
Abstract
Background
Delirium is a common complication of critical illness with a significant impact on patient morbidity and mortality. The Greater Manchester Critical Care Network established the Delirium Reduction Working Group in 2015. This article describes a region-wide delirium improvement project launched by that group.
Methods
Multiple Plan-Do-Study-Act cycles were undertaken. Cycle 1: April 2015 demonstrated only 48% of patients had a formal delirium screen. Following this a network-wide event took place and the Delirium Standards for the Greater Manchester Critical Care Network were produced. Cycle 2: May 2016 quarterly audits across the network monitored compliance against the agreed standards. Group events involved implementation of a delirium care bundle, sharing best practice, educating staff and providing guidance on the management of delirium. Cycle 3: November 2016 quarterly audit continued and a regional delirium study day was rolled out across the region.
Results
We have 14 different units across our network, all of which have participated in the audit. The first audit showed a delirium point prevalence of 28%, subsequent point prevalence audits demonstrated rates as low as 13%. There has also been an improvement in the use of delirium screening tools. In the first audit 37% of patients had two delirium screens in 24 h, this has increased to 60% in the latest audit. Improvements were also made in availability of sensory aids and pain assessments.
Conclusion
The project has demonstrated the feasibility of delivering a coordinated delirium improvement project across multiple critical care units.
Introduction
Delirium is a common complication of critical illness, which confers a significant burden of morbidity and mortality. A meta-analysis of 42 studies published in 2015 found an incidence of 31.8%. 1 Studies have shown delirium to be an independent predictor of long-term mortality and cognitive impairment and that it increases duration of mechanical ventilation, intensive care stay and hospital stay.1–3 Delirium is one of the top three James Lind Alliance priorities for intensive care. 4
