
Abstract
Introduction
National guidelines suggest recommended staffing levels for therapies. The aim of this study was to capture information on existing staffing levels, roles and responsibilities and service structures.
Methods
An observational study using online surveys distributed to 245 critical care units across the United Kingdom (UK). Surveys consisted of a generic and five profession specific surveys.
Results
Eight hundred sixty-two responses were received from 197 critical care units across the UK. Of those that responded, over 96% of units had input from dietetics, physiotherapy and SLT. Whereas only 59.1% and 48.1% had an OT or psychology service respectively. Units with ring fenced services had improved therapist to patient ratios.
Discussion
There is significant variation in access to therapists for patients admitted to critical care in the UK, with many services not having services for core therapies such as psychology and OT. Where services do exist, they fall below the recommended guidance.
Keywords
Introduction
The role of allied health professionals (AHPs), including Practitioner Psychologists, within critical care has received increasing attention over the last decade 1 . As critical care services place greater emphasis on recovery and rehabilitation, the need for access to specialist AHPs has become ever more apparent 2 . Recent guidelines for the provision of intensive care services (GPICS v2) provide clear recommendations regarding the AHP roles alongside guidance on staffing structures and therapist to patient ratios 3 . Furthermore, there is a dearth of research into the role of AHPs within critical care and recent, yet to be published, evidence gathered by the current authors has emphasised both the lack of existing literature regarding staffing levels, role, and the perceived impact of AHPs on rehabilitation.
Data regarding AHP workforce in critical care have previously been captured via local evaluations and national workforce studies. In 2016 the Critical Care Network National Nurse Leads (CC3N) 4 identified that many critical care units had limited access to AHPs with very limited access to services such as occupational therapy and psychology. More recent guidance, however, supports the role of AHPs within critical care 2,3,5-10. The ‘first wave’ of the covid-19 pandemic highlighted the significant role of AHPs 11 . A recent Intensive Care Society publication, ‘Recovery and Restitution of Critical Care Services during the COVID-19 pandemic 12 highlighted the extreme demands that were placed on the critical care workforce resulting in worsening AHP to patient ratios. However, these extended ratios assumed that existing GPICS standards were being reached pre-pandemic, which based on available data was unlikely 4 .
The aim of this survey-based study therefore, was to explore the existing AHP (dietetics, occupational therapy, physiotherapy, psychology, and speech & language therapy) workforce. The objectives were to gain information regarding service availability, funding, and workforce structure, as well as obtaining insights into profession specific roles.
Methods
Design and Methods of Data Collection and Data Analysis
An observational study using an online survey was used to collect data.
Development of the Surveys
A ‘generic’ survey was devised to gather data on the type of critical care unit and the number of critical care beds. Five profession specific surveys were also developed to capture information regarding AHP’s roles. The chief investigator devised the surveys based on previous examples 4,13–15 with each survey containing identical overarching questions. Once developed by the chief investigator, all draft surveys were reviewed and adapted based on feedback from the research group with profession specific surveys being reviewed by relevant professionals. All surveys were managed by Online Surveys (https://www.onlinesurveys.ac.uk/).
Pilot Study
A pilot study was completed within two NHS critical care networks (NHS Wales Critical Care Network & North-West London Critical Care Network) to ensure the method of distribution and the survey content were appropriate. During the pilot phase, all sites completed both the generic and profession specific surveys and provided feedback on content, structure, and ease of use. Minor changes were subsequently required to the surveys with no major changes indicated. As no questions were added or removed, the pilot data were also included within the main analysis.
Participants
Participants were AHPs working within critical care in the UK and were not excluded based on years of post-graduate or critical care experience to ensure comprehensive data collection. No demographic data were collected.
Distribution Method
Hospitals with at least one critical care unit were identified by the lead AHP of each critical care network, who provided a contact for each hospital. The research team contacted each named hospital contact and provided information regarding the survey, process for distribution to each allied health profession and links to each survey. Only one response was required per profession per critical care unit. The surveys were open for a 12-week period from November 2020 to February 2021. Reminders were sent at 4 and 8 weeks via email to the named hospital contact.
