify the independent factors associated with a positive HADS score. The odds ratio (OR) and the associated 95% confidence intervals (CIs) were also reported. The multivariable logistic regression model included four variables from the univariate analysis that all had a p value <.10, namely smoking/drinking habits, personal history of psychopathology, unemployment and source of income threatened by the hospitalisation. The variables were chosen based on the number of positive outcome cases and the favourable associations identified via the univariate analysis.
All the reported p-values are two-tailed, with a p value <.05 indicating statistical significance. The analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 27).
Ethical approval
This study was approved by Hospital Pedro Hispano’s Ethics Committee prior to data collection (ethics registration no. 29/CE/JAS). The family members were informed about the research, and they all signed a written consent form that assured them the anonymity and confidentiality of their data would be maintained, while also explaining the purpose of the study and the usefulness of the predicted results. This consent form was signed by each family member during their relative’s ICU stay. The family members acted as surrogates for the patients with regard to the provision of written consent to participate in the study.
Results
Participants
The total number of families approached regarding participation in the present study was 291. Among them, 17 family members were not included because their relatives died during the hospitalisation period, 82 family members were excluded because they missed the follow-up consultations and 28 family members did not consent to participate. Ultimately, the study sample included 164 patients who were hospitalised in the ICU of Hospital Pedro Hispano and their respective family members. A flow diagram of the study’s recruitment process is presented in Figure 1. Flow diagram of the study’s recruitment process.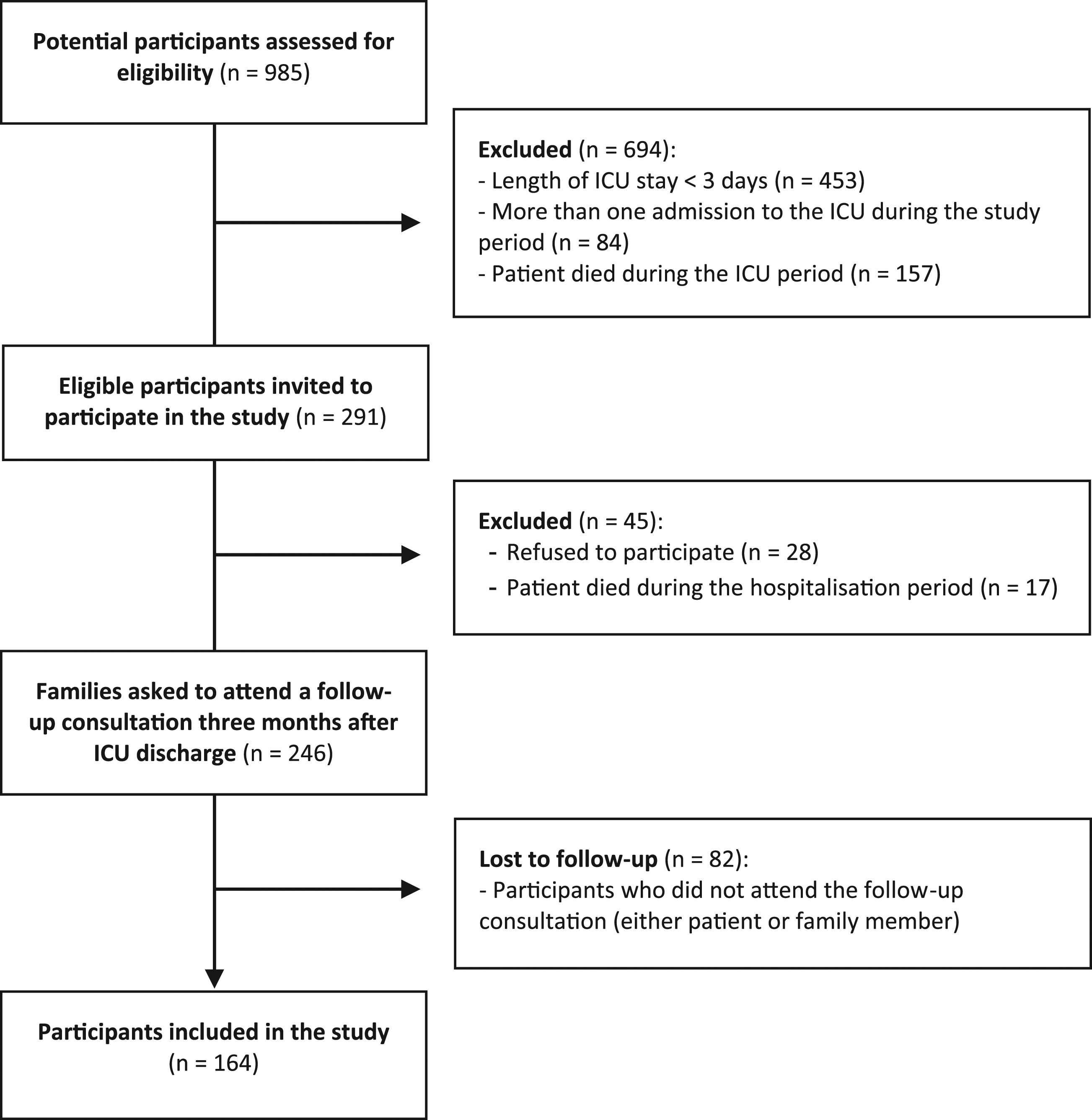
Participants’ characteristics