Delirium, in the critically ill, is difficult to identify and assess. Studies have shown that clinicians detect less than one-third of delirium in patients. 5 There are two validated screening tools for use in intubated patients, the Confusion Assessment Method for the ICU (CAM ICU) and the Intensive Care Delirium Screening Checklist. 5
Unfortunately there is no evidence that any single treatment is able to reduce the incidence or duration of delirium, therefore management primarily focuses on addressing the possible underlying causes and ensuring effective communication and reorientation. 6
The Greater Manchester Critical Care Network (GMCCN) was established in 2002 as a collaborative partnership bringing together clinical services to work together to promote the highest quality critical care services. It was formalised in 2013 as the Operational Delivery Network but its remit has remained unchanged; to ensure that critical care services are delivered in a safe and effective way thereby ensuring that patients receive consistently high quality care and experience.
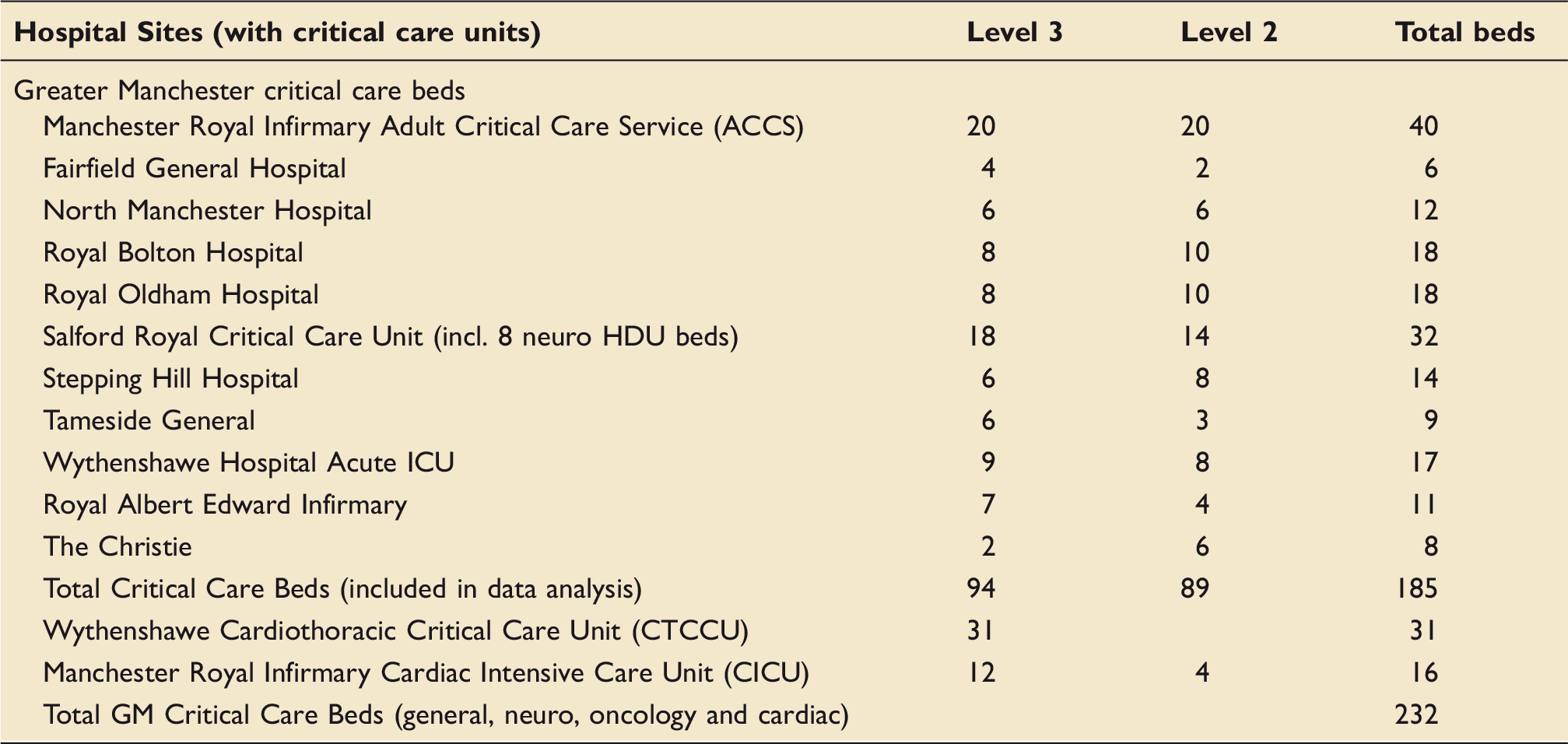
In April 2015 the GMCCN formed a Delirium Reduction Working Group with the aim to reduce the incidence and duration of delirium across the network using a multi-faceted approach. The group is made up of doctors, nurses and other health professionals from across critical care units in our network. The network spans a large area covering the ten metropolitan boroughs of Greater Manchester – Bolton, Bury, Oldham, Rochdale, Stockport, Tameside, Trafford, Wigan, Manchester and Salford.
Distribution of critical care beds in Greater Manchester.
