
Abstract
Background:
Socioeconomic inequalities in chronic disease management and outcomes are well-established. Their association with critical illness management and outcomes is less clear. This study aimed to investigate the association between socioeconomic status and outcomes following emergency admission for critical illness.
Methods:
Three Scotland-wide health databases were linked: the Scottish Intensive Care Society Audit Group database (critical care units); the Scottish Morbidity Record 01 (hospital admissions) and death certificates. A retrospective cohort study was conducted on adults (⩾16 years) admitted as an emergency to critical care units between 25th October 2010 and 25th October 2021 inclusive. Cox proportional hazards models were used to investigate the association between area-based socioeconomic status (Scottish Index of Mortality (SIMD) decile) and all-cause mortality, adjusting for potential confounders: age, sex, comorbidities, illness severity, and diagnostic group. Secondary outcomes included unit and hospital lengths of stay, and emergency hospital readmissions.
Results:
Overall, 50,914 patients were included in the cohort. Those in the least deprived decile were less likely to die (adjHR 0.85, 95% CI 0.79–0.92), had 19% longer critical care unit stays (95% CI 13–26) and a 12% longer hospital stays (95% CI 7%–18%). Over the subsequent year, the least deprived had significantly fewer emergency hospital re-admissions (adjIRR 0.73; 95% CI 0.67–0.81).
Discussion:
People living in the most deprived communities have worse outcomes following emergency admission to critical care; particularly in the longer term and reinforcing the need to address socioeconomic inequalities in healthcare access and outcomes.
Introduction
The social determinants of health have emerged as an important public health priority, with a growing understanding of the link between social conditions and health-related outcomes. 1 However, while a significant body of research has addressed the impact of socioeconomic status on chronic illness, 2 the influence of social factors on outcomes following critical illness is less well understood and recent reviews of the association between socioeconomic status and outcomes in critical care have highlighted mixed results from previous studies.3,4
In emergency care, social deprivation is associated with greater likelihood of presentation across a range of acuity, 5 and there is some evidence that patients from more deprived areas are more likely to die following emergency presentation. 6 However, as most studies of the effect of socioeconomic status on outcomes following critical illness have considered all admissions to critical care, 3 or assessed admissions by surgical status, 7 it is less clear how social deprivation impacts outcomes following emergency presentation. Specific consideration of emergency presentations is important because appropriate critical care interventions at each stage of the patient journey, from the pre-hospital phase to in-hospital care, have the potential to improve outcomes.8,9 However, it is not currently known to what extent socioeconomic deprivation is associated with healthcare use and outcomes following emergency critical illness.
As healthcare systems strive to mitigate inequalities in health, 1 understanding the impact of socioeconomic status across a range of clinical acuity is important, to plan services which are currently often distributed inversely to projected need10 –12 and to allow the consideration of strategies that might prevent poor outcomes in vulnerable groups. 13 This study aims to assess the association between socioeconomic status and mortality following emergency admission for critical illness, as well as healthcare use in terms of critical care length of stay and hospital readmissions.
Methods
Dataset linkage and analysis were performed within a trusted research environment provided by Public Health Scotland with approval, including ethical review, from the Public Benefit and Privacy Panel for Health and Social Care (2223-0006).
Data from the Scottish Intensive Care Society Audit Group (SICSAG) database, covering all adult critical care unit and high dependency unit (HDU) activity across Scotland, were linked to the Scottish Morbidity Record 01 (SMR01) and National Records of Scotland databases, covering acute hospital admissions and death records respectively.
The study cohort included all emergency hospital admissions that included a critical care unit stay for adults aged ⩾16 years, between 25th October 2010 and 25th October 2021 inclusive. Emergency admission status was determined by SMR01 records and excluded those admitted to critical care following elective surgery or as part of a planned admission. To take account of differences in terminology between hospitals, we included Intensive Care Unit (ICU) or High Dependency Unit (HDU) admissions during which patients received critical care; defined as those receiving mechanical ventilation or multiple vasopressors. Where patients experienced multiple emergency admissions across the study period, only the first was included as an index event. Data were censored at the end of the study period, or at patient death, whichever was sooner.
The primary outcome of interest was 1-year all-cause mortality following hospital admission. Secondary outcomes included critical care unit and hospital lengths of stay and, for those surviving to hospital discharge, the number of emergency readmissions to hospital in the following year.
The primary exposure was area-based socioeconomic deprivation obtained from postcode of residence and measured using the Scottish Index of Multiple Deprivation (SIMD). The SIMD uses 37 indicators across seven domains (income, employment, education, health, access to services, crime and housing) to rank 6976 small areas (population 700–800) across Scotland. The ranking is used to derive deciles, from 1 (most deprived 10%) to 10 (least deprived 10%). 14
Potential confounders, included as covariates in the models, included: demographic factors (age on admission and sex), number of comorbidities (defined by comorbidities of the Charlson Comorbidity Index), 15 main diagnosis necessitating critical care admission (using APACHE (Acute Physiology and Chronic Health Evaluation) II diagnostic categories in established groupings 16 ), and a measure of disease severity, the Acute Physiology Score (APS) of the APACHE II model. 17
Statistical analyses
Population demographics and clinical characteristics were summarised using the median and interquartile range (IQR) for continuous variables, and numbers with percentage for categorical variables. As the impact of socioeconomic status on outcomes from Scottish ICUs during the COVID-19 pandemic has previously been reported, 11 additional sensitivity analyses were undertaken excluding all admissions after 31st December 2019.
