
Abstract
Aim
In the United Kingdom (UK), 600 deaths per annum are attributable to drowning. Despite this there is scarce critical care data on drowning patients globally. We describe drowning cases admitted to critical care units with a focus on functional outcomes.
Materials and Methods
Medical records for critical care admissions following a drowning event were retrospectively reviewed across six hospitals in Southwest England for cases presenting in the period between 2009 and 2020. Data was collected according to the Utstein international consensus guidelines on drowning.
Results
Forty-nine patients were included, 36 males and 13 females, including seven children. Median submersion duration was 2.5 min 20 cases were in cardiac arrest when rescued. At discharge 22 patients had preserved functional status, 10 patients had a reduced functional status. 17 patients died in hospital.
Conclusion
Admission to critical care following drowning is uncommon and associated with high rates of mortality and poor functional outcomes. We find that 31% of those who survived a drowning event subsequently required an increased level of assistance with their activities of daily living.
Introduction
Drowning is defined as the process of experiencing respiratory impairment from submersion or immersion in liquid, with outcomes classed as mortality, morbidity, or no morbidity.1,2 At least 372,000 people die following drowning per annum globally, with approximately 600 of these in the UK.2,3 There is limited information in the literature regarding patient centered outcomes following drowning related admissions to critical care units. Disability is common after critical illness and is important to patients, being associated with reduced self-reported quality of life. 4 This historical focus on mortality as a primary outcome has resulted in little understanding of patient morbidity following critical illness due to drowning.
Efforts to better understand drowning are hampered by inconsistent recording of variables in the published literature. This has made inferences from systematic review and meta-analysis difficult. Quan et al. (2016) performed a meta-analysis of at-scene predictors of drowning outcome based on 24 cohort studies including adults and children. 5 They found three factors significantly associated with more favourable outcomes: shorter submersion time, shorter EMS response times and drowning in saltwater. They note, however, that the quality of evidence to support prognostic factors “was low to very low.” A further systematic review of 49 papers in 2020 by Koon et al. found similar issues with key data missing such as CPR modality, pre-hospital airway management, functional and patient centered outcomes. 6
A consensus conference of resuscitation experts produced a tool for the uniform collection of data from drowning––the Utstein tool. 7 The aim of this was to standardise data collection in the field of drowning research, to enable more meaningful comparison, analysis and meta-analysis.
The United Kingdom (UK) is an island nation with a developed health care system, pre-hospital emergency medical services (EMS) and coastal lifesaving and lifeguarding services. The Maritime and Coastguard Agency (MCA) is responsible for the maritime UK Search and Rescue response, the co-ordination and delivery of which is managed by Her Majesty’s Coastguard (HMCG). These assets include HMCG Coastal Rescue Teams, the Royal National Lifesaving Institute (RNLI) Lifeboats and Lifeguard units, Independent Lifeboats, and UK Search and Rescue Air assets. On some occasions they can also call upon military assets, commercial vessels and volunteer teams. There is significant cross-over with the other statutory and voluntary emergency services who provide the majority of inland search and rescue capability. To the authors’ knowledge there is no peer reviewed data seeking to describe drowning cases in the UK in the past 20 years and what historic data there are pertain to paediatric drownings.8,9 The National Water Safety Forum maintains a database of inland and coastal drowning fatalities. This is known as the Water Incidents Database (WAID) and it records data from coroner reports, search and rescue organisations and individual submissions. The WAID database is limited in only including basic information on deaths and no data on non-fatal drownings. A more complete picture of non-fatal coastal drownings can be gleaned from MCA and RNLI data who publish annual statistics. The data behind these summaries lack the detail and breadth to satisfy Utstein standards, as they contain very limited clinical information and are confined to a single part of the patient journey (i.e. up to hospital). Due to these limitations in the available data, no UK drownings were included in recent landmark meta-analyses.5,6
Drowning victims have a wide range of trajectories through healthcare services depending on their severity of injury. Those with minor or no symptoms may be safely discharged with advice from the scene. 10 At the other end of the spectrum are those who are critically ill who have survived initial resuscitation attempts and will be admitted to a critical care unit. 10 This cohort is often admitted for a short period of ventilatory support. 11 Patients admitted to critical care following a drowning event represent a cohort of interest from which we may better understand predictors of drowning outcomes.
We aimed to collect data on drowning victims across multiple critical care units in the southwest of the UK using the Utstein Drowning tool. This study will describe drowning cases admitted to critical care and provide insights into the morbidity and functional outcomes following a drowning event.