We used The Institute for Healthcare Improvement (IHI) Model for Improvement 7 to adopt a Plan-Do-Study-Act (PDSA) cycle approach. This paper summarises the incremental cycles of delirium reduction and quality improvement and the resulting improvement in delirium screening and point prevalence rates.
Methods
PDSA Cycle 1 – April 2015
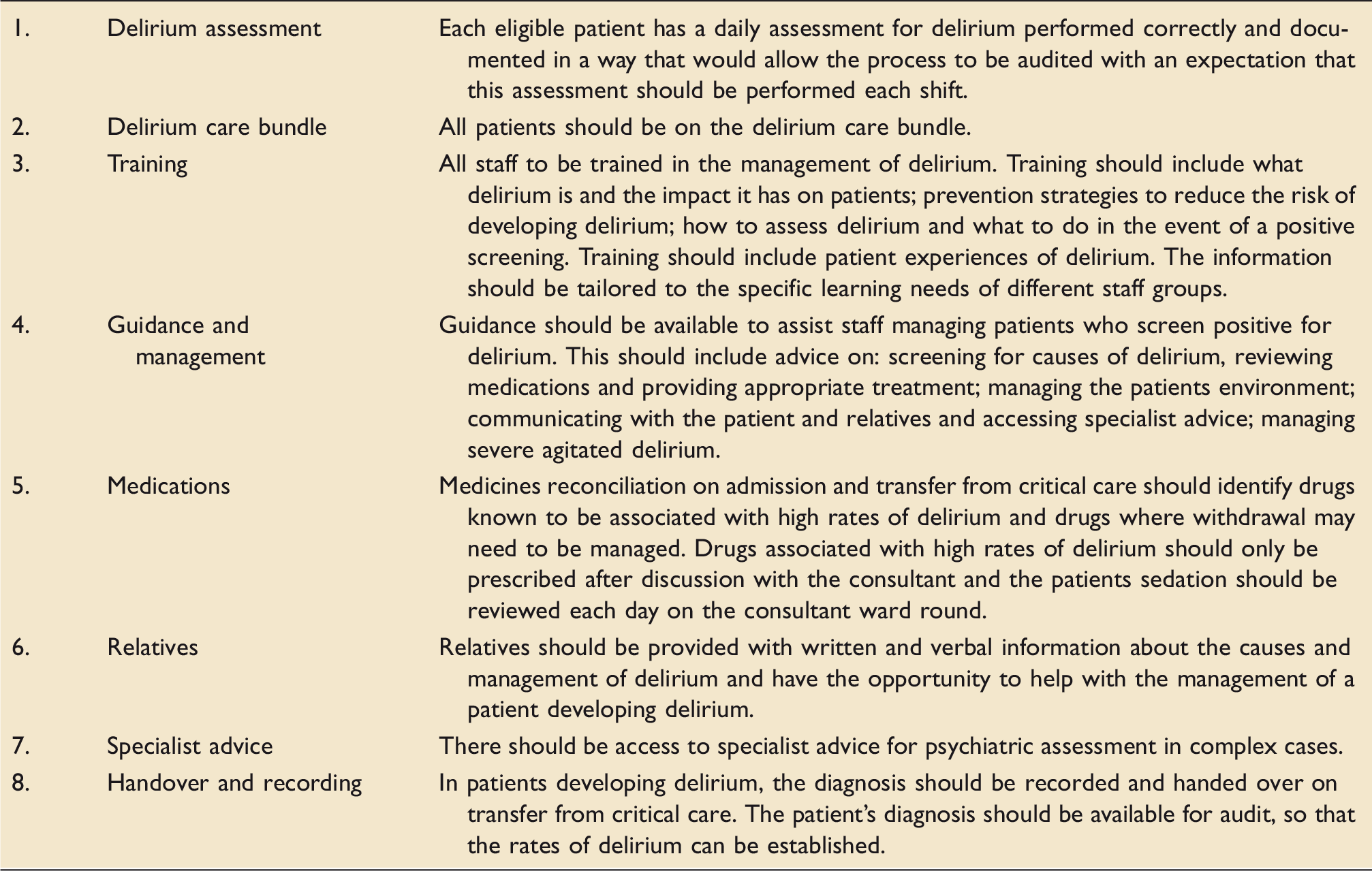
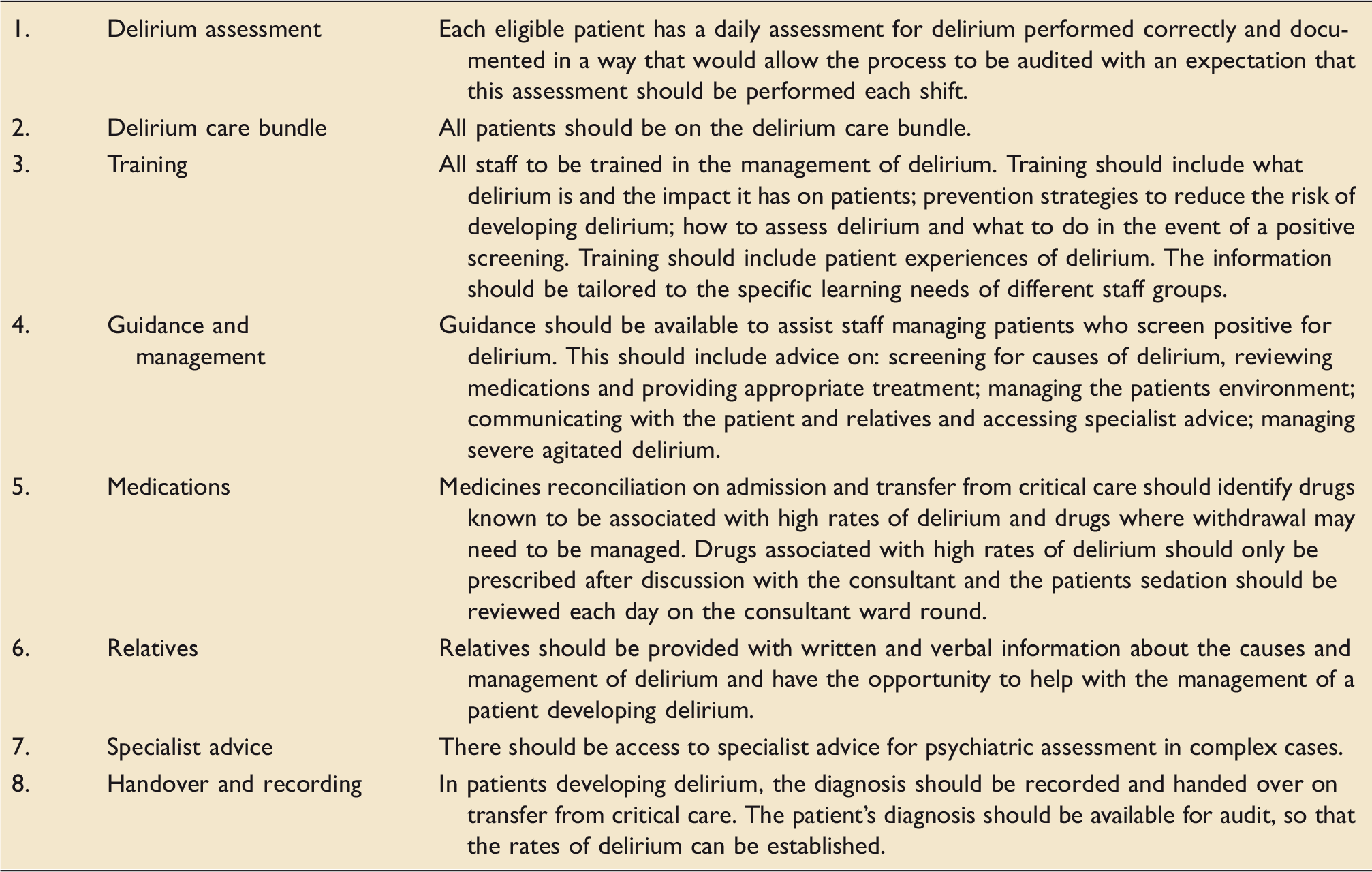
Delirium Standards for the Greater Manchester Critical Care Network.
Delirium care bundle.
An initial audit was performed to determine current practices related to identification and management of delirium including the use of a delirium-screening tool across the region. This was a snapshot audit covering all the patients on the unit on a single day. Nursing staff, in many cases the delirium link nurse for the unit primarily collected the audit data. The delirium link nurse is a nurse who has agreed to lead on delirium locally and attend the regular network meetings, engaging with the quality improvement activity associated with it. Most of the information, such as CAM ICU scores, pain assessments and RASS scores were obtained from the daily observation chart. Other nursing documentation recorded information about the need for glasses, dentures and hearing aids and the physiotherapy and mobilisation plans. Personalised care involved finding out what mattered most to the patient, ascertaining their likes and dislikes and giving them the opportunity to have personal belongings with them. The location of this information varied between trusts. Data collectors could identify themselves which patients were able to see clocks.
PDSA Cycle 2 – May 2016 onwards