The APACHE II score, and therefore the APS variable, is not a mandatory field in the SICSAG dataset and missing data has been encountered in previous studies. 11 Missing data for the APS variable was handled with multiple imputation, with the number of imputations calculated using the methods of von Hippel. 18
Cox proportional hazards models were used to investigate the association between socioeconomic status and mortality up to 365-days following hospital admission, reported as hazard ratio (HR) with 95% confidence interval (95% CI) and visualised with adjusted Kaplan-Meier plots stratified by socioeconomic deprivation. Proportionality assumptions were assessed visually.
Critical care unit length of stay, available as fractions of days, was modelled using log normal regression with robust standard errors, and both hospital length of stay and emergency readmissions in the year following discharge, available as count data, was modelled using negative binomial regression. 19 Coefficients of log normal and negative binomial regression were exponentiated for interpretation as percentage change and incidence rate ratios (IRR) respectively, and presented as forest plots. 20
The models were run univariately then as multivariable models including the covariates listed above. Data were analysed using R (R Foundation for Statistical Computing, Vienna, Austria), using the adjustedCurves and MASS packages.21,22
Results were reported in accordance with the STROBE guidelines (Table S13). 23
Results
Of the 51,663 emergency admissions over the 11-year period, 749 (1.4%) were excluded due to missing SIMD data, leaving 50,914 (98.6%) admissions for inclusion in the analyses (Supplemental Figure S1).
Patient demographics and baseline clinical characteristics are presented, stratified by SIMD decile in Table 1. The number of admissions to critical care varied inversely with increasing socioeconomic status, ranging from 8055 (15.8%) admissions from the most deprived decile, to 2951 (5.8%) in the least deprived. Median age at admission also differed by socioeconomic status, from 54 (IQR 41–67) years for the most deprived to 66 (54–75) years for the least deprived decile. Across the socioeconomic spectrum, men represented a greater proportion of admissions (58.3%). Most patients had at least one comorbidity (61.0%), and the most deprived decile was more likely to experience four of more comorbidities on admission; 5.5% compared to 1.7% of the least deprived decile. Median APACHE II APS, a measure of acute illness severity, was relatively stable across the cohort. More affluent patients were admitted more often with cardiovascular diagnoses including septic shock (38.9% of least deprived decile vs 12.2% of most deprived decile), while the most deprived patients were admitted more often with respiratory diseases (18.0% of least deprived vs 24.0% of most deprived) or self-poisoning (4.1% of least deprived vs 11.0% of most deprived).
Baseline characteristics of emergency admissions to critical care in Scotland 2010–2021.
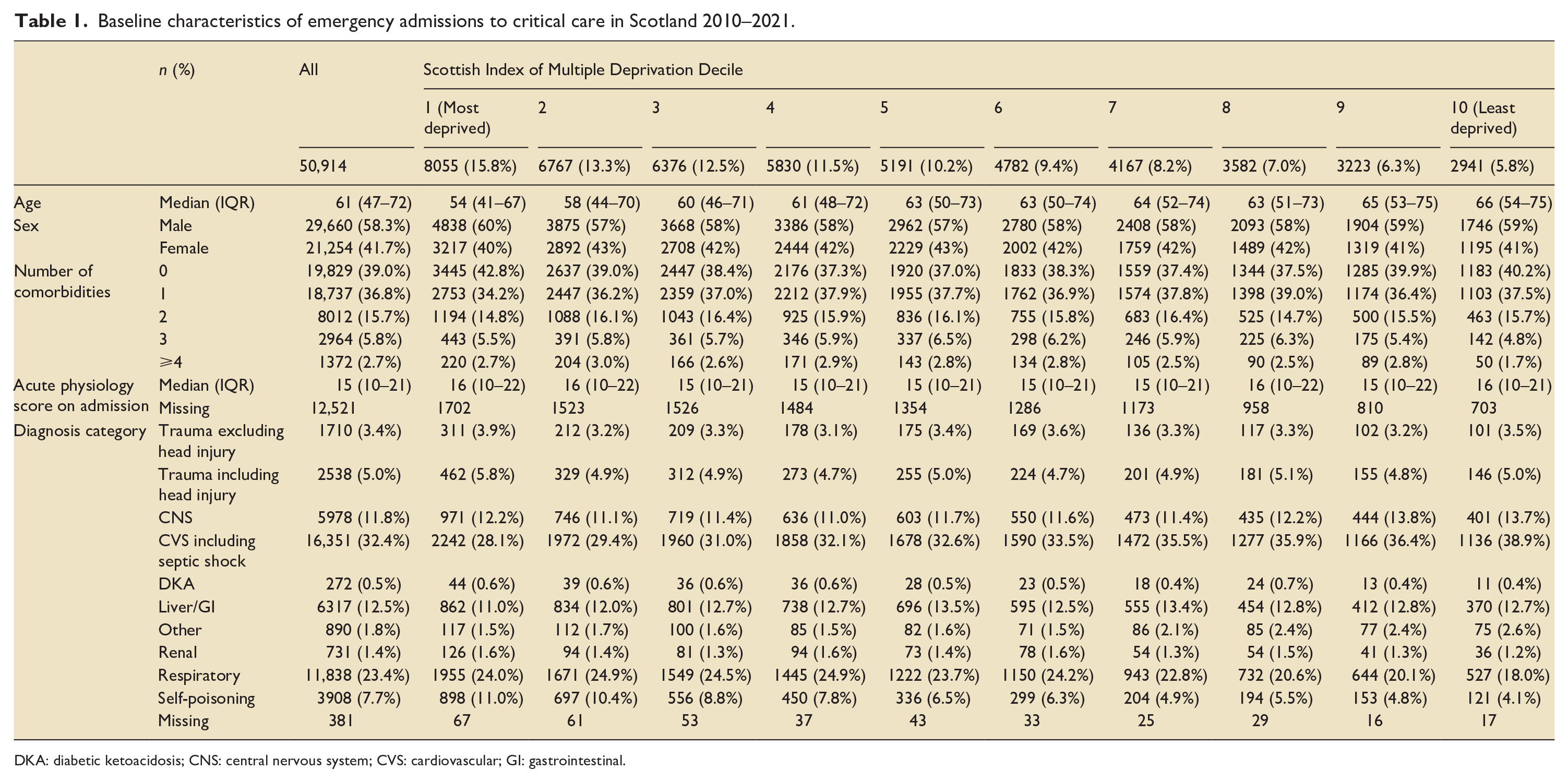
DKA: diabetic ketoacidosis; CNS: central nervous system; CVS: cardiovascular; GI: gastrointestinal.