Analysis
Survey data were analysed in Excel (Microsoft Excel, Redmond, WA, USA) and were analysed descriptively. No qualitative data was received.
Critical care beds in the United Kingdom are designated as Level 2 or Level 3 16 . Unlike previous surveys 4 , total bed numbers were used rather than ‘level 3 bed equivalents’. This was to ensure more accurate staff to patient ratios especially for units tending to have more level 2 admissions. One whole time equivalent (1.0 WTE) was 37.5 h/week. For questions exploring direct and non-direct roles, participants were able to respond as ‘never’, ‘rarely’, ‘sometimes’, ‘fairy often’ and ‘very often’. For analysis these were further categorised in two distinct categories, (1) for ‘never’ and ‘rarely’, and (2) for ‘sometimes’, ‘fairy often’ and ‘very often’.
Results
Demographics
A total of 862 responses were received for all AHPs. These contained data for 197 of the 245 (80.4%) hospitals identified through the initial recruitment process.
Staffing
AHP services and staffing in critical care units.
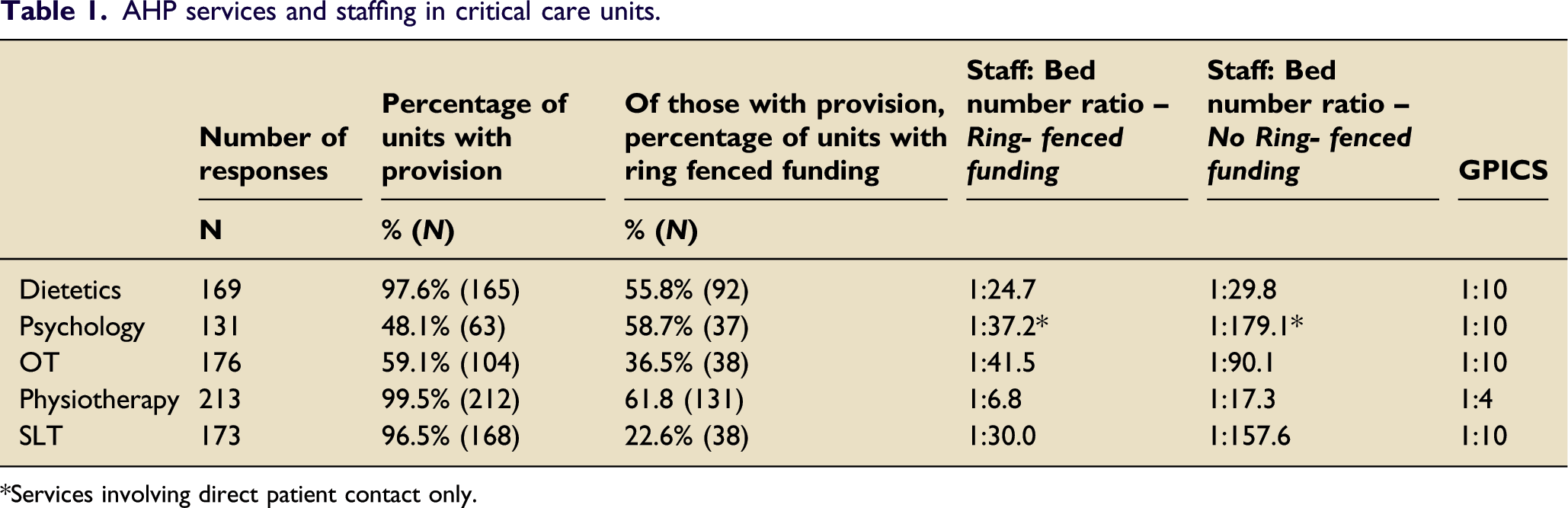
*Services involving direct patient contact only.
Of professions that provided a service, there was variation as to whether these services were funded directly by the critical care unit or were in any way ringfenced to ensure service to critical care. Physiotherapy was most frequently funded by the critical care unit (62%) with SLT least funded (23%), (Table 1).