Quarterly audit was performed across the network looking at compliance against the delirium standards and results fed back at the Delirium Reduction Working Group meetings. We focused on implementation of a delirium care bundle, sharing best practice, educating staff and providing guidance on the management of delirium. During this time we had a focused effort to improve the provision of clocks showing both time and date available for all patients and the introduction of patient passports to aid in the delivery of personalised patient care. The passports document patients’ likes and dislikes and provided a set place to record the need for glasses and hearing aids. A copy of the patient passport can be found in the online appendix.
PDSA Cycle 3 – November 2016
We continued with quarterly audit and meeting of the Delirium Reduction Working Group. There have been eight audit cycles to date. We compared the number of patients in the first audit with delirium to the number of patients with delirium in the last audit using Fishers Exact Test.
Introduction of a delirium section in the GMCCN Skills Institute Critical Care Course has enabled up to date training for nursing staff across the network. Every nurse who is appointed to a job in critical care in a unit that does not provide a critical care course needs to undertake the GMCCN course. They cover sedation, delirium and rehabilitation with a focus on definition of delirium, types of delirium, risk factors for delirium, deliriogenic drugs and consequences and treatment of delirium. The course is run twice a year with staff generally attending 6–12 months after starting in a post. We also began to distribute a delirium e-learning package. It is hosted on the Greater Manchester Cares online platform. A link can also be found on the GMCCN website. It takes around 30 min to complete and is suitable for both medical and nursing staff. It has been left to the discretion of the individual trusts whether it is voluntary or mandatory for staff. Currently it is mandatory in three trusts in the region.
Results
Audit data returned for each unit.