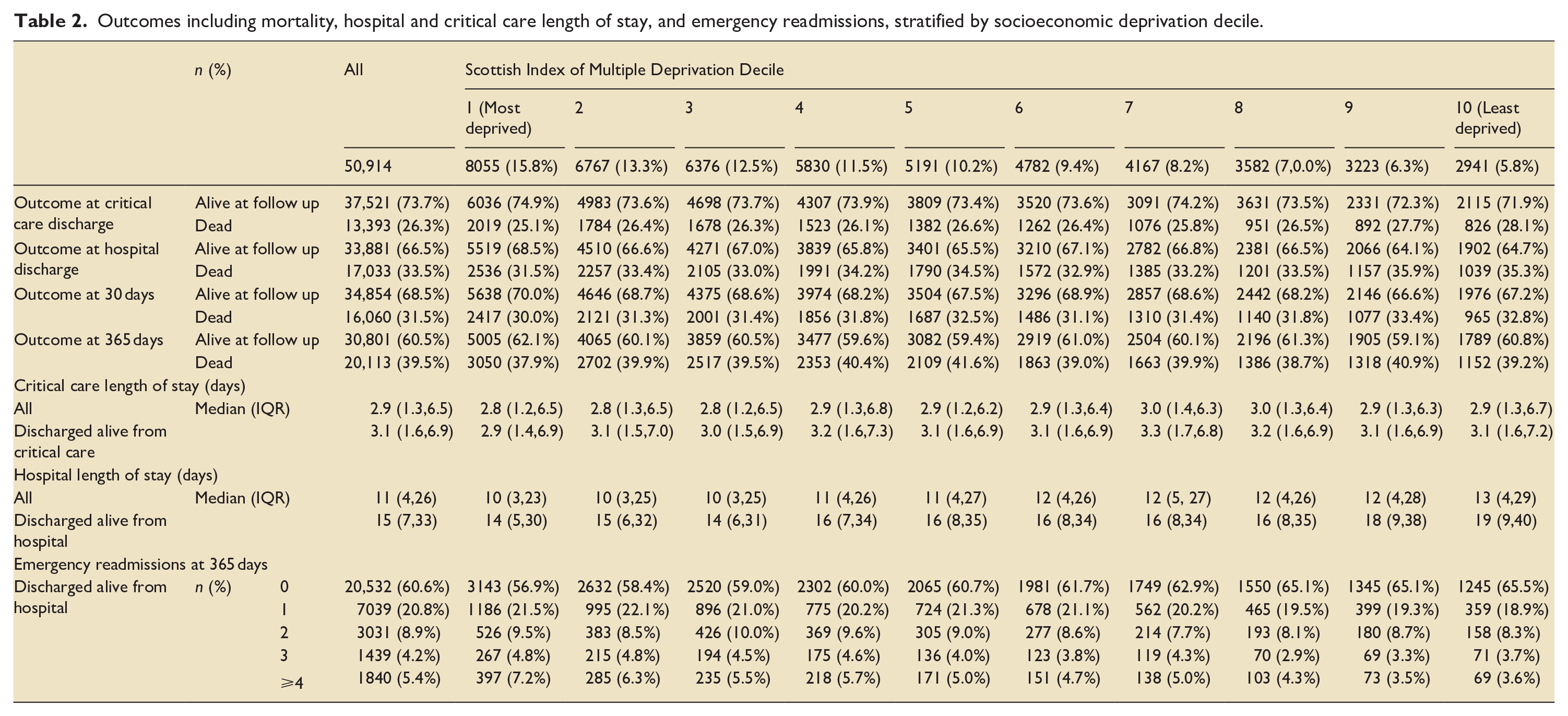
The median follow-up included for survival analysis was 365 days (IQR 3–365 days). The majority of patients, 30,801 (60.5%), were alive at follow up. Median critical care length of stay was 2.9 days, and similar across SIMD deciles. Median hospital length of stay was 11 days for the whole cohort and increased with increasing affluence, from 10 days in the most deprived decile to 13 days in the least deprived. Emergency readmissions to hospital reduced with increasing socioeconomic status, with 397 (7.2%) of the most deprived having ⩾4 emergency readmissions during the year after discharge, compared to 69 (3.6%) of the least deprived. Outcome data for mortality at endpoints up to 1 year, length of stay, and emergency readmissions, are seen in Table 2.