The family members’ mean age was 53.9 years (standard deviation [SD]: 14.7 years, range: 23–84 years). The majority of the family members were female (72.0%), and approximately half of them were the patients’ spouses (48.8%). A personal history of anxiety, depression, insomnia or other psychiatric disorder was reported by 61.6% of the family members, with 39.0% of the sample reporting using psychiatric medication. Smoking or drinking habits were reported by 25.0% of the family members, meaning that these individuals performed the relevant habit daily and recognised themselves as having a physical/psychological dependency. Approximately half of the family members already had experience of being a caregiver (51.8%), which was defined as experience of taking care of a dependent adult due to old age, sickness or disability.
The majority of the families included in this study had a nuclear structure (61.3%), referring to a family unit consisting of two adults and any number of descendants living together. Moreover, most of them reported facing socioeconomic constraints (67.1%), meaning that the family’s income was just sufficient or not enough to cover their minimum expenditure. Unemployment was reported by 14.6% of the family members, while 24.4% stated that their source of income was threatened by the patient’s hospitalisation. The demographic characteristics of the family members are presented according to the patients’ outcomes in Table 1.
Characteristics of patients admitted to the ICU according to the outcome (family member’s HADS score).
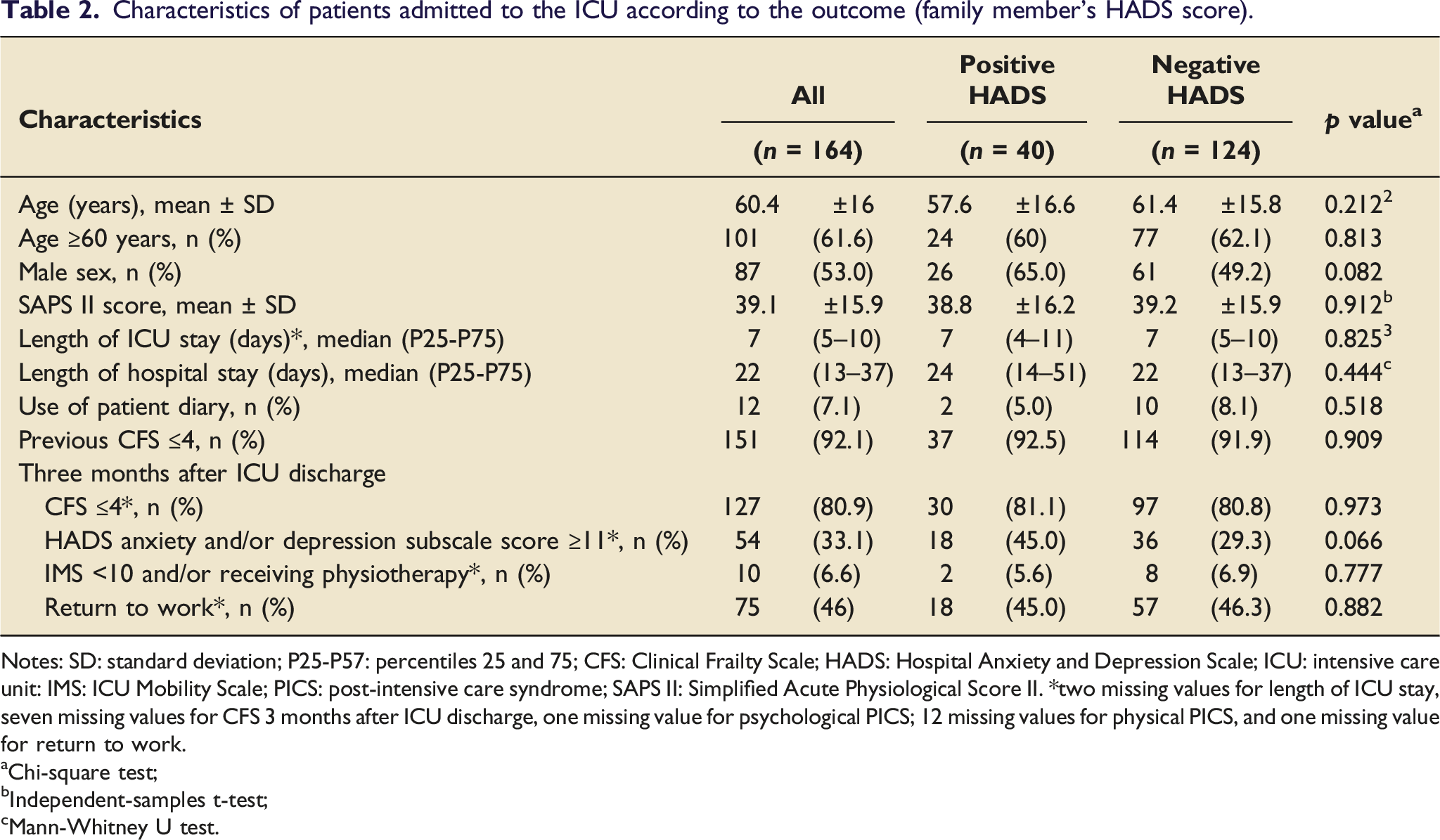
Notes: SD: standard deviation; P25-P57: percentiles 25 and 75; CFS: Clinical Frailty Scale; HADS: Hospital Anxiety and Depression Scale; ICU: intensive care unit: IMS: ICU Mobility Scale; PICS: post-intensive care syndrome; SAPS II: Simplified Acute Physiological Score II. *two missing values for length of ICU stay, seven missing values for CFS 3 months after ICU discharge, one missing value for psychological PICS; 12 missing values for physical PICS, and one missing value for return to work.
Chi-square test;
Independent-samples t-test;
Mann-Whitney U test.
Descriptive data concerning the outcome
