
Abstract
The COVID-19 pandemic has generated renewed interest in the psychological rehabilitation needs of patients admitted to intensive care units. While the availability of embedded practitioner psychologists within adult critical care teams remains inconsistent, post numbers have increased in response to the clinical needs of the pandemic. As psychology services within adult critical care become more widely established, models for service provision will be required. We describe our experience of developing a model for the delivery of a clinical psychology service within critical care in a District General Hospital with specialist tertiary surgical and cancer services. The current paper describes a service design that is firmly rooted in psychological theory and the broader clinical health psychology evidence base. We hope that our learning will be helpful to others.
Introduction
The role of practitioner psychologists in critical care rehabilitation has been recognised for some time within national guidelines;1,2 yet, the availability of services remains inconsistent.
As more practitioner psychologists are appointed to work in critical care, models for service provision will be required. We describe our model for a clinical health psychology service.
The rationale for an embedded clinical health psychology service
The prevalence of psychological, cognitive and functional difficulties following intensive care units (ICU) admission is well documented
3
and ‘post-intensive care syndrome’ (PICS) is a recognised long-term condition (Figure 1). There is evidence supporting the benefits of integrating psychology throughout the critical care pathway. Domains of post-intensive care syndrome.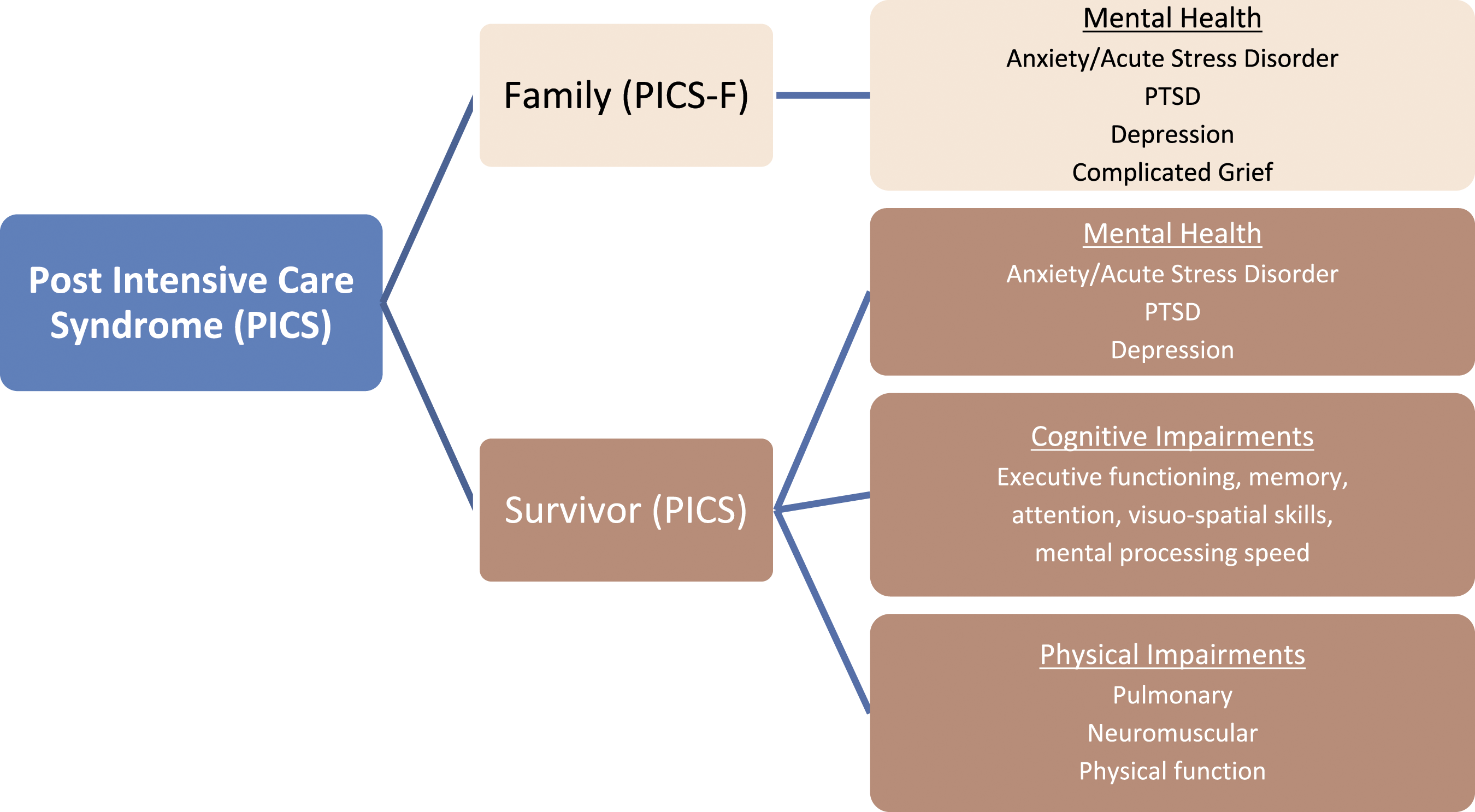
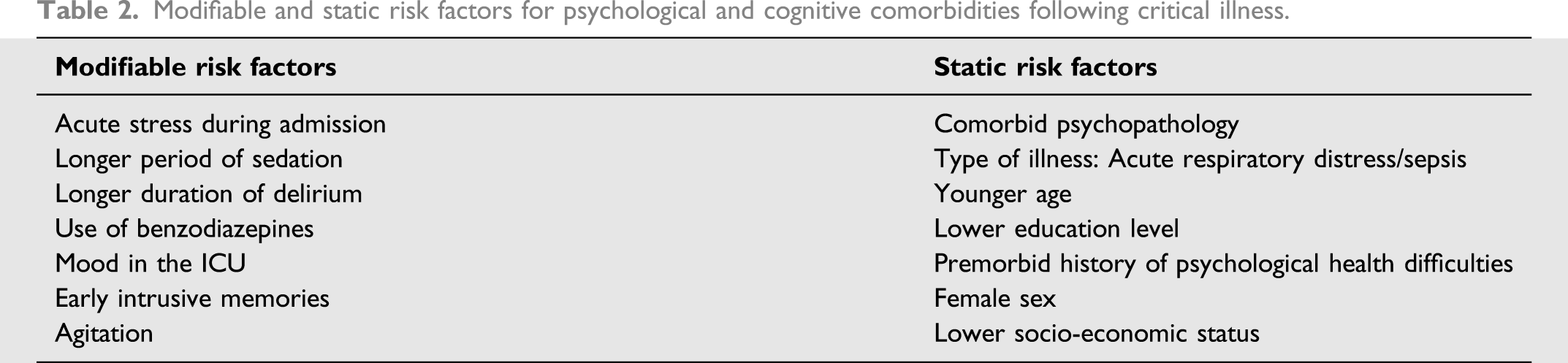
Modifiable risk factors for psychological and cognitive comorbidities may be addressed during admission. Acute stress predicts psychological morbidity post-discharge 3 and psychological screening and interventions may reduce this. 4 Delirium screening and the implementation of neuro-rehabilitative management approaches help improve long-term neuropsychological outcomes. 5 A summary of the evidence for the application of psychological theory to critical care rehabilitation is available. 6