Outcomes including mortality, hospital and critical care length of stay, and emergency readmissions, stratified by socioeconomic deprivation decile.
No significant difference was seen on univariate analysis of the association between socioeconomic status and probability of 1-year survival, for the least deprived compared to the most deprived decile HR 1.05 (95% CI 0.98–1.12). However, at other deciles of SIMD significant differences were found, with a greater likelihood of death in areas of greater affluence; for example, for the second-least deprived decile, SIMD 9, HR 1.11 (95% CIs 1.04–1.18). In multivariable analysis, these findings were reversed, with significantly reduced risk of mortality for patients from more affluent areas; for the least deprived compared to the most deprived decile adjusted HR 0.85 (95% CIs 0.79–0.91). Results of Cox proportional hazards survival modelling is seen in Table 3 and adjusted Kaplan-Meier survival curves for the primary outcome are demonstrated in Figure 1. Full model outputs are available in Online Supporting Information Tables S1–S6.
Cox proportional hazards modelling for the association between socioeconomic status and mortality up to 1 year.
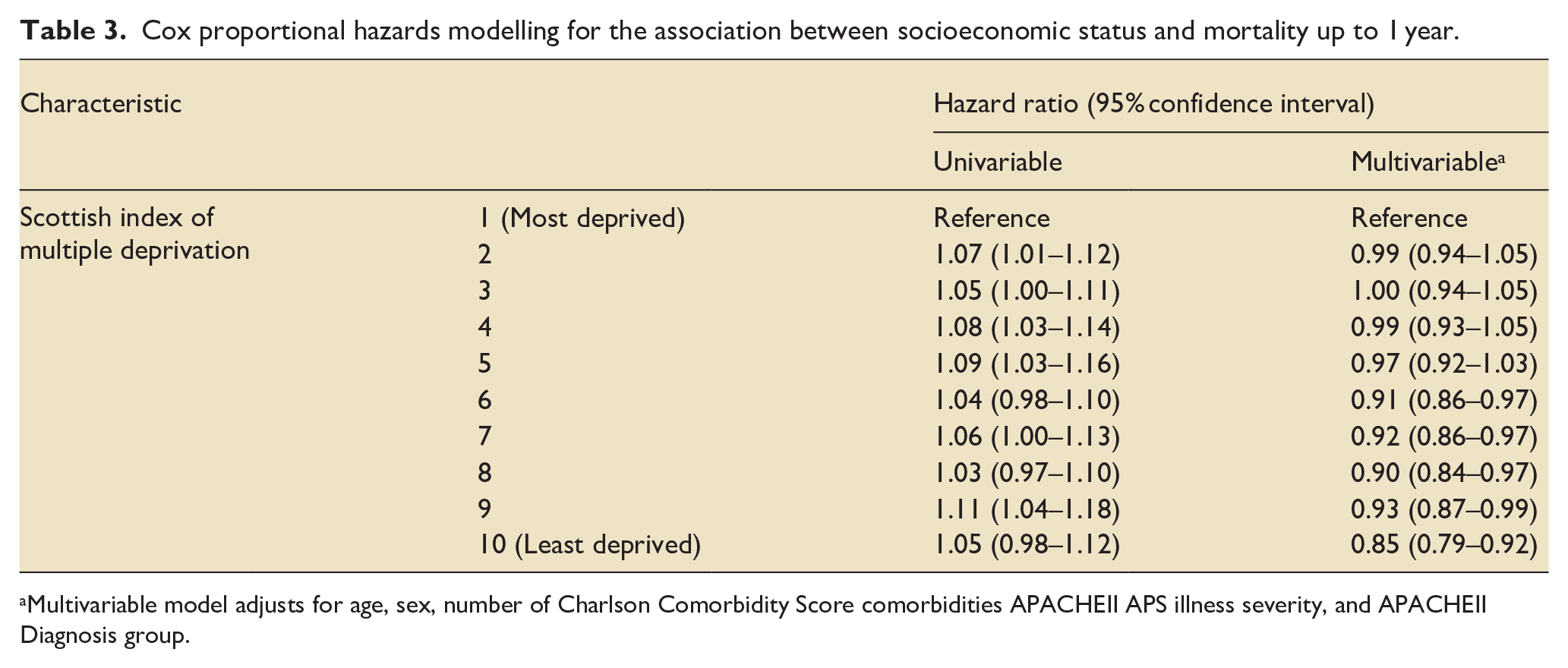
Multivariable model adjusts for age, sex, number of Charlson Comorbidity Score comorbidities APACHEII APS illness severity, and APACHEII Diagnosis group.