Therapist to bed number ratios are shown in Table 1, with comparison of those sites with services directly funded by critical care units with those where services were provided via generic resources. For all professions, services directly funded by critical care units had better staff to patient ratios. This was particularly apparent for SLT and OT, although none were compliant with GPICSv2 3 recommendations.
Physiotherapy most consistently provided a service 7-days a week (97.2%) which included on-call and emergency duty rotas. Only dietetics reported no weekend service. OT, SLT and psychology provided weekend input in 7.7%, 6.5% and 1.6% of hospitals respectively.
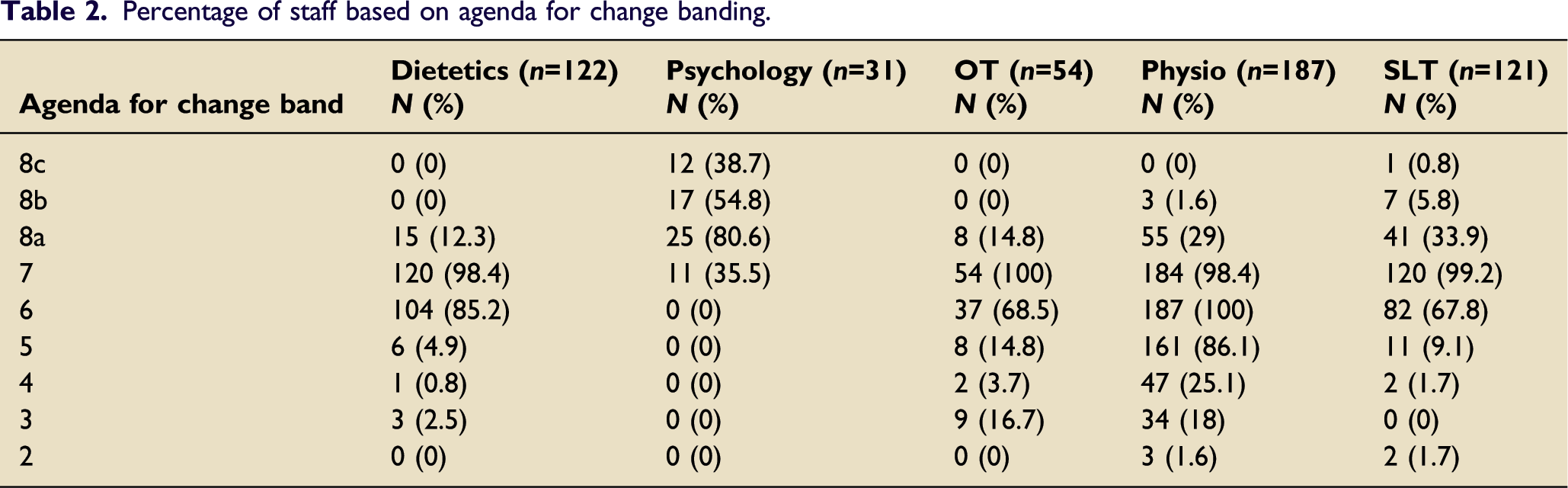
Percentage of staff based on agenda for change banding.