Emotional distress was detected in 24.4% of the family members, as determined by a HADS score indicating the probable presence of either anxiety or depression (score ≥11). The HADS questionnaire is divided into the HADS anxiety subscale and the HADS depression subscale. With regard to the HADS anxiety subscale, 60.4% of the family members had a score in the normal range (score 0–7), 17.7% had a score suggestive of the presence of anxiety (score 8–10) and 21.9% had a score indicating the probable presence of an anxiety disorder (score of 11 or higher). In terms of the HADS depression subscale, 81.8% of the family members had a score in the normal range (score 0–7), 9.1% had a score suggestive of the presence of depression (score 8–10) and 9.1% had a score indicating the probable presence of a depressive disorder (score of 11 or higher).
The mean score for the HADS anxiety subscale was 7.0 points (SD: 4.5), while the mean score for the HADS depression subscale was 4.2 points (SD: 4.0). Thus, the levels of anxiety experienced by the family members surpassed their depression levels.
Of the 40 family members who had a HADS score indicative of emotional distress, 11 individuals (27.5%) had high scores (score ≥11 points) for both the anxiety and depression subscales, while 25 (62.5%) had a high score for only anxiety and 4 (10.0%) had a high score for only depression.
Univariate analysis
A significant association was found between a positive HADS score (indicating emotional distress) and the following characteristics on the part of the family members: unemployment (p = .008), a personal history of psychopathology (anxiety, depression, insomnia or other psychiatric disorder) (p = .045) and the presence of smoking/drinking habits (p = .036). The odds of the family members having a HADS score indicative of emotional distress was found to be 3.23 times higher among the unemployed family members when compared with those who were employed or retired (OR: 3.23 [95% CI: 1.32–7.97]), 2.24 times higher in the family members with a personal history of psychopathology when compared with those with no such history (OR: 2.24 [95% CI: 1.01–4.98]) and 2.26 times higher in the family members who reported smoking or drinking habits when compared with those who did not report such habits (OR: 2.26 [95% CI: 1.05–4.90]).