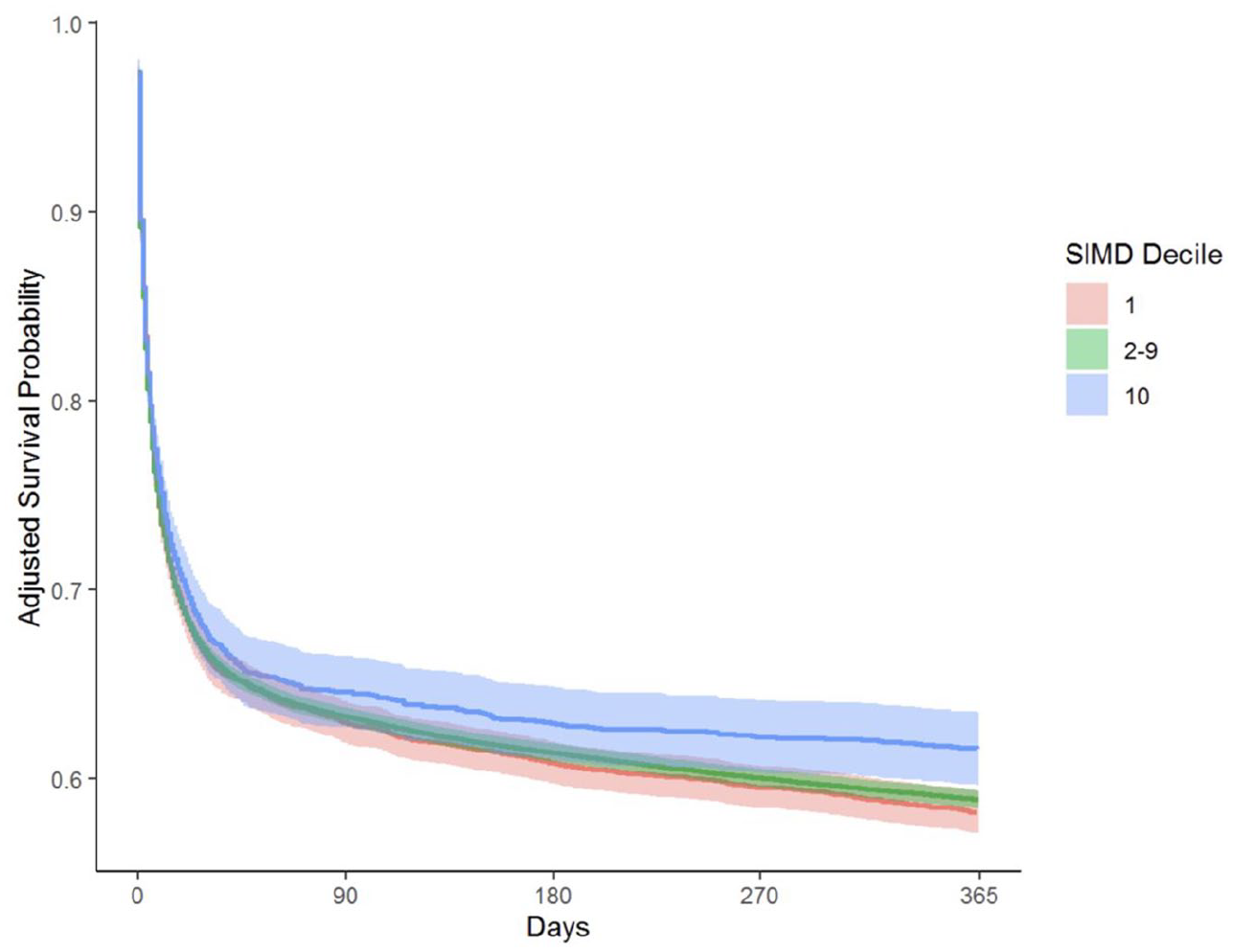
Adjusted Kaplan-Meier survival curve for mortality in 365 days following hospital admission with critical illness, stratified by socioeconomic status as Scottish Index of Multiple Deprivation. *SIMD – Scottish Index of Multiple Deprivation. Multivariable model adjusts for age, sex, number of Charlson Comorbidity Score comorbidities APACHEII, and APS illness severity APACHEII Diagnosis group.
There were significant differences in length of stay across the cohort; in the multivariable model, those in the least deprived decile were estimated to have a 19% longer critical care unit stay (95% CI 13–26) than the most deprived, and a 12% longer hospital stay (95% CI 7–18). Similar findings were seen in subgroups of patients surviving to discharge from both critical care and hospital. In multivariable models, those in the least deprived decile had a lower rate of emergency hospital readmission in the year following discharge, IRR 0.73 (95% CI 0.67–0.81). Forest plots for the multivariable models for length of stay and emergency readmission are seen in Figure 2, with univariable and multivariable model outputs in Table 4. Full model outputs are available in the Supplemental Appendix.