Materials and methods
This retrospective notes review was conducted in critical care units across six acute NHS Trusts in the South-West Anaesthesia Research Matrix (SWARM): Northern Devon, Royal Devon & Exeter, Royal Cornwall, Somerset, Torbay and South Devon and University Hospitals Plymouth. Cases were identified using the Intensive Care National Audit & Research Centre (ICNARC) Case Mix Programme Database with an admission reason being “Drowning (fresh or salt water)” between the first of January 2009 and 31st of December 2020. The Case Mix Programme is a national, comparative audit of patient outcomes from critical care. Patients of all ages were included. ICNARC data on functional outcomes at discharge was also used with permission. This expected dependency post hospital discharge is a subjective prediction by a clinician based on the personal assistance likely to be needed for daily activities include bathing, dressing, going to the toilet, moving in/out of bed/chair, continence and eating. 12 Once identified, notes were reviewed by a local investigator as part of registered clinical audit projects at each Trust. Variables were extracted according to the Utstein tool for drowning. 7 Initial observations were taken from the pre-hospital phase of care, or upon attendance in the emergency department if the former were not available.
Water temperature is a variable of interest. When not recorded in medical records a specific water temperature was estimated from historic water temperature data. 13 Where a specific estimate was not possible due to location, as per Utstein standards a binary categorisation of icy or non-icy was applied. This was estimated by the authors based on the time of year, seasonal air temperature data and the size and type (fresh, salt, indoor, outdoor) of the body of water in question.