Several other characteristics on the part of the family members also appeared to be related to an increased likelihood of a positive HADS score. For instance, a higher prevalence of emotional distress was found in the spouses when compared with the non-spouses (57.5% vs 42.5%), in the family members who had prior experience of being a caregiver when compared with those with no such experience (60% vs 40%) and, more predictably, in the family members who had a personal history of anxiety, depression or another psychiatric disorder when compared with those with no such history (75% vs 25%). Although this study found no statistically significant association between these three characteristics and the presence of a positive HADS score, it is still important to highlight their potential relevance.
When examining the association between the family members’ HADS scores and the patients’ characteristics, we found that family members with a positive HADS score were more frequently related to male patients and to patients who reported a positive HADS score 3 months after ICU discharge. However, while these tendencies were observed, no evidence was found of a significant association between the patients’ characteristics and the family members having a HADS score indicative of emotional distress.
Multivariate analysis
Univariate and multivariate analyses of the key risk factors and the incidence of emotional distress in family members.
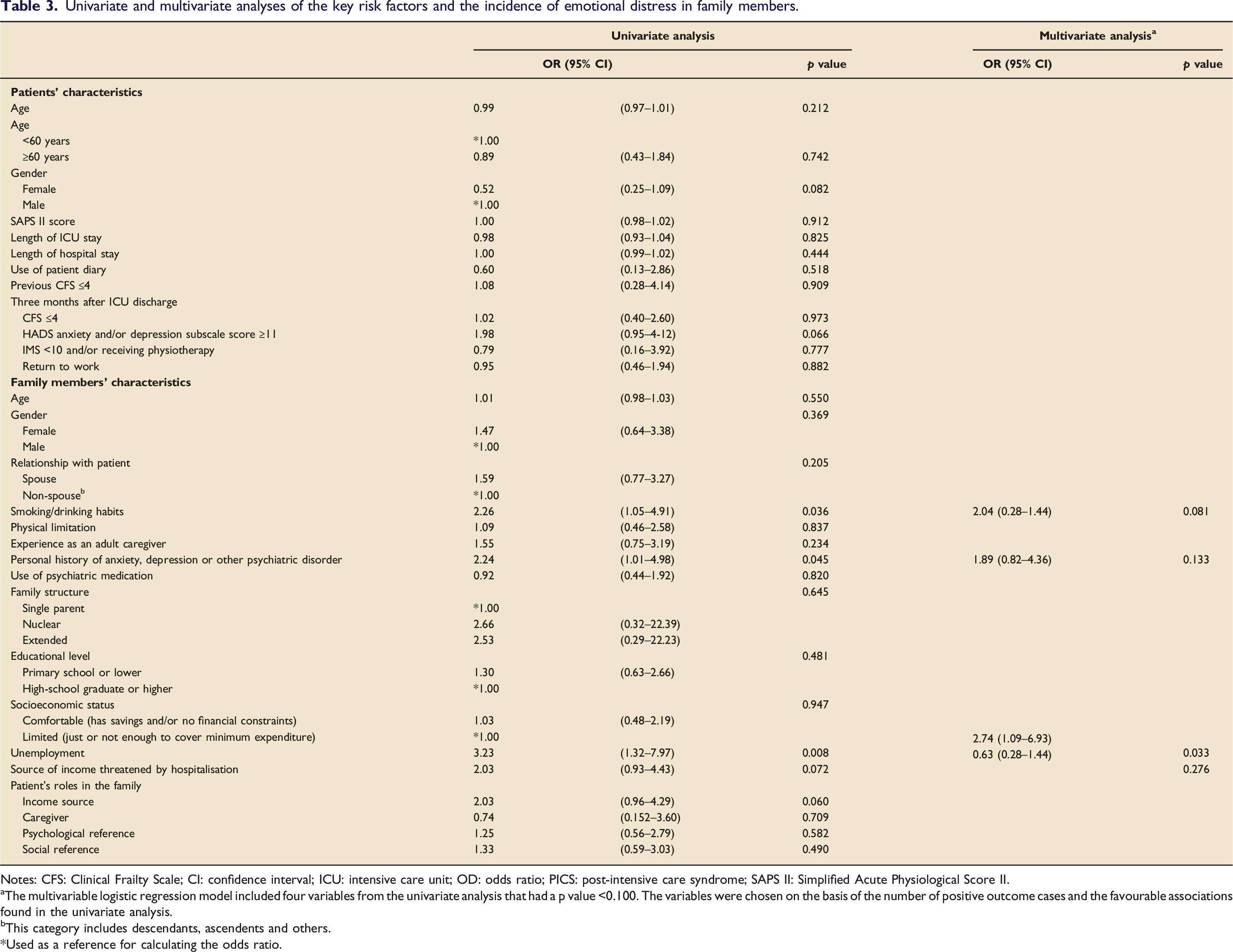
Notes: CFS: Clinical Frailty Scale; CI: confidence interval; ICU: intensive care unit; OD: odds ratio; PICS: post-intensive care syndrome; SAPS II: Simplified Acute Physiological Score II.