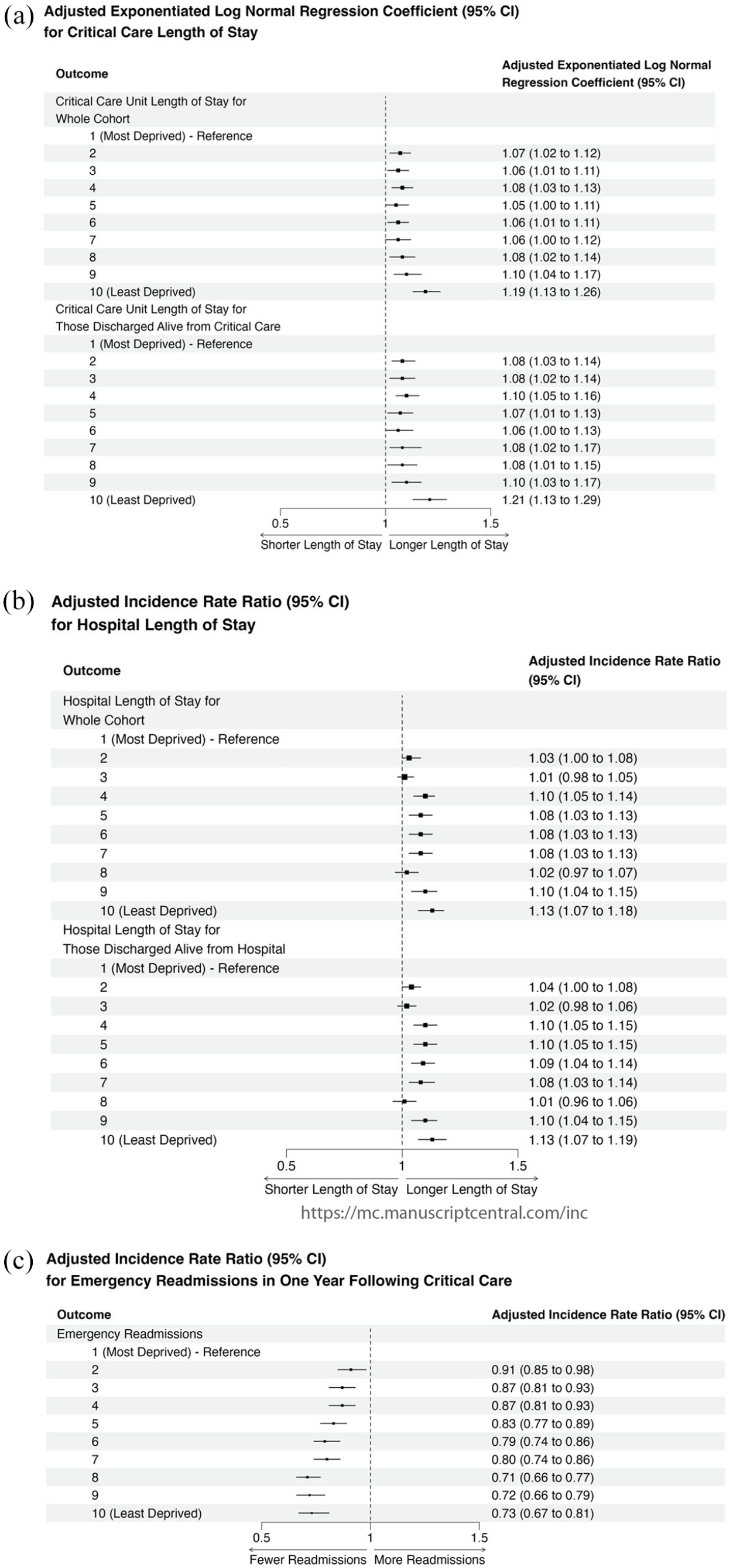
Forest plots for the association between socioeconomic status by the Scottish Index of Multiple Deprivation and critical care length of stay (a), hospital length of stay (b), and emergency readmissions (c). Multivariable models adjust for age, sex, number of Charlson Comorbidity Score comorbidities APACHEII, and APS illness severity APACHEII Diagnosis group.
Results of regression modelling for critical care and hospital length of stay, and emergency readmissions in the 1 year following emergency admission to critical care.