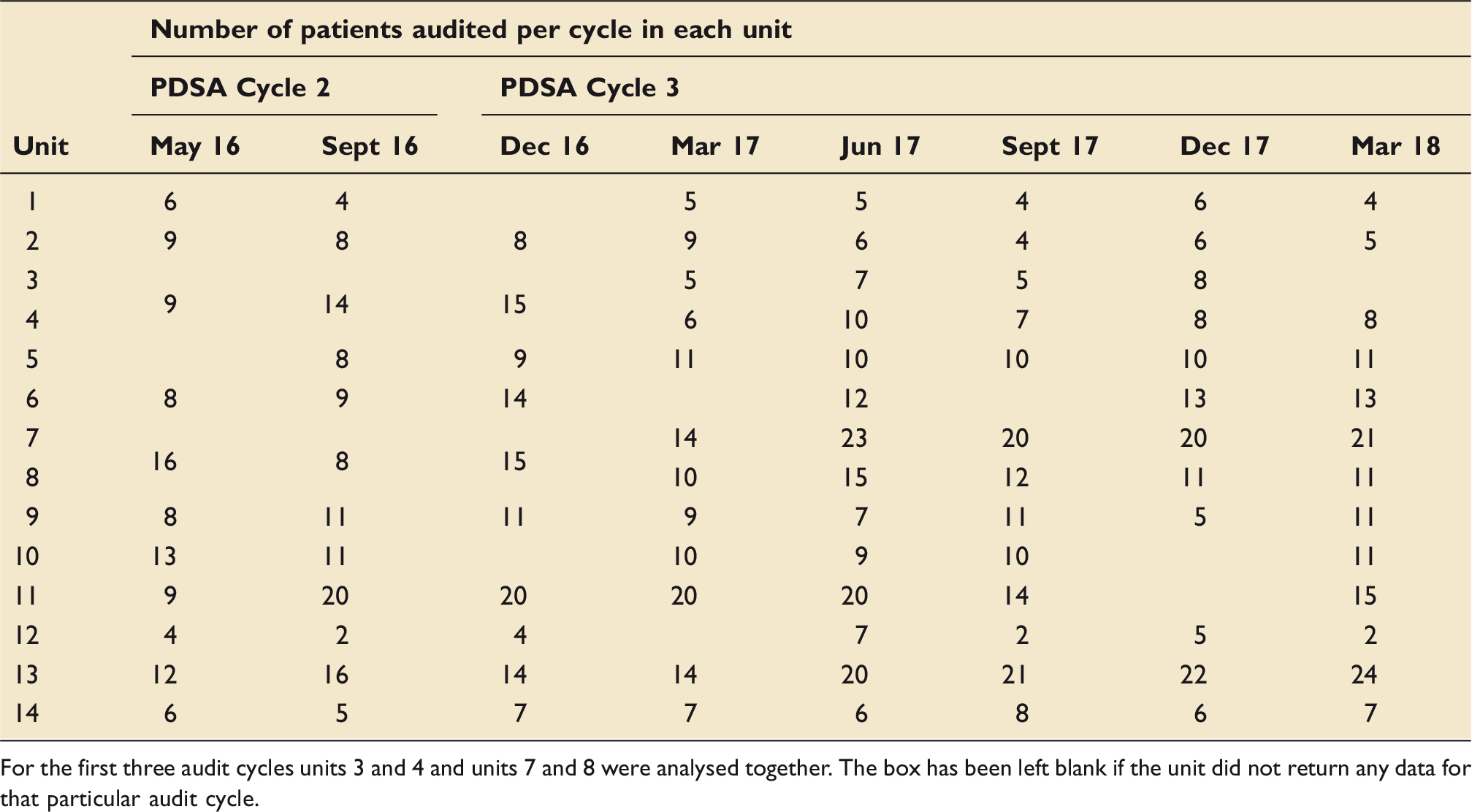
For the first three audit cycles units 3 and 4 and units 7 and 8 were analysed together. The box has been left blank if the unit did not return any data for that particular audit cycle.
The first audit in May 2016 showed a delirium point prevalence of 28%, the most recent showed a point prevalence of 13%. There was a sustained low rate of delirium maintained throughout the audit period. Figure 1 demonstrates the point prevalence of delirium throughout the region over consecutive audit periods.
