
Abstract
Intensivists are increasingly involved in the care of frail patients as our population ages. Careful person-orientated, individualised decision-making, weighing benefits and harms of critical care are required in such situations. Few studies have reported outcomes of patients with treatment limitations. This dual-centre observational study reports outcomes of 3781 patients (2018-20). At least one treatment limitation was set at admission in 13% (n = 486). Of this group 55% survived to hospital discharge, of whom 69% were discharged home; 39% remained alive at 1 year. These findings provide objective data to support clinicians, patients and relatives in shared decision-making. Future multi-centre work could explore how best to identify those most likely to benefit from critical care
Introduction
Advances in critical care have enabled support of patients with profound illness severity. In parallel, projections suggest sustained increases in our older population, 1 with accompanying increases in those living with frailty and co-morbidities. The goal of critical care is not to avoid death at any cost, but to return a person to a quality of life that they would find acceptable. 2
There is some evidence to suggest older people may have the most to gain from escalation to critical care.3,4 However, failure to make appropriate treatment decisions may protract the dying process, be undignified and run contrary to the core ethical principals of non-maleficence. For relatives this may complicate grief and for staff cause moral distress and burnout.5,6 Clinicians are therefore necessarily wary of disproportionate treatments administered to those at highest risk of death.
Patients infrequently have advanced directives and often lack capacity. This leaves intensivists in a challenging position, navigating patients and their loved ones through complex decisions. 2 Objective outcome data may help such discussions, however few studies have focused on outcomes from patients who had treatment limitations placed at critical care admission.7,8 This study aimed to quantify the proportion of admissions who had treatment limitations placed and report 1-year outcomes.
Methods
Retrospective dual-centre observational study including all admissions to two non-specialist critical care units in Sussex, UK (2018-20). Treatment limitations (within first 24 hours of admission) included not for escalation to: invasive positive pressure ventilation (IPPV), non-invasive ventilation (NIV), kidney replacement therapy (KRT) or vasopressor support. Median (interquartile range, IQR) were reported. Comparisons were assessed using Mann-Whitney U and Mantel-Haenszel chi-squared tests.
Results
Of 3781 total critical care admissions, median age was 67 (IQR 52–77), 32% received IPPV, 14% NIV and 7% KRT. Frailty was measured by the clinical frailty scale, (CFS) 9 with a median overall score of 3 (IQR 2–5). At least one treatment limitation was present on admission to critical care in 13% (n = 486).
Comparison of age, frailty, organ support received and mortality (critical care, in hospital, 90 days and 1 year) of patients with treatment limitations and those for full escalation.