Data was compiled and analysed using the R programming language. 14 The central tendency of non-parametric continuous variables are represented by their median and their spread by interquartile ranges. Categorical variables are represented by percentages with the denominator being the number of complete cases (we report data completeness in Supplementary Table 1).
Results
Forty-nine cases were admitted to participating critical care units over the 11 year period. This cohort consisted of 36 males and 13 females between the ages of 1 and 89 years. There were seven cases in children ≤18 years of age. Most cases occurred in the summer months (39%) and in the afternoon (47%). In all cases the water was not icy. The specific water temperature was documented in 17 cases and estimated from historic data in a further 8 cases (see Figure 1). Box and whisker with jittered points indicating spread of temperatures at the first available recording, first hospital recording and corresponding water temperature. Many of the initial temperatures were unrecordably low and are not plotted here. Background colour relates to the y-axis for illustrative purposes.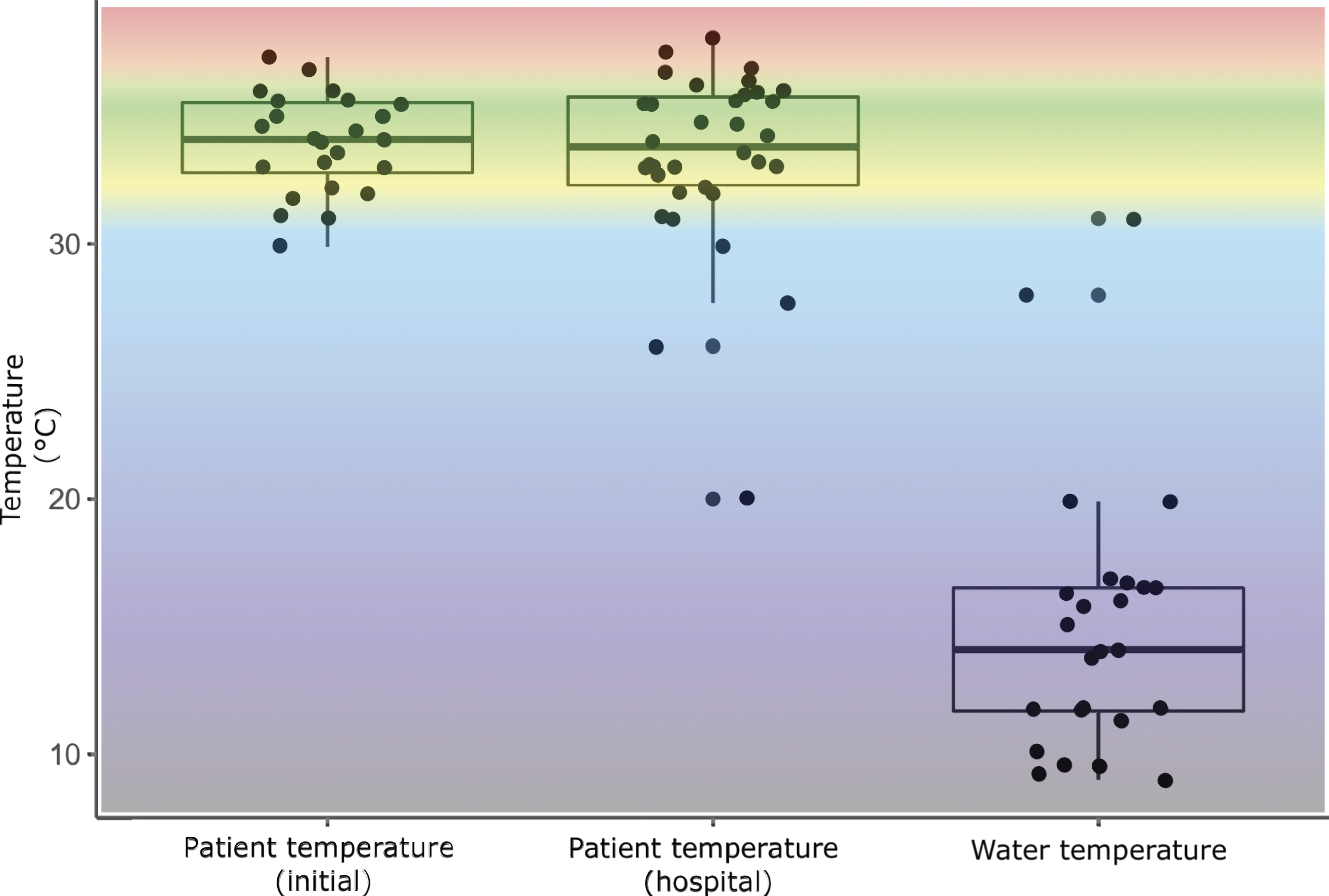
Saltwater drownings account for 25 cases (51%), with a further 10 (20%) occurring in swimming pools. The remaining cases occurred in freshwater in rivers, ponds or bath tubs. 22 cases occurred in still water, 12 in waves and six in flowing water.
Submersion duration was known for 30 out of 49 cases. As shown in Figure 2, median submersion duration was 2.5 min (IQR 1.0–9.3, range 1.0–30.0). The time between being seen underwater to first treatment was known for 28 cases, with a median of 12.0 min (IQR 9.0–20.0, range 2.0–78.0). Box and whisker with jittered points indicating spread of duration of submersion and submersion to treatment times. Submersion is recorded as the time the airway was seen underwater. Submersion ends when the victim is removed from the water (rescue). The difference between the two durations is due to the time taken between rescue and treatment by emergency medical services.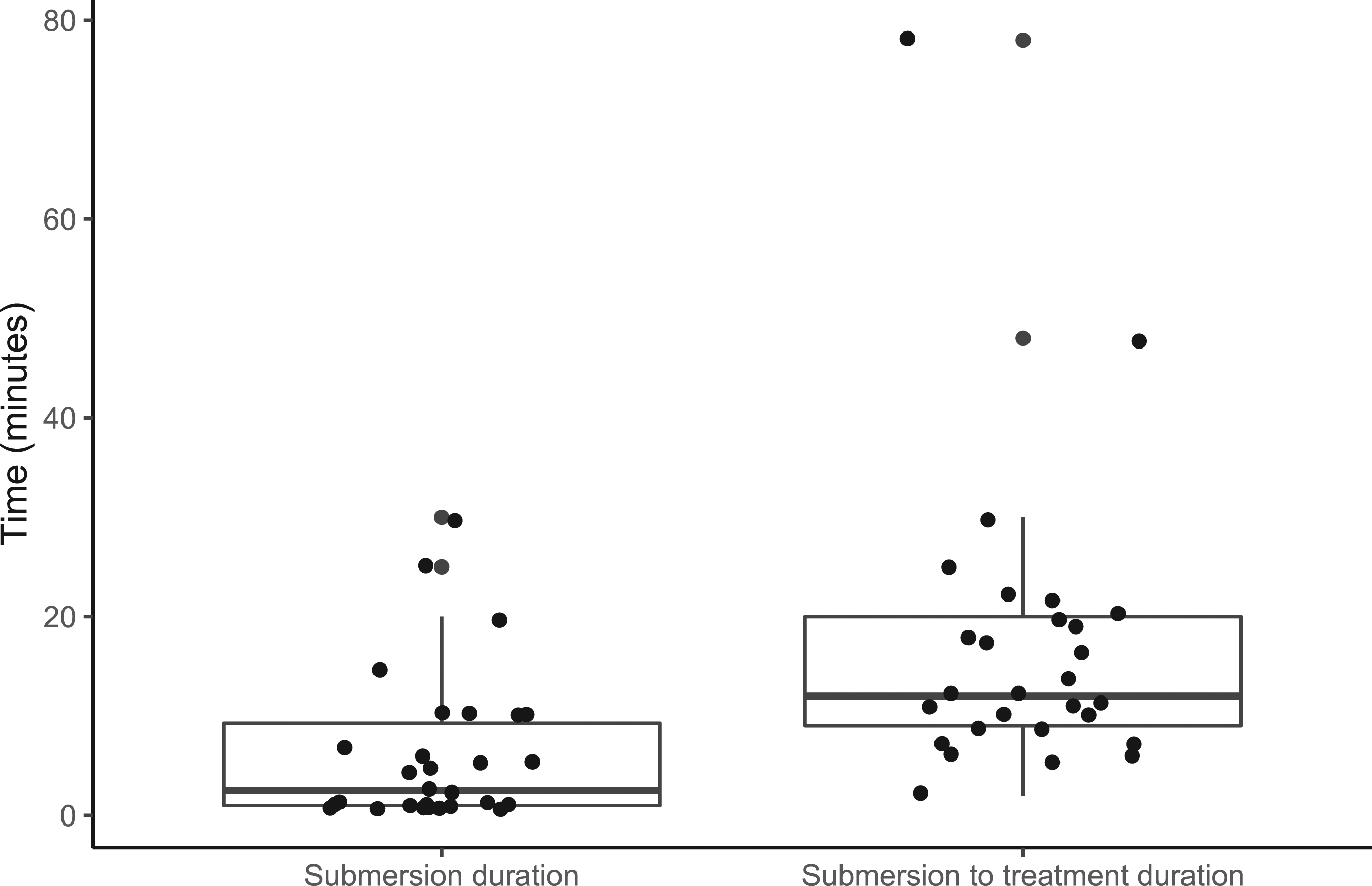