Point prevalence of delirium across the network over consecutive audit periods.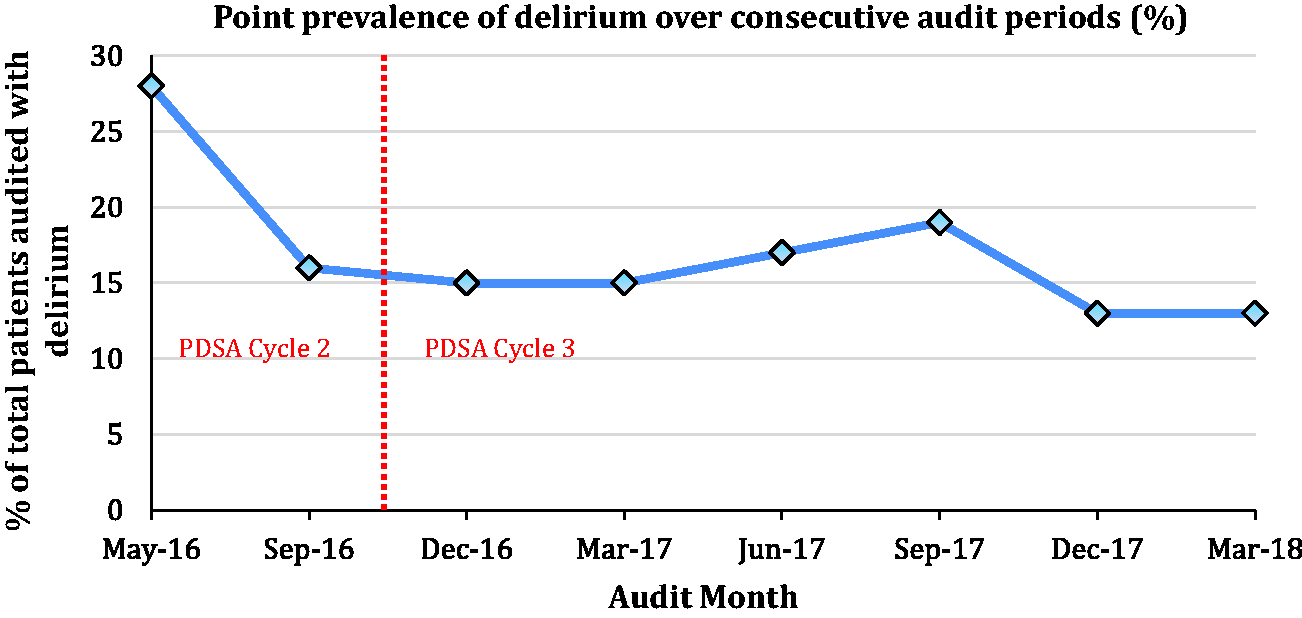
Number of patients with delirium in initial audit cycle vs. last audit cycle. a
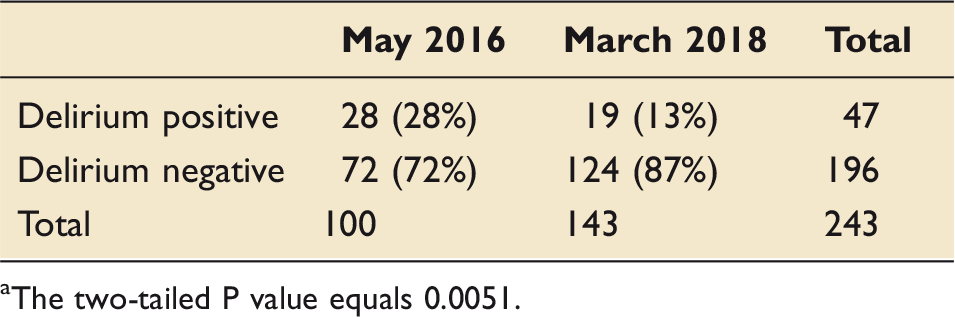
The two-tailed P value equals 0.0051.
Figure 2 shows the data for the individual units.
Point prevalence of delirium in the different units over consecutive audit periods.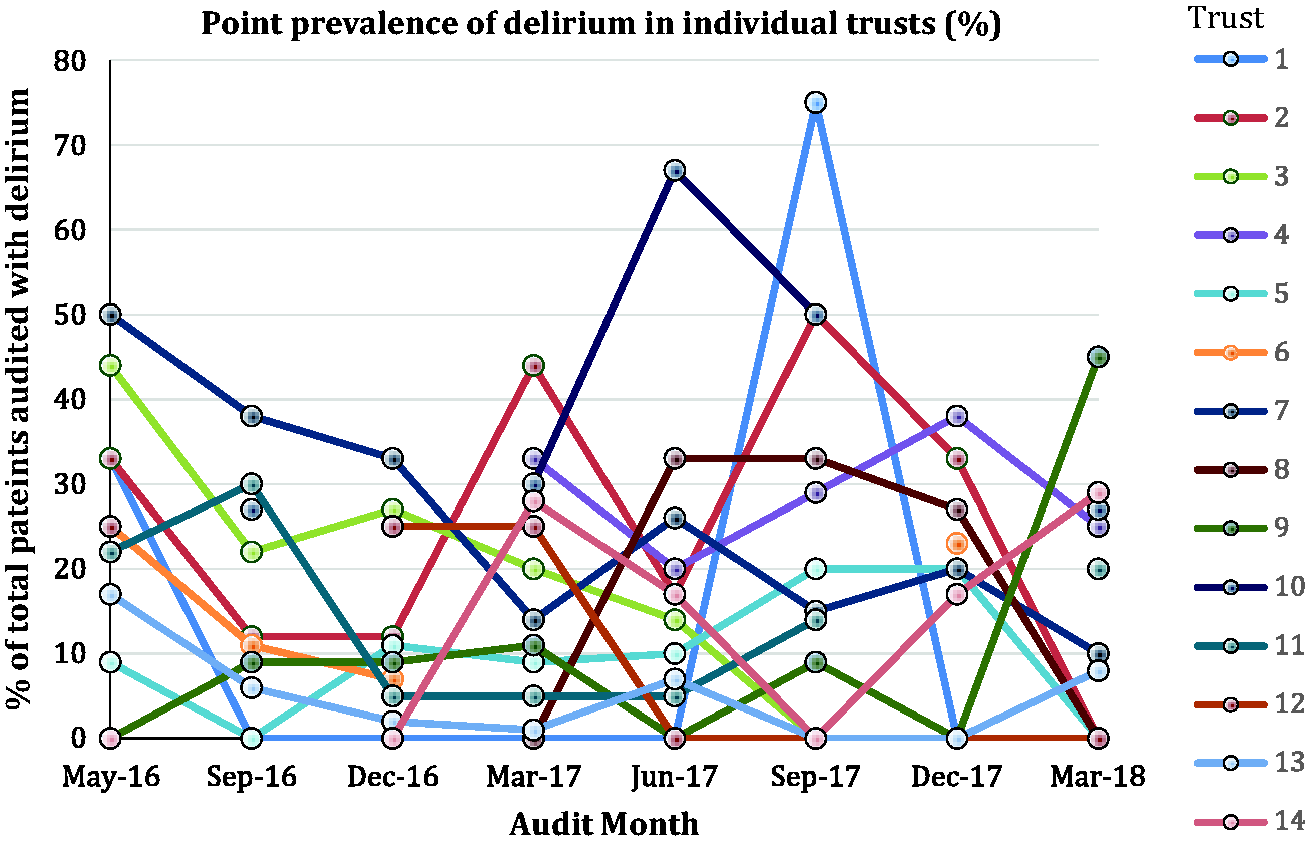
There has been improvement in the use of delirium screening tools. One of the network targets in the delirium care bundle is that each patient