Direct Roles and Responsibilities
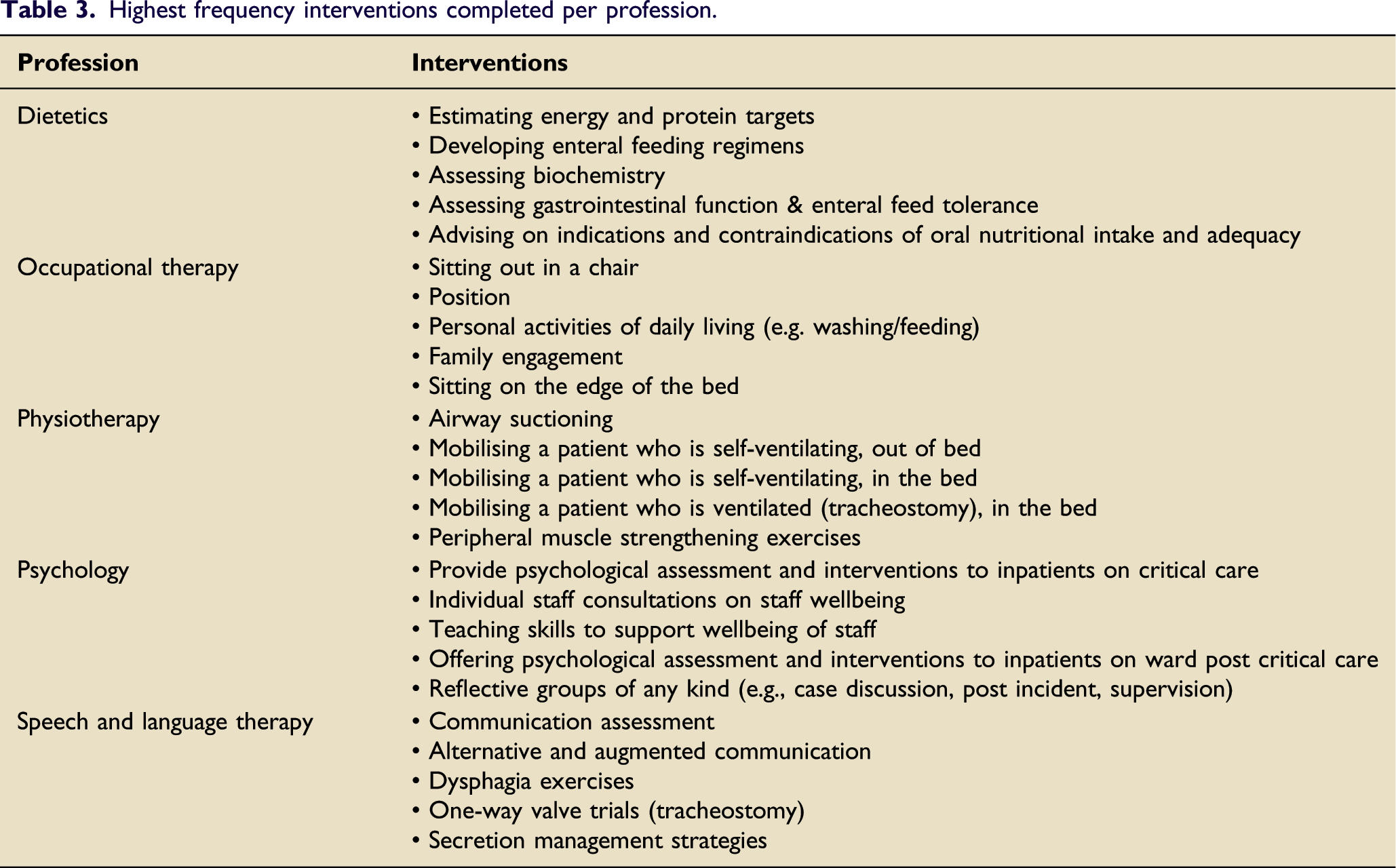
Highest frequency interventions completed per profession.
Non-direct Roles and Responsibilities
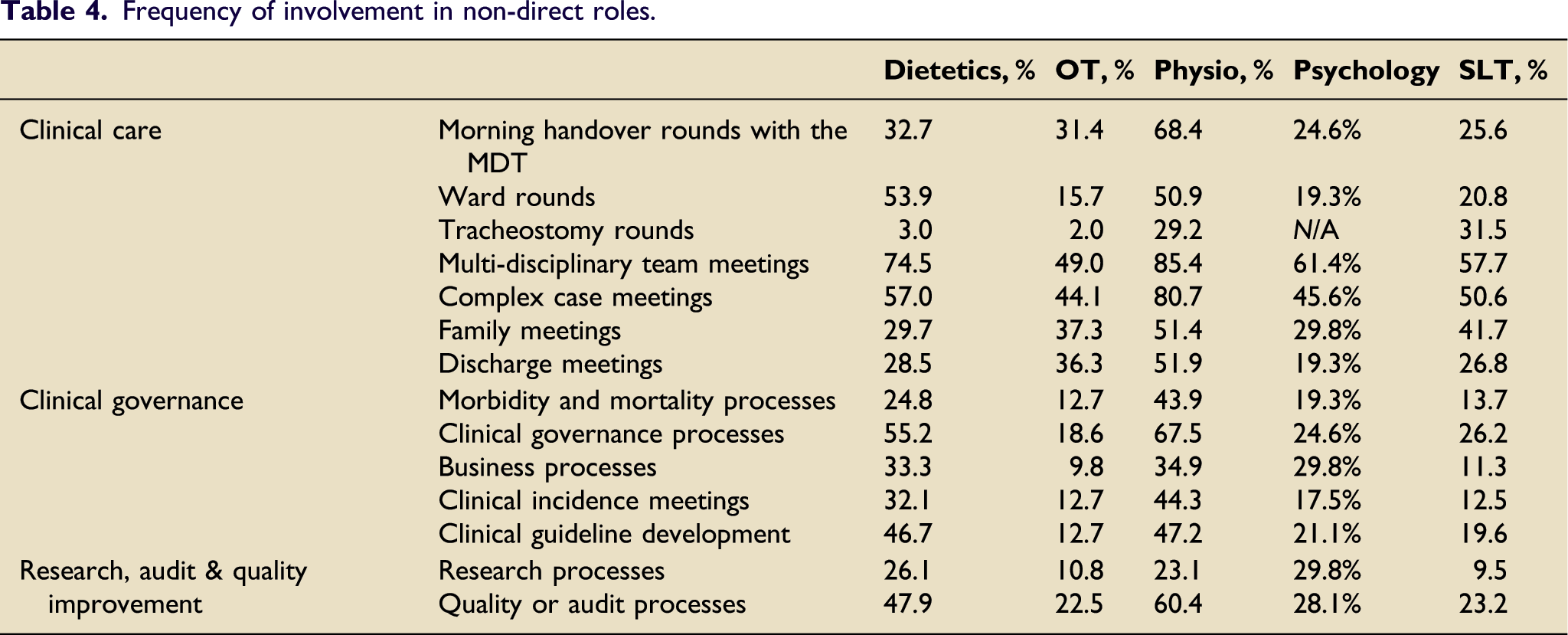
Frequency of involvement in non-direct roles.
Critical care follow-up and post hospital discharge exercises classes
There was variation in involvement in critical care follow-up clinic and post hospital discharge critical care rehabilitation programmes. Physiotherapy was most frequently involved in both follow-up and post hospital discharge critical care rehabilitation programmes (58.2% and 10.3% respectively). Figure 1 shows the responses from all professions. Involvement in critical care follow-up clinic and rehabilitation programmes.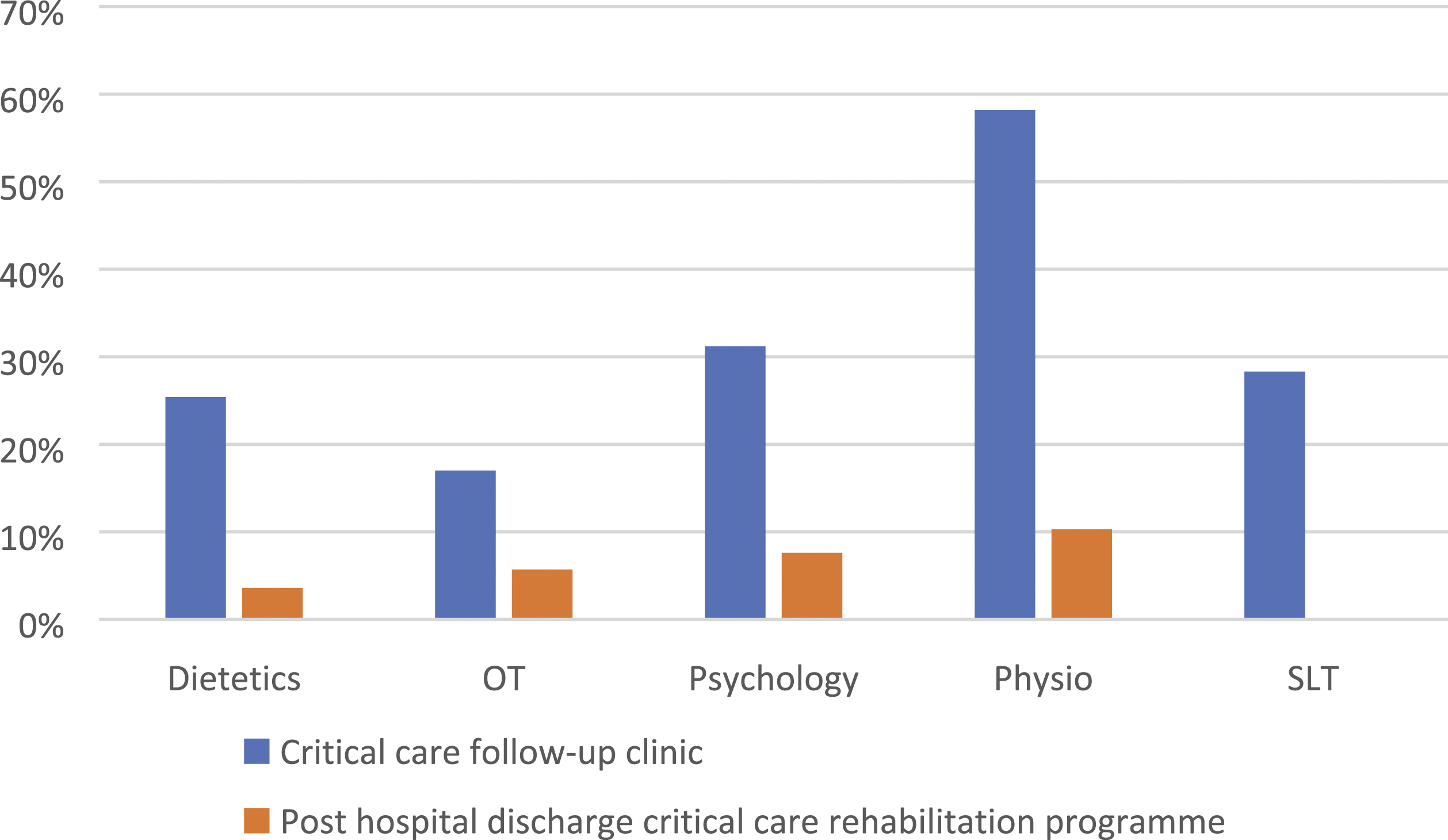
Discussion