The most common identifiable precipitant was drug intoxication (20%). Seventy-one percent of patients did not have pre-existing illnesses. The most common pre-existing illness was a chronic neurological disorder (including seizure disorders). A lack of adult supervision was identified in three of seven paediatric cases.
Seventy-one percent of cases were directly witnessed, the majority by bystanders rather than lifeguards or emergency services. Most cases were removed from water by bystanders (60%), six were rescued by lifeguards (3 pool, 3 beach). Twenty cases received bystander CPR and a partially overlapping 20 cases were found to be in cardiac arrest by EMS. Seven patients who had not received bystander CPR were subsequently found to be in cardiac arrest by EMS and seven patients who had received bystander CPR were subsequently found to have cardiac output on EMS assessment. Of those in confirmed cardiac arrest the rhythm was non-shockable in all cases with 15 (75%) in asystole and 5 (25%) in pulseless electrical activity (PEA). CPR was ongoing on arrival to hospital in 10 cases (50%), the remaining 10 achieved pre-hospital return of spontaneous circulation (ROSC). The median duration of CPR was 10 min (IQR 2.0–26.0, range 1.0–210.0). Of those 20 patients in cardiac arrest for whom the most advanced airway management was documented, 13 were intubated, five had a supraglottic airway inserted and one was managed by mask ventilation alone. Overall, 16 patients (33%) were intubated in the pre-hospital phase, 13 of these were in cardiac arrest and three patients underwent pre-hospital emergency anaesthesia (PHEA).
Demographics, comorbidities and initial observations.