The multivariable logistic regression model included four variables from the univariate analysis that had a p value <0.100. The variables were chosen on the basis of the number of positive outcome cases and the favourable associations found in the univariate analysis.
This category includes descendants, ascendents and others.
*Used as a reference for calculating the odds ratio.
Discussion
Emotional distress, as manifested in the symptoms of anxiety and/or depression, is a potential marker of PICS-F. In this study emotional distress was measured with the HADS score and identified in 24% of the family members. This finding is consistent with the findings of prior studies that have established such symptoms to be common in the family members of ICU patients, with the reported prevalence rates ranging from 15% to 74%.17–23
Interestingly, 61.6% of family members reported a history of anxiety, depression or other psychiatric disorders in the socio-demographic questionnaire. This higher prevalence, when compared to anxiety/depression measured with the HADS score (24%), may be justified by the fact that the HADS score explores only manifestations of anxiety and depression, leaving out other psychiatric disorders. Additionally, researchers did not differentiate past from current history of these disorders, which may justify a higher overall prevalence. Lastly, family members that have been diagnosed with anxiety/depression may have adequate mental health counselling and/or medication, possibly reducing the likelihood of the development of symptoms related to the ICU experience and, therefore, a positive HADS score. Future studies on this matter would benefit from a more detailed survey regarding the participant’s medical history of psychiatric disorders.
Other studies have explored family members’ characteristics as possible predictors of PICS-F and determined that the female gender,20,22,24,25 a young age,22,23,26 a conjugal relationship with the patient,20,21 cohabitation with the patient, 23 the presence of a pre-existing mental health disorder(s) 25 and recent personal experience of serious physical illness 25 all appear to predispose family members to PICS-F.
In addition, several studies have analysed gender differences in terms of the global prevalence of anxiety and depression and found higher rates of these mental disorders among those of the female gender.27–30 Our study population was mainly composed of female individuals (72% of the family members), which could indicate selection bias. However, the percentage of female family members with a positive HADS score was only slightly higher than the percentage with a negative HADS score (77.5% vs 70.2%), while no evidence of a significant association was found between gender and a positive HADS score (as the outcome of interest).
In the present study, several personal traits were found to be associated with the presence of emotional distress among the family members of ICU patients, although unemployment was the only trait determined to be independently associated with the outcome, which represents the main finding of the study.
To the best of our knowledge, this is the first study to identify unemployment as a risk factor for emotional distress among the family members of ICU patients. In a prospective study, Fumis et al. compared the mental health outcomes of the family members of patients from different socioeconomic backgrounds who were admitted to the ICUs of two Brazilian hospitals, one private and one public. The authors found that the symptoms of depression were worse in the public hospital group, a population with a significantly lower monthly income and an unemployment rate of 33%, 31 which is in line with the findings of the present study. No data was found regarding the prevalence of anxiety and depression within a healthy Portuguese unemployed population, which limits a comparison with the findings of this study.
During the years in which this study was conducted, the mean unemployment rate in Portugal was 7.5%, 32 although among the study population the unemployment rate was found to be significatively higher (15%). Unemployment has for long been associated with emotional instability, as it represents a threat to the individual’s self-esteem and economic security.33,35 In light of this, it is unsurprising that this personal trait is associated with emotional distress among the family members of ICU patients. Fortunately, unemployed family members can be easily identified through interviews with ICU staff, making it possible for the prompt acknowledgment of at-risk family members and an earlier referral for social care and psychological support (if required).
PICS-F represents a response to critical illness that is experienced by the family members of ICU patients. Moreover, it includes new or aggravated psychological symptoms arising from the experience of their relatives’ hospitalisation. PICS-F may be experienced in the form of symptoms of anxiety, depression, post-traumatic stress disorder or other expressions of emotional suffering. Our study sought to examine the manifestations of anxiety and depression on the part of family members after their relatives had been discharged from the ICU in order to identify the risk factors associated with PICS-F. One limitation with regard to this study concerns the fact that the authors remained unaware of the family members’ mental health status and HADS scores prior to their relatives’ stay in the ICU, which raises doubt as to whether they were already under emotional distress prior the hospitalisation and how much of that distress was aggravated by the patients’ time in the ICU and the subsequent recovery process.