Following discharge, psychological therapies are recommended in the treatment of PTSD, anxiety and depression. Practitioner psychologists within intensive care units bring knowledge of the critical care context to outpatient work. The effectiveness of exposure-based interventions benefits from access to the critical care environment and medical colleagues.
While the relatively novel status of clinical health psychology in adult critical care means that cost-effectiveness data is lacking, evidence from other long-term conditions is relevant. For example, patients with cardiovascular problems and comorbid mental health difficulties remain admitted to hospital for longer, with total costs increasing by 49%. 7 Following outpatient cognitive-behavioural treatment hospital admissions fell, representing a cost reduction of £2000 per person. In PICS, when symptoms remain unaddressed persistent cognitive impairments predict a reduction in employment status at 12 months. 8
A sufficiently resourced clinical health psychology service can also offer psychological care to families and promote strategic approaches to improving staff wellbeing.
Service design
Underlying philosophy
Our service promotes optimal recovery outcomes by preventing and treating psychological, cognitive and behavioural difficulties associated with PICS.
The service achieves this by promoting an ethos that considers psychological rehabilitation to be everyone’s responsibility and that all patients will have psychological needs of differing complexity.
Most psychological care is provided via ‘treatment as usual’, delivered by the multi-disciplinary team who are trained to create a psychologically informed service at all levels. Nurse-led preventative psychological interventions are not supported by existing evidence 9 so patients with more complex needs are assessed by the psychology service.9,10
Psychology staffing and governance
Our ICU admits approximately 1400 people per annum. There are around 24 patients daily including level 2 and level 3 dependency. Bed number is not necessarily a reliable proxy for the required psychology hours to provide an effective service; case mix and complexity need to also be considered.