should have a minimum of two CAM ICU screens in a 24 h period. In the first audit 37% of patients met this target; this has increased to 60% in the latest audit and has been consistently above 50% since June 2017. This can be seen in Figure 3.
Graph demonstrating the increase in percentage of patients meeting network target of two CAM ICU screens in 24 h over consecutive audits.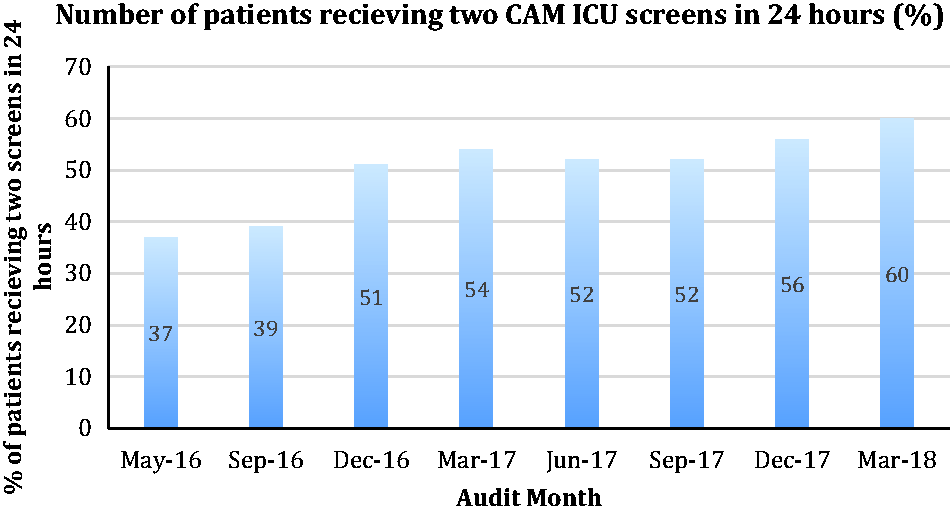
Progress has also been made in other areas. Figure 4 demonstrates the increase in the number of patients with evidence of personalised care over the consecutive audit periods.