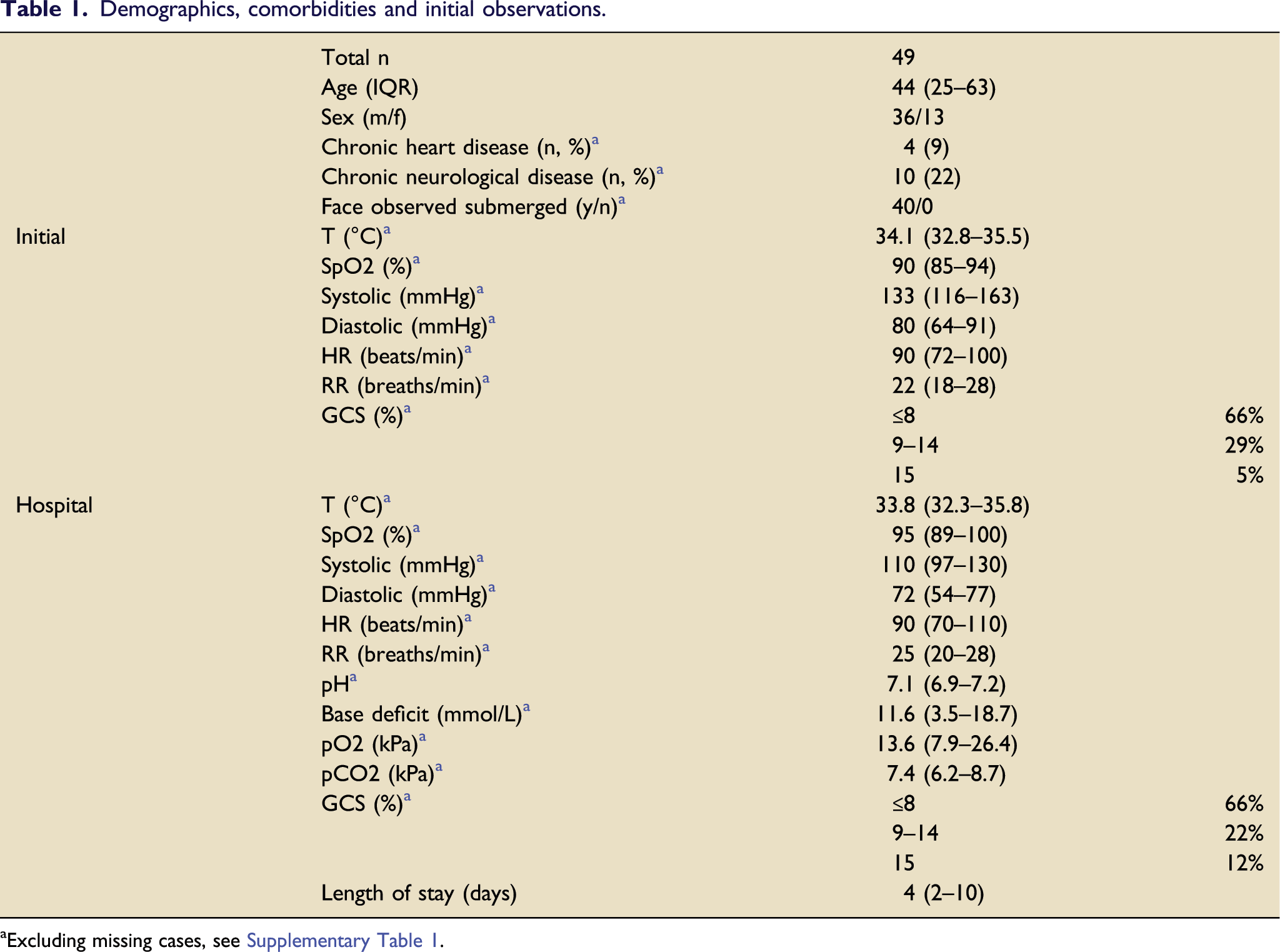
aExcluding missing cases, see Supplementary Table 1.
The average length of stay in hospital was 4 days (IQR 2–10, range 0–95). 12 (25%) patients underwent therapeutic hypothermia by targeted temperature management. At discharge 22 (45%) patients had preserved functional status, 10 (20%) patients had a reduced functional status relative to their premorbid status, either needing some or total support with activities of daily living (ADL). 17 (35%) patients died in hospital. Of those in confirmed cardiac arrest, 15 (75%) died and of the remaining 2 (10%) had preserved functional status and 3 (15%) needed total assistance with ADLs.
Table 1––Demographics, comorbidities and observations for patients having undergone a drowning event. Initial observations were taken from the pre-hospital phase of care, or upon attendance in the emergency department if the former were not available. Unless otherwise stated, central tendency and spread is measured using median and interquartile range. Full observations and data completeness are found in Supplementary Table 1.