Within our model, the breadth of role and the importance of integration requires a post of at least 0.5 whole time equivalent. The post’s banding at 8b fits with the Agenda for Change Framework and reflects the nature, complexity and autonomy of the role.
Implementing an effective governance framework is important to promote best practice. We believe psychology posts are optimally embedded within existing clinical health psychology teams, if available. The clinical psychologist is managerially accountable to the ICU clinical director and clinically accountable to standards set by the HCPC and the supervising consultant clinical psychologist.
The inpatient service
Screening and assessment
The predictive function of inpatient acute stress 3 for psychological difficulties post-discharge means it is important to begin early screening and assessment for acute stress.
The Intensive Care Psychological Assessment Tool (IPAT) 11 is an acute stress screening tool. Within our service, a score of seven or above indicates a need for enhanced psychological care from the team. 11 A higher threshold of 11 or above triggers referral to the psychology service, to match clinical need with treatment intensity. The nursing team also screens patients for delirium using validated tools.
Direct inpatient interventions
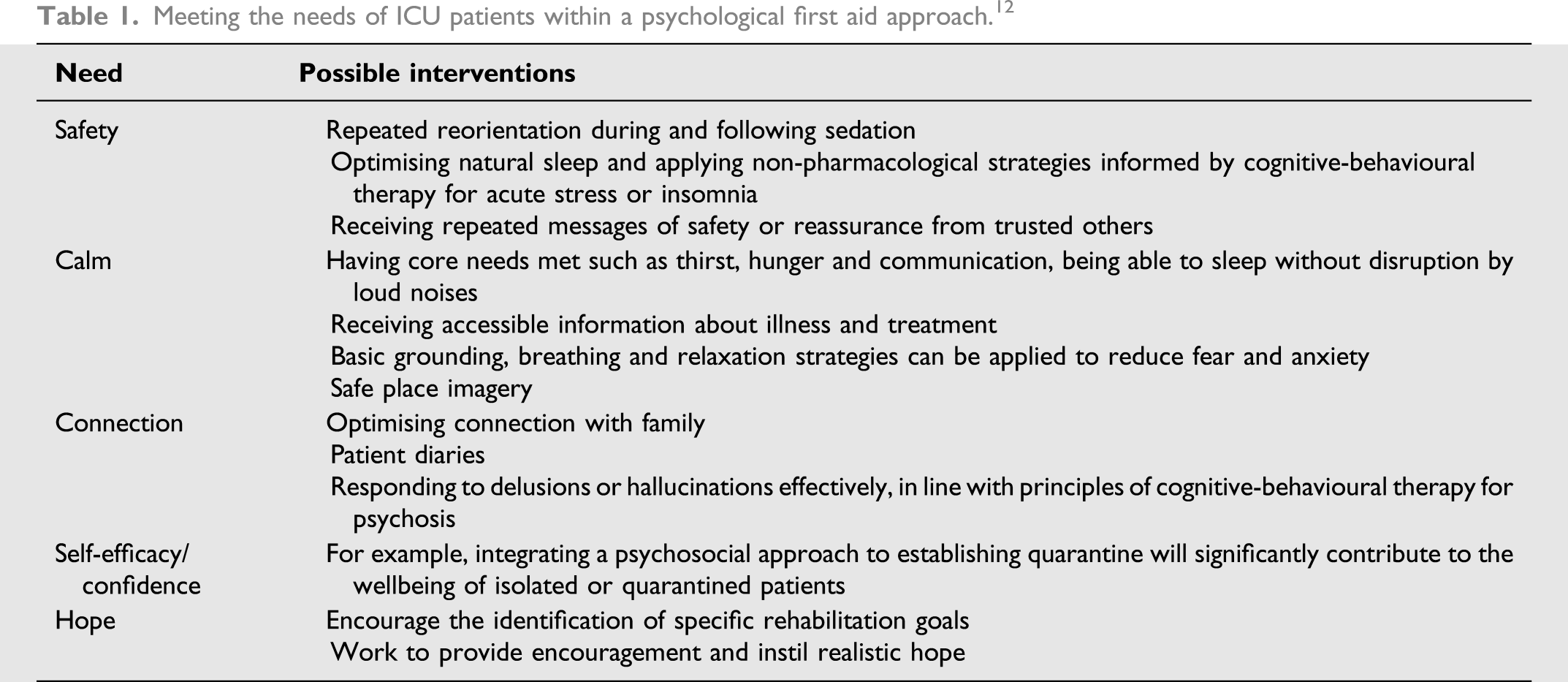
Two models commonly applied within inpatient work include Psychological First Aid 12 and cognitive-behavioural therapy (CBT). Both facilitate a sense of relational, physical and psychological safety during an ICU admission.