Increase in evidence of personalised care over consecutive audit periods.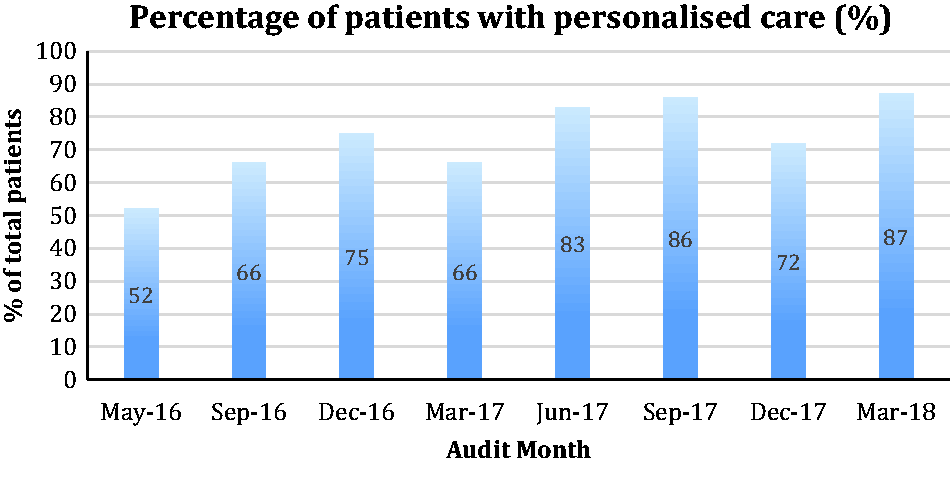
The number of patients who have had a documented physiotherapy and mobilisation plan and who have had a pain assessment within the last 4 h was consistently over 80%. The results of this can be seen in Figure 5.
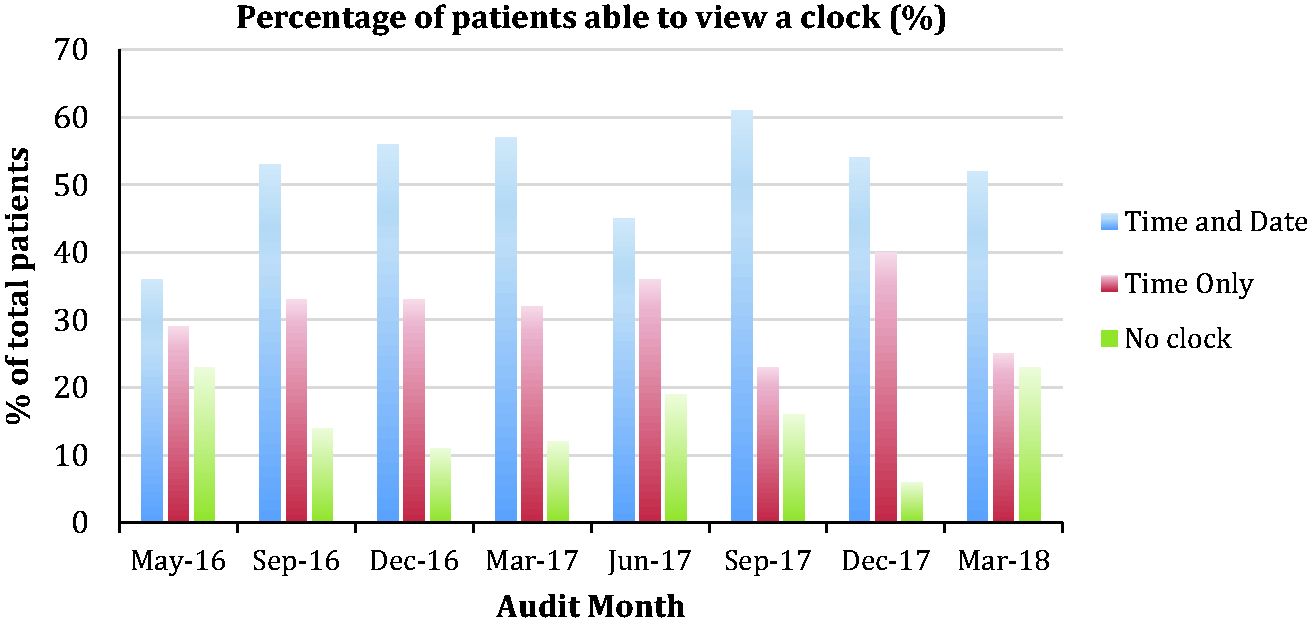
One of our standards is that every patient should be able to see a clock displaying both the time and date. The results of this can be seen in Figure 6.
Graph showing the percentage of patients who have had a documented physiotherapy/mobilisation plan and who have received a pain assessment within the last 4 h over the consecutive audits. Percentage of patients able to view a clock over the consecutive audit periods.