Despite recent increased attention, this survey indicates that therapy services to critical care do not meet national recommendations 3 , with many critical care units not providing key services particularly occupational therapy and psychology. Where services do exist, none met the suggested therapist to patient ratios.
Staffing
In 2016, the national critical care non-medical workforce survey 4 identified the shortfall in therapy services. At the time, critical care units reported that 86% of units had access to a dietitian, 14% to OT, 17% for psychology and 30% for SLT (physiotherapy figure not stated). These numbers have now improved, with >90% access to dietetics, physiotherapy and SLT demonstrated in our survey. The current study has also identified the variation in sources of funding particularly whether the therapy service is funded directly by critical care or at least ringfenced in some format. As can be seen in the results, whilst access to services may have improved, these are frequently not directly funded e.g. whilst 96.6% of units that responded may have access to a SLT, in only 23% of those is the service protected.
Therapy services that received direct funding from critical care reported better therapist to patient ratios, with the lowest ratio seen for physiotherapy. However, all therapies reported much higher i.e. worse ratios than those recommended in the guidelines for the provision of intensive care services (GPICS) 3 .
Variation was observed across the professional groups regarding agenda for change banding. To our knowledge this is the first study exploring staffing frequency based on UK agenda for change and therefore comparison with existing findings is not possible. Critical care therapy support workers are becoming increasingly recognised 3 , as reflected in the physiotherapy results indicating staff within bands 2–4. Support workers were not previously included in critical care workforce surveys and therefore comparison is not possible.