The fact that critical illness is typically unpredictable and commonly arrives unannounced makes it hard to know the family members’ previous HADS in advance of their relatives’ hospitalisation. Nevertheless, the prevalence of anxiety reported in this study’s findings presents as significantly higher than that of the general population, more specifically a healthy older adult Portuguese population, as stated in the work by Sousa et al. 35 If we take these findings into consideration, it is possible to conclude that the emotional distress observed in the family members in this study may be new or aggravated by their ICU experience, which suggests that they may be an expression of PICS-F.
In terms of the data collection process applied in this study, no surrogate marker of the strength of the relationship between the patient and their family member was gathered. The family member chosen for inclusion in the study was the one who met the inclusion criteria, identified themself as the principal informal caregiver after patient’s hospital discharge and, simultaneously, was most frequently present during visiting hours in the ICU. This was determined by the research team based on a subjective analysis, which may indicate selection bias.
Loss to follow-up occurred in approximately 30% of the families (both patients and family members) invited to the follow-up consultation, resulting in a reduction in the expected sample size. These losses may interfere with the strength of our findings and, therefore, must be pointed out. The number of family members lost to follow-up was increased by the fact that we excluded the family member if the respective patient failed to attend the follow-up consultation.
The patients’ characteristics, namely age, length of ICU/hospital stay, severity of illness and frailty status after ICU discharge were not found to be related to the expression of emotional distress among family members. This finding is supported by the findings of similar studies that did not identify a consistent association between patients’ variables and family members’ outcomes.20,25,27 Although other studies have noted a lack of correlation between patients’ illness severity and the symptoms of anxiety and depression among their family members, our findings do not allow for such a specific analysis, as the study sample is most likely skewed in terms of its distribution. The family members of patients who died during the hospitalisation period, that is, most likely the patients who were most severely ill and so had higher SAPS II scores, were not included in the study sample. This subgroup was excluded from the analysis because manifestations of complicated grief may be easily confused with manifestations of burden and emotional distress related to the ICU admission exhibited by family members. The fact that this subgroup was excluded may also have had an impact on the observed HADS scores, since these family members are likely to experience more distress during their relatives’ acute illness.
The lack of an association between the patients’ variables and the family members’ outcomes makes it more difficult to identify at-risk individuals and raises doubts as to whether changes in patient care alone could help to prevent the experience of PICS-F by family members.
It is possible (and likely) that other factors influencing family members’ mental health and wellbeing have been overlooked in this study. Moreover, a weakness of the present investigation lies in the fact that a subset of factors related with the ICU’s standard of care, which have previously been found to be associated with the development of anxiety, depression and post-traumatic stress disorder,17,20,36 were not explored. These factors include the time allowed for family visits, the regularity of nurse and/or physician meetings with family members, the consistency and quality of the information provided and the physical conditions of the ICU environment. Although these factors already form part of the standard of care we aim to deliver at our ICU, we believe that investigating them further would be particularly relevant because they are easily modifiable by ICU staff.
A deeper awareness of PICS-F and increased knowledge of the risk factors associated with it are essential for the development of effective prevention strategies. Several studies have proposed preventive measures for PICS-F and shown the reduction of emotional distress on the part of family members following their implementation, including a reduction in post-traumatic stress-related symptoms in families with access to an ICU diary37,38 and a reduction in anxiety and depression symptoms among family members in contact with a psychologist during their relatives’ ICU stay. 39 To the best of our knowledge, no prior study has used family members’ characteristics to identify those individuals in need of particular support during their relatives’ ICU stay. Yet, if more was known about both the risk factors for PICS-F and individual susceptibility, more personalised care could be provided to family members in order to prevent the manifestation of emotional distress in this context.
In conclusion, the findings of this study indicate an association between family members’ emotional distress and their personal traits, thereby extending the prior literature by suggesting that patients’ characteristics are less relevant to the experience of PICS-F. Unemployment may represent a meaningful risk factor for emotional distress in family members (a potential marker of PICS-F), given its relationship with positive HADS scores among the family members of patients following their ICU discharge. These findings may help to improve prevention strategies concerning PICS-F by indicating the need to assess family members’ characteristics and demographics early on during their relatives’ ICU stay and, consequently, allowing for the early identification of at-risk individuals and the timely implementation of adequate support services.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.