Psychological first aid
Meeting the needs of ICU patients within a psychological first aid approach. 12
Cognitive-behavioural therapy for acute stress
Principles of CBT for acute stress 13 can be applied, which appear both acceptable and feasible for critical care patients.14,15 This involves development of a ‘clinical formulation’, which refers to a theoretically grounded way of making sense of an individual’s distress. A formulation draws on evidence-based theoretical models to identify predisposing, precipitating, perpetuating and protective factors and guides intervention.
CBT techniques commonly drawn upon within inpatient work are described below. These share a simplicity that make them accessible within brief consultations to people who may be sleep deprived or cognitively impaired.
Behavioural activation
Learning theory proposes that low mood during a critical care admission can result from losing contact with sources of intrinsic reward, enjoyment or satisfaction. Once a person feels low in mood, motivation and activity reduce, leading to further reduced contact with intrinsic reward. A behavioural approach to this vicious cycle involves increasing contact with sources of reward in the absence of motivation. 16 Even within the context of an ICU admission where activity is limited, learning theory proposes that improvements in mood can be achieved through an emphasis on activity monitoring and scheduling. For example, by scheduling visits or rehabiliation sessions and monitoring behavioural and emotional outcomes.
Cognitive-behavioural models of anxiety
Cognitive-behavioural models of panic disorder propose that panic attacks occur when people experience symptoms of anxiety and appraise these symptoms in a catastrophic way, exacerbating the threat response. Similarly, cognitive-behavioural models can be applied to address psychological barriers to respiratory weaning, particularly when anxiety is maintained by appraisals regarding the meaning of unpleasant yet benign symptoms of weaning. 17 Formulation is key to understanding whether a physiological sensation is triggering distress due to misattribution, association with a trauma memory, discomfort or another cause.
Elaboration of trauma memories
Cognitive-behavioural models of post-traumatic stress 18 suggest that the fragmented and incoherent nature of trauma memories contributes to the maintenance of a sense of current threat. Sedation, analgesia, delirium and sleep deprivation may increase fragmentation of episodic memories. While acknowledging the evidence against intervening within the first 4 weeks following a psychological trauma to avoid interrupting the normal process of adjustment, national guidelines also recommend CBT for acute stress. The clinical psychologist works alongside multi-disciplinary colleagues to provide accessible information to patients who wish to elaborate memories.
Stimulus discrimination
The way in which trauma memories are processed mean ICU patients may experience intrusive, involuntary recall of traumatic memories characteristic of an acute stress response. 13 Helping inpatients learn to deliberately notice internal and external differences between stimuli experienced ‘then’ (at the time of the trauma) and ‘now’ (in the present moment) can reduce distress.
Functional analysis
Functional analysis provides a tool to examine the antecedents and consequences of behaviour. During an ICU admission, the behaviours people use to cope are contextual and therefore influenced by the environment and the consequences of a coping response. A functional analysis can collect information about triggers and consequences of coping responses help to understand a behaviour and guide behaviour change strategies when required.
Psychoeducation
Providing information regarding the cause, meaning and usually transient nature of hallucinations, flashbacks or circadian rhythm disturbance can help to reduce acute stress. A tendency to ‘catastrophise’ regarding the meaning of ambiguous or threatening events refers to a cognitive distortion where we overestimate the ‘awfulness’ of an event and underestimate our ability to cope should it re-occur. For example, ‘I’ve lost my mind’. Providing accessible information to explain symptoms associated with delirium can help patients to ‘de-catastrophise’ the meaning of symptoms and reduce distress.
Diversifying emotional regulation strategies
Existing regulation strategies may be unavailable to patients during admission (for example, socialising or exercise) and therefore diversifying strategies may be helpful. Grounding techniques are a basic tool for helping people to reduce acute anxiety. Mental images can produce strong emotional reactions and emotions are often associated with spontaneous images. 19 Given that our emotional responses can respond similarly to real and imagined images, encouraging patients to use images they associate with safety can reduce distress.