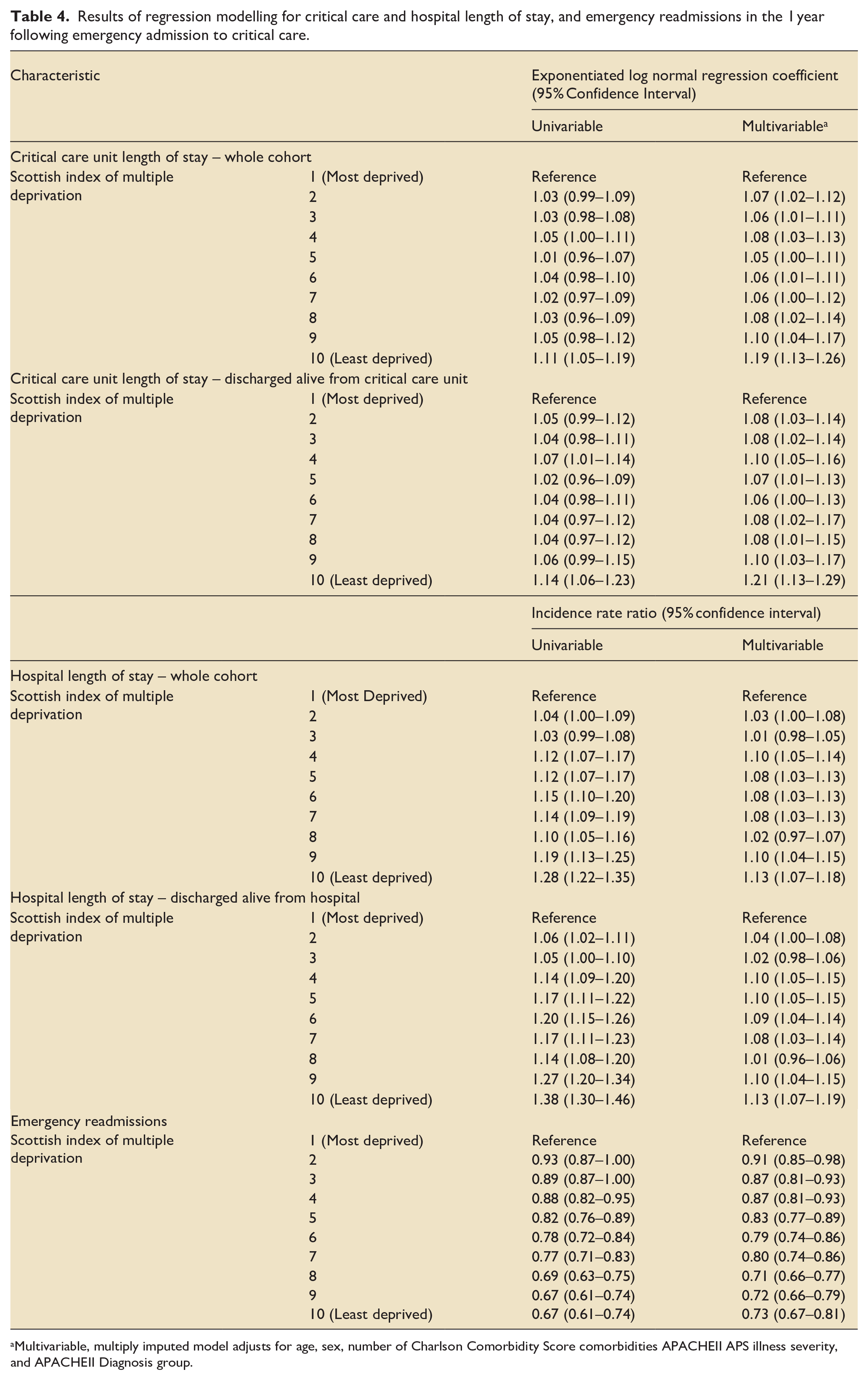
Multivariable, multiply imputed model adjusts for age, sex, number of Charlson Comorbidity Score comorbidities APACHEII APS illness severity, and APACHEII Diagnosis group.
Sensitivity analyses for the period prior to the COVID-19 pandemic, excluding patients admitted to hospital after 31st December 2019, demonstrated consistent results to the main analysis (Supplemental Tables S7–S12).
Discussion
The results provide evidence that those living in the most deprived areas have the highest demand for critical care, the shortest duration of care in critical care units, and the worst outcomes. People living in the most deprived areas are both more likely to require readmission following discharge from critical care units and more likely to die. The Inverse Care Law describes the tendency of healthcare provision to vary inversely with population need. 10 While these results demonstrate that critical care admissions are markedly higher for the most socioeconomically deprived patients, suggesting the potential of critical care to mitigate some of the harms associated with health inequalities, their outcomes remain poorer than less deprived patients, indicating that a gap remains between the provision of care and expected outcomes. These findings may be framed in the differentiation between inequalities, which involves the identification of differences in healthcare provision between groups, and of inequity, which describes how those differences reflect the underlying level of need in different populations. 24
This study assesses outcomes up to 1 year following critical care admission, and the increased risk of emergency readmission for the most deprived indicates the potential for unmet need in supporting recovery from critical illness in this group. Significant differences in mortality are present between the most deprived groups and those in each of the SIMD deciles 6–10, however, the greatest effect sizes are seen at the extremes, indicating a dose-dependent relationship between area-level socioeconomic deprivation and mortality following critical illness.
There are several possible mechanisms for these findings. It is plausible that those from more affluent areas recognise the signs of critical illness earlier, and present at a time of greater therapeutic potential. More deprived areas are known to have less access to critical care resources,11,12 and excess mortality in these groups may reflect restricted access to effective critical care interventions. Unmeasured confounders may also have a role; for example, only the number of chronic conditions experienced by each patient was accounted for in modelled, which does not reflect the specific diagnosis or nature of these chronic diseases, or that APS does not fully account for acute disease severity. While these results are adjusted for severe comorbidities, they do not adjust for less-severe multimorbidity that is known to be more prevalent in patients experiencing social deprivation, 25 and may increase the risk of death in emergency critical illness. Those from the most deprived areas are admitted to critical care at a younger age, indicating systematic differences in the population at-risk and mirrors population-level findings of reduced life expectancy for the most deprived patients. 2 Differences in mortality may reflect differences in therapeutic intensity across the socioeconomic spectrum. Whilst limited previous work has suggested there is no existing evidence for differences in critical care unit treatments by race 26 or socioeconomic status, 27 our finding of shorter duration of stay in critical care units for more deprived groups merits further research. It is plausible that patient or family preferences, or clinician decision-making, varies with socioeconomic status. For example, racial and ethnic characteristics have been shown be associated with end-of-life care decisions in critical care, 28 and implicit bias has been demonstrated in healthcare providers, especially in high cognitive load scenarios such as those seen in critical care. 29
The most deprived groups had shorter length of stay, but higher mortality, even for those patients discharged alive. While shorter length of stay may indicate a more efficient care for these groups, higher mortality suggests that effectiveness may be poorer. However, this cannot be assessed rigorously in the absence of sufficiently granular data on case-mix. It is also possible that ICUs and hospitals in more deprived communities discharge patients earlier in response to known higher demand for their services. 11
Visual inspection of the adjusted Kaplan-Meier plot of survival to 1 year indicates clearer separation of groups later in the follow-up period. This finding, together with evidence of greater number of emergency hospital readmissions for more deprived groups, may indicate that it is not inpatient care for the index episode that creates the differences seen between groups, but differences in the recovery from critical illness that contributes to the increased mortality for more deprived groups.