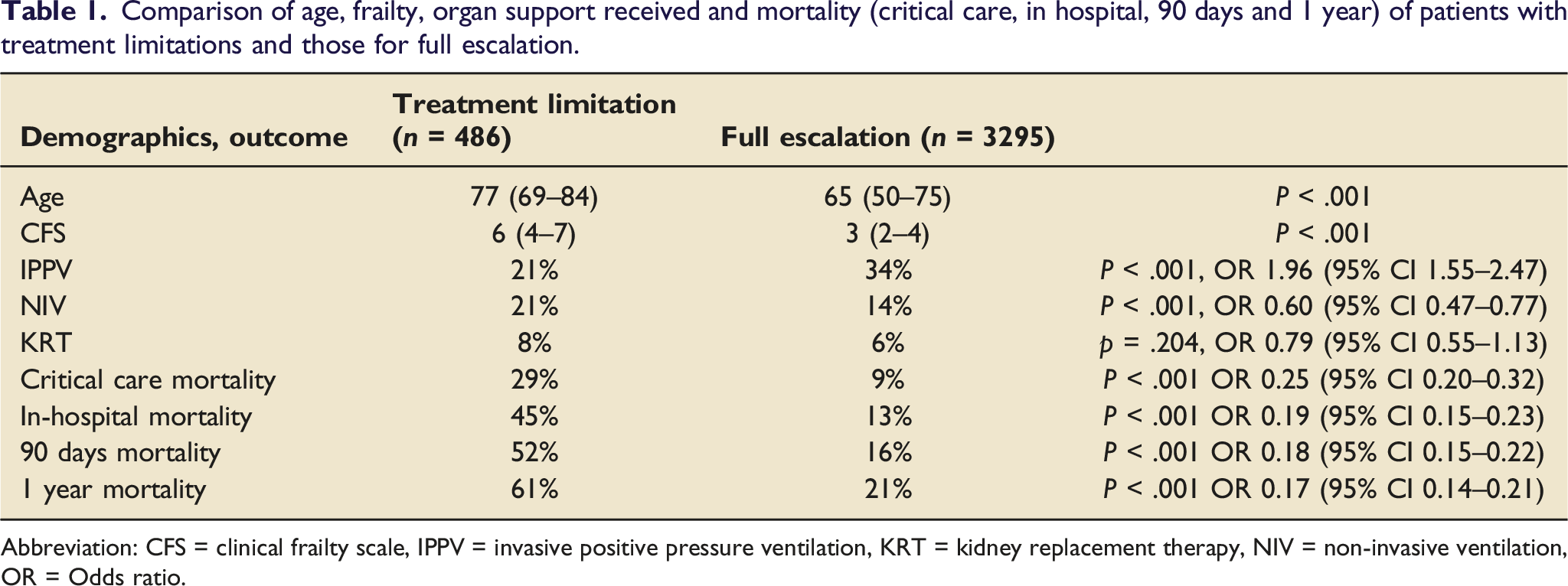
Abbreviation: CFS = clinical frailty scale, IPPV = invasive positive pressure ventilation, KRT = kidney replacement therapy, NIV = non-invasive ventilation, OR = Odds ratio.
Patients for full escalation were more likely to receive IPPV (34% vs 21%, p < .001, OR 1.96 (1.55–2.47)), received less non-invasive ventilation (14% vs 21%, p < .001, OR 0.60 (0.47–0.77)), and similar KRT delivery (6% vs 8%, p = .204, OR 0.79 (0.55–1.13)). Mortality at all time points was higher in those with treatment escalation limitations, of whom 39% were alive at 1-year.
Discussion
This dual-centre critical care observational study found that a significant proportion of patients have treatment limitations in place. Although mortality was higher than those without treatment limitations, more than half (55%) did survive to hospital discharge and 39% were alive at 1 year. This adds to the literature, reporting contemporaneous longer-term outcomes, with few such studies reported.7,8
Deciding if a frail, co-morbid person will benefit from critical care is an increasingly common scenario. Despite this, there is variability in decision-making between and within countries, and even individual intensivists within the same unit. 10 In this ‘grey zone’ of decision-making, admitting a patient to critical care with treatment limitations suggests a position where the responsible intensivist has acknowledged the fragility of the patient with a probable high risk of death, but consider the presentation to be potentially a treatable one.
More patients in this study with treatment limitations received NIV, reflecting a ceiling of care of respiratory support. The lack of difference in KRT between two groups is of interest. We postulate that co-morbid patients with treatment limitations may have had prior dialysis, thus it was deemed appropriate to continue this during their critical illness, but limit other aspects of care. Additionally it may be that clinicians consider KRT to be less invasive than IPPV, despite both carrying a high risk of death.
Study shortcomings include the retrospective nature and focus on two hospitals in an area with a high proportion of older people. All critical care admissions were included, with treatment limitations set within 24 hours, rather than later, often as a reaction to further deterioration attenuating selection bias. 4 However, the cohort had already undergone assessment with a decision to admit to critical care, with a view to having an acceptable likelihood of surviving. Therefore this should not be extrapolated to a general hospital population, when considering escalation decisions. Analysis of outcomes for each frailty group and including advanced directives or patient preferences influencing decision-making could be further studied. We hope this paper stimulates further exploration of this topic. Future prospective, multi-centre work could investigate patients with treatment limitations experience of critical care and quality of life as well as identifying causes of death within this group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.