National guidance documents 3,5,17 highlight the need for critical care input across the recovery pathway including follow-up clinics and ongoing rehabilitation post discharge. The development of the Post-ICU Presentation Screen (PICUPS) tool has shown potential to better identify rehabilitation needs at varying stages of patient’s recovery and suggests when AHP intervention is necessary18,19. However, the current survey shows variation across professions regarding involvement in follow-up clinics or post discharge rehabilitation classes. Although all professions reported some involvement in follow-up clinic, it is not known if this is regular attendance or ad-hoc. This finding is also supported in a recent review of recovery, rehabilitation and follow up services 20 . Whilst improvements in AHP involvement in follow-up clinic has improved since previous findings 21 , psychology remains most frequently cited as lacking 20 , with the current study suggesting only 31.2% (n=41) of services having any form of involvement. Additionally, involvement in post hospital critical care rehabilitation programmes remains low with physiotherapists most frequently involved but only at 22 (10.3%) sites across the UK.
Direct roles and responsibilities
The role of therapists within critical care has previously been explored 4 however details and clinical frequency of interventions were not investigated. The minimum standards of clinical practice by physiotherapists have been explored in three countries each reporting similar outcomes 22–24. In the UK version, 107 assessment or treatment interventions were deemed as essential skills 22 . Whilst not all of these were explored in the current survey, the role of physiotherapy within airway clearance and rehabilitation remains clear. Similarly, other therapy professional groups suggested regular use of interventions previously recognised within the literature 25–28 e.g. estimating energy and protein targets (dietetics), personal activities of daily living (OT), offering psychological assessment and interventions to inpatients on critical care (psychology) and communication assessments by SLT. These results can now be used as a baseline for future studies and to guide ongoing discussions on roles within critical care.
Indirect roles and responsibilities
Whilst therapists are recognised as core members of the critical care multi-professional team 2,3,17, their involvement in non-direct elements of services e.g. research, business meetings etc., was previously not known. Based on the current findings, physiotherapists most frequently attended and/or participated in indirect elements of the service. Specifically, involvement in research and business processes remain low. SLT reported the lowest frequency of involvement across all categories, which may reflect staffing ratios and the low percentage of roles directly funded by critical care. All these aspects require further investigation particularly around the impact of direct ‘ring-fenced’ funding and the need for therapy staff to be involved in these non-direct activities 3 . Whilst not reflected in this survey, it is also likely that therapists have line management responsibilities within their respective departments e.g. appraisals and recruitment as seen previously (4).
Limitations
A total of 197 of the 245 (80.4%) hospitals identified through the initial distribution process completed at least one of the surveys. All UK-nations responded with representation from every critical care network. However, few hospitals completed all surveys and there were lower response rates within certain professions e.g. psychology. There are many potential reasons for this. The survey was distributed to a therapist in every hospital; however, it was then reliant on that person to forward to appropriate people. In hospitals where services do not exist, it may not have been clear to the local link, who it should be forwarded to, therefore resulting in non-completion. If these units do not have therapy services to critical care, then the true UK-picture is likely to be worse, with a lower percentage of units having any form of input from each of the therapy professions. Furthermore, this survey was initiated towards the start of a peak of the covid-19 pandemic and remained open for 12 weeks. Increased clinical workload, staff sickness and self-isolation, and participant fatigue may have contributed to reduced completion.
Future research
This study has shown that existing AHP workforces within critical care fall below national recommendations. Furthermore, despite increasing guidance and evidence of the importance of integration of AHPs into critical care services, this does not appear to be translating into existing services especially regarding in-direct aspects of patient care and clinical governance. Future research must now focus on the impact of AHP services to critical care, and on patient outcomes.
Conclusion
There is significant variation in access to therapists for patients admitted to critical care in the UK, with many services not having services for core therapies such as psychology and occupational therapy. Furthermore, despite national guidance suggesting therapist to staff ratios, the results of this survey suggest that even where services exist, these do not meet recommendations.
Footnotes
Acknowledgements
The authors thank Heleen van Aswegen, Claire Mills and Mark Borthwick for sharing previous surveys exploring therapy workforces and all staff who completed the questionnaire surveys.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Raw data available by direct request to the corresponding author.
Ethics Approval
This study was discussed with the local research and development department and Health Care Research Wales and deemed not to require full ethical application. All information collected was routinely collected data and no identifiable data was used within the analysis or manuscript.