Working with families
Involving families in their relative’s care (for example, filling gaps in the patient’s episodic memory) and providing information that helps families understand the ICU context (for example, regarding the meaning of alarms and delirium) may reduce the likelihood of relatives experiencing helplessness and other psychological sequelae.
Indirect inpatient interventions
Indirect interventions may have broader systemic influence than individual level interventions and help to develop a more psychologically informed critical care unit.
Patient diaries
A review of the patient diary literature relating to outcomes, governance and consent is available elsewhere, 20 but briefly patient diaries are completed by staff and relatives during an inpatient admission and returned to patients following discharge to help develop a more coherent narrative of admission. Initially, patient diaries were conceptualised as a preventative intervention for post-traumatic stress; however, literature does not consistently support this function. 21 Rather, psychological trauma theory supports the importance of helping people create coherent, elaborated memories of traumatic experiences 18 and patient diaries therefore constitute an important resource within a broader rehabilitation package. There is evidence that patient diaries can reduce depression rates following discharge 20 and risk of psychological trauma in family members. 22
Consultation
Consultation involves working with other healthcare professionals to make sense of how a patient is behaving, drawing on psychological theory. Common areas for consultation include understanding and responding to difficulties with patient engagement in rehabilitation. For example, if a patient appears low in mood a response might be to consider anti-depressant medication. While this is understandable, the response itself risks pathologising normal psychological reactions, risks the under-diagnosis of hypoactive-delirium and would not be indicated without evidence of moderate-severe depression. The psychology service aims to offer an alternative perspective within these discussions, providing an informed rationale regarding why in some cases a psychological or pharmacological intervention may or may not be warranted. 23
Training
The clinical health psychology service provides training to multi-disciplinary colleagues. For example, the CBT for psychosis literature emphasises how confronting or disputing the content of delusions can (1) interfere with the development of a trusting relationship and (2) lead to an increase in the intensity with which beliefs are held 24 Training therefore includes experiential practice in how responding with empathy, warmth and genuineness may help delirious patients feel safer and understood.
Promoting natural sleep
Disturbed sleep architecture in the ICU is associated with delirium and adverse pulmonary, cardiovascular and immunologic outcomes. 25 For example, REM sleep performs an important role in the processing of recent emotive experiences and when REM sleep is lacking the strength of affect within an autobiographical memory network persists, resulting in the potential for psychological sequalae. 26 Furthermore, sleep disturbance occurring in the aftermath of a traumatic experience is associated with an increased risk of PTSD. 27
Sleep medication may be used to improve sleep in the ICU, despite achieving small effect sizes of questionable clinical significance 28 undermining sleep architecture 29 and the risk of rebound insomnia. There is insufficient evidence to suggest that pharmacotherapy improves sleep in hospitalised patients. 30 Rather, cognitive-behavioural therapy for insomnia (CBT-I) is recommended as first line 31 and is more effective than medication in addressing numerous problematic aspects of sleep. 32 Brief behavioural treatments for sleep difficulties are efficacious, supporting their application within inpatient medical contexts. 33
Non-pharmacological strategies for delirium
In line with the ABCDEF bundle, 34 the psychologist can work with multi-disciplinary colleagues to reduce environmental triggers and formulate reasons for agitation (for example, discomfort, thirst and isolation). Modifiable risk factors for delirium can be addressed, including eliminating benzodiazepine use and optimising contact with family. 35 Sedatives or antipsychotics are often prescribed to address associated agitation, but have potentially harmful side-effects and do not influence severity or length of delirium. 36
Current evidence supports neither pharmacological nor non-pharmacological strategies to reduce the duration of delirium in critically ill patients, so prevention is prioritised.
Following discharge from the intensive care unit
Ward follow-up allows ongoing psychological assessment and treatment to continue, particularly when a range of factors (pain, sleep deprivation, the effects of medication and confusion) have prevented patients accessing the service during their ICU admission.
Our model for intensive care unit follow-up clinics
Modifiable and static risk factors for psychological and cognitive comorbidities following critical illness.
Our model favours inter-disciplinary rather than multi-disciplinary team working. Within ‘multi-professional’ clinics, professionals treat the patient independently while in ‘inter-disciplinary’ clinics effective care is accomplished through the interaction between the patient and team members, with responsibilities shared and decisions made collectively. 37 Within rehabilitation teams, inter-disciplinary working is found to achieve better results for nearly every aspect of team effectiveness. 38 In terms of clinic leadership, we are guided by evidence defining the nature of optimal leadership within inter-disciplinary health teams, which recommends inclusive leadership and the promotion of non-hierarchical structures. 39
In practice, this involves each team member accepting responsibility for stepping in and out of the leadership role in clinic when their expertise is required. We strive to operate the clinic in a non-hierarchical manner; we sit with the patient in a circle, away from desks and set an agenda that is guided by the patient’s rehabilitation concerns.