Discussion
This retrospective study report on drowning victims in the UK presents a summary of drowning related critical care admissions in Southwest England over an 11-year study period. The summary statistics presented here are produced based on detailed patient level data recorded in line with Utstein standards and are the first such data from the UK. 7
Drowning related admissions to critical care units are relatively uncommon, with participating units in the SWARM trainee research network overall averaging fewer than one case per year. This cohort was generally less co-morbid than average for the UK, which could be a result of fitter people being more likely to undertake activities in and around water. We found submersion is generally brief, in keeping with previous data. 5 Our cohort presented hypoxic, hypercapnic with a profound mixed respiratory and metabolic acidosis. Despite this, our data show that the drowning process was amenable to intervention; 45% of admissions were discharged with a preserved functional status, and we report a 25% survival from out of hospital cardiac arrest (OHCA) despite all cases being in non-shockable rhythms. 15 Our data is in keeping with previous descriptions of short critical care and hospital stays. 11
This work is limited by its retrospective nature, meaning that some data was inconsistently recorded or missing (data completeness for each variable is shown in Supplementary Table 1). The drowning process itself brings limitations to some variables. Drowned victims are often wet and cold which can make pulse oximetry and infra-red thermometry unreliable.16,17 We found 30% patients had unrecordably low initial temperatures, which may explain the apparent drop in average temperature in hospital data as the previously unrecordable very low core temperatures could be measured. These cases may have benefited from pre-hospital thermometry methods which do not rely on detection of infra-red light.
It is important to note that this work only seeks to describe the small proportion of drowning patients admitted to critical care, not all-comers. Indeed, thanks to its broad definition we can be sure that not all drowning victims are seen by lifeguards or emergency services, let alone hospital clinicians. For this reason, we have taken a pragmatic approach to break down the larger problem of understanding drowning management and subsequent outcomes. This meant focusing on the highest acuity patients; those admitted to critical care. This paper provides the first such data from the UK and contributes to similar work from around the world.11,18–21
Known risk factors for drowning include alcohol usage, male sex and epilepsy.19,22–24 In our cohort, 82% of cases had at least one of these three risk factors. Further risk factors include low socioeconomic status, lack of supervision and rural residency.25–27 The impact of these risk factors on our data however is unclear due to the difficulty of obtaining such variables from retrospective data. There is conflicting data on the role of age as a risk factor in drowning. Globally the years up to 14 have been identified as a risk factor, however the UK mortality data does not bear this out.4,27 This data includes seven paediatric cases, of which the majority were transferred to a children’s hospital for further management. There is censoring of paediatric drowning cases in this cohort due to direct transfer to the children’s hospital bypassing local critical care services either from the scene or from the emergency department.
The presence of lifeguards, education campaigns (e.g. “float to live”), induced hypothermia and in rare circumstances very rapid cooling at time of submersion have been suggested as protective factors in drowning events.27,28 We collected data on lifeguard involvement, induced hypothermia, water temperature as well as EMS response times (Figure 2). Lifeguards rescued only 12% of this cohort. This may represent the vast challenge of covering more than 7,000 miles of coastline and innumerable inland waterways but could also be due to a protective effect of rapid lifeguard rescue in avoiding critical care admission. 29 Education is difficult to assess in this context as discussed above, with anecdotal reports suggesting the advice to float on unexpected immersion may avoid commencement of the drowning process. 28 Coastal waters in the UK are very rarely in the icy range (<6°C) where neuroprotective effects can occur however inland waterways may be in this range during much of the winter, especially on high ground and following recent rain or snow fall.30,31 None of the cases in this cohort occurred in icy bodies of water.
There is significant morbidity following drowning in this cohort. 31% of patients who survived to discharge went on to require an increased level of assistance with their activities of daily living. Independence is an important outcome to patients and loss of independence is associated with poorer reported quality of life.4,32 This is a new finding and sheds light on an important and under investigated topic.
The quality of evidence on which gold standard management of drowning victims is currently based is suboptimal due to the challenges of studying this population. Large meta-analyses of retrospective data are of value in the absence of randomised trials. 33 Previous meta-analyses of retrospective data have been hampered by poor quality data.5,6 By collecting data in accordance with the Utstein standards, we hope to contribute to a better understanding of the morbidity of drowning
Conclusion
This paper is the first such data from the UK and contributes to similar work from around the world. Admission to critical care following drowning is associated with high rates of mortality and poor functional outcomes. By recording a functional outcome at patient discharge, we find that 31% of those who survived a drowning event subsequently required an increased level of assistance with their activities of daily living. Looking forward there is a need for more standardised data sets to allow causal studies to detect signals in treatment differences.
Footnotes
Acknowledgements
The authors would like to thank participating NHS Trusts for their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analysed during this study are included in this published article and its supplementary information files.
Ethical approval
This study seeks to define current care for drowning patients in critical care. There are no interventions, no patient identifiable data is presented and the results are not intended to be generalisable or transferable. As such this study did not require specific ethical approval as it falls under the scope of clinical audit and service evaluation.