These data demonstrate both greater requirements for, and poorer outcomes following, emergency care among the most deprived, and reflects recent systematic reviews and the only available meta-analysis of general critical care cohorts.3,4 No other report is known to have assessed outcomes from emergency admissions to critical care across a spectrum of socioeconomic status, and given the understanding of the importance of robust and functional links between the different phases of care in critical illness, 9 these findings have importance across the spectrum of emergency care, from the pre-hospital environment, to Emergency Departments and critical care units. Deprived communities are already known to have less likelihood of receiving early effective interventions in critical illness, such as bystander cardiopulmonary resuscitation in cardiac arrest, 13 and poorer access to critical care.11,12 These findings reflect known inequalities in emergency healthcare and demonstrate that these inequalities are associated with poorer outcomes. Mitigating the unequal outcomes is likely to require a whole-system approach; from effective public health interventions to reduce the risk, and improve recognition, of emergency illness, to improved ambulance service pre-hospital response and Emergency Department care, 30 as well as a recognition that socioeconomic status is associated with outcomes within the ICU.
This work benefits from a large sample size when compared to many studies in the field,3,4 improving the precision of effect estimates. Linkage across national-level datasets provide complete coverage of the Scottish population during the investigated timeframe, and includes national mortality records. Similar APACHEII Acute Physiology Scores were seen across the range of socioeconomic status, implying little difference in the threshold for admission, but differences in outcomes remain, and it is notable that patients admitted to critical care from more deprived areas were younger than their more affluent counterparts, in keeping with the well-documented effects of social deprivation on life expectancy. 1
This study has limitations. Despite the use of national records, which record all deaths, it is not possible to account for the deaths of patients who might emigrate outside of Scotland following discharge. A small number of patients without a Scottish address, or of no fixed abode, were excluded, as it is not possible to assign SIMD deciles to these patients. Concerns regarding the potential circularity or endogeneity of SIMD, a socioeconomic index which includes health outcomes, as a metric to assess the health outcomes across a population have been explored, with reassuring findings when compared to indices only assessing income and employment.31,32 While confounders known to contribute to mortality in critical illness and available to us were included in the multivariable modelling, the possibility of residual confounding is a limitation of all observational studies, and particularly those where models include relatively heterogenous diagnostic groups. 33 The APACHE II clinical severity score from which APS is derived is a mandatory field in ICU, but not HDU, admissions in Scotland. As such, missing variables will not occur completely at random and despite multiple imputation techniques accounting for other features of admission, may introduce bias, albeit with lower risk than complete case analysis. 34 While the number of imputations is calibrated to the proportion of missing data, higher proportions of missing data result in less certainty around imputed values.18,35 Concistent with literature in the field, 3 no adjustment was made for multiplicity of analyses. While this brings a recognised risk of increasing probability of Type I error in random data, in circumstances where data are derived from observations, this approach is likely justifiable and reduces risk of type II error. 36
This study is restricted to patients admitted to critical care, and as such, does not include those suffering critical illness where it was felt that the potential benefits of critical care interventions did not outweigh the burdens, and so were not admitted to critical care. However, these findings suggest that despite a greater number of admissions for more deprived groups, mortality remains higher than in the more affluent, suggesting that the true burden of critical illness in the most deprived might be even higher than these inequalities suggest.
Healthcare policy must recognise and seek to mitigate structural inequalities that are known to exist in the distribution of resources,10,11 and this study reaffirms the greater need for critical care services in more deprived communities. Future research should assess the mechanisms for the poorer outcomes seen, and strategies for improving survival following critical illness in more deprived groups. It is notable that successful critical care follow-up programmes already integrate social support. 37 We found that the most deprived had a greater number of emergency readmissions following critical illness so, as these programmes develop, the impact of social determinants on the return to healthy lives should remain a key consideration in post-critical care support.
Supplemental Material
sj-docx-1-inc-10.1177_17511437251338608 – Supplemental material for The association between socioeconomic status and outcomes in critical illness: A national cohort study of emergency admissions to critical care units in Scotland 2010–2021
Supplemental material, sj-docx-1-inc-10.1177_17511437251338608 for The association between socioeconomic status and outcomes in critical illness: A national cohort study of emergency admissions to critical care units in Scotland 2010–2021 by Ryan D McHenry, Christopher EJ Moultrie, Alasdair R Corfield, Nazir I Lone, Daniel F Mackay and Jill P Pell in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by clinical research funding from ScotSTAR, Scottish Ambulance Service.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.