While evidence for the effectiveness of follow-up clinics is inconclusive
40
our experience is that follow-up clinics do not usually function as an isolated intervention. Indeed, the only outcome we routinely measure is patient satisfaction. Helpful functions include: 1. Assessment of post-intensive care syndrome 2. Normalising biopsychosocial consequences of ICU admission. 3. Constructing a timeline of admission. 4. Re-visiting the ICU as a means of updating episodic memories. 5. Facilitating onwards referrals. 6. Assessment of how health beliefs may be influencing rehabilitation behaviours. This is important, given the well-established findings within the broader rehabilitation literature that health beliefs are more predictive of return to work,41 attendance at rehabilitation42 and re-admission to hospital43 than measures of illness severity.
Outpatient clinical health psychology service
The service also provides evidence-based outpatient psychological interventions, as recommended by the Guidelines for Provision of Intensive Care Services II. 1
Common presentations include adjustment to physical limitations, depression, anxiety disorders, PTSD and persistent cognitive impairments.
A common theoretical model informing formulation and treatment is the Cognitive Model of PTSD. 18 This model suggests that people with PTSD experience a persistent sense of current threat characterised by intrusions (for example, nightmares and flashbacks), strong emotions and hyperarousal. This sense of current threat is created by (i) excessively negative appraisals of the trauma and its consequences and (ii) characteristics of the trauma memories that lead to re-experiencing symptoms. This sense of current threat is perpetuated by cognitive and behavioural control strategies, which maintain threat by preventing change in the appraisals and trauma memory.
Psychological treatment over 8–12 sessions 44 therefore involves 1 modifying excessively negative appraisals 2 ; reducing re-experiencing symptoms by elaborating trauma memories; and 3 reducing counterproductive control strategies. Formulation is crucial to understanding how physical, cognitive and psychological symptoms are interacting.
The service works closely with primary care providers of psychological therapies. Onwards referrals are made when a patient would not specifically benefit from seeing a psychologist who understands the ICU context. The clinical health psychology service also provides training to local services and therefore a reciprocally supportive relationship has developed.
If patients report persistent cognitive impairments, a cognitive screen such as the Montreal Cognitive Assessment (MoCA) 45 would be administered. Patients who meet inclusion criteria for local neurorehabilitation or memory clinics would be referred. More often the cognitive changes patients report are formulated within a differential diagnosis model (which considers both psychogenic and organic causes). In such cases, patients are given information about the factors which may be contributing to their cognitive changes and a treatment plan agreed collaboratively. Patients may be offered adapted CBT, cognitive compensatory or rehabilitation strategies informed by the clinical interview, drawing on the limited available evidence.46,47 While formulation within the context of a full neuropsychological assessment would be optimal, this exceeds the resources of the service.
Staff health and wellbeing
The roles of the service in promoting staff health and wellbeing are multifaceted and underpinned by evidence that individual self-care strategies will only be moderately effective in reducing psychological distress. Far more protective will be the bonds between colleagues and social support within teams. 48 The service works alongside leaders to promote a caring and cohesive team dynamic; for example, promoting regular huddles and buddying systems, promoting models of compassionate leadership and emphasising the importance of social support between colleagues. The service organises surveys measuring individual 49 and team level factors of health.
The service facilitates opportunities for staff to talk about their experience of working on the unit. The model used to facilitate these sessions is ‘Schwartz Rounds’, which are associated with reduced distress, improved team work and enhanced social support. 50
Following potentially traumatic events on the unit, the service offers an active monitoring, 44 assessment and onwards referral function for staff in need. The service liaises with occupational health and primary care services to promote timely access to evidence-based therapies.
Conclusion
In light of the severity of the stressors associated with ICU admission alongside the prevalence of psychological and cognitive morbidities post-discharge, it is surprising that embedded ICU psychology services are not commonplace. One barrier to the development of services is perhaps uncertainty within acute medical teams regarding what practitioner psychologists actually do. This paper aims to elucidate this. The development of the Psychologists in Intensive Care UK (PINC-UK) Network indicates that this is a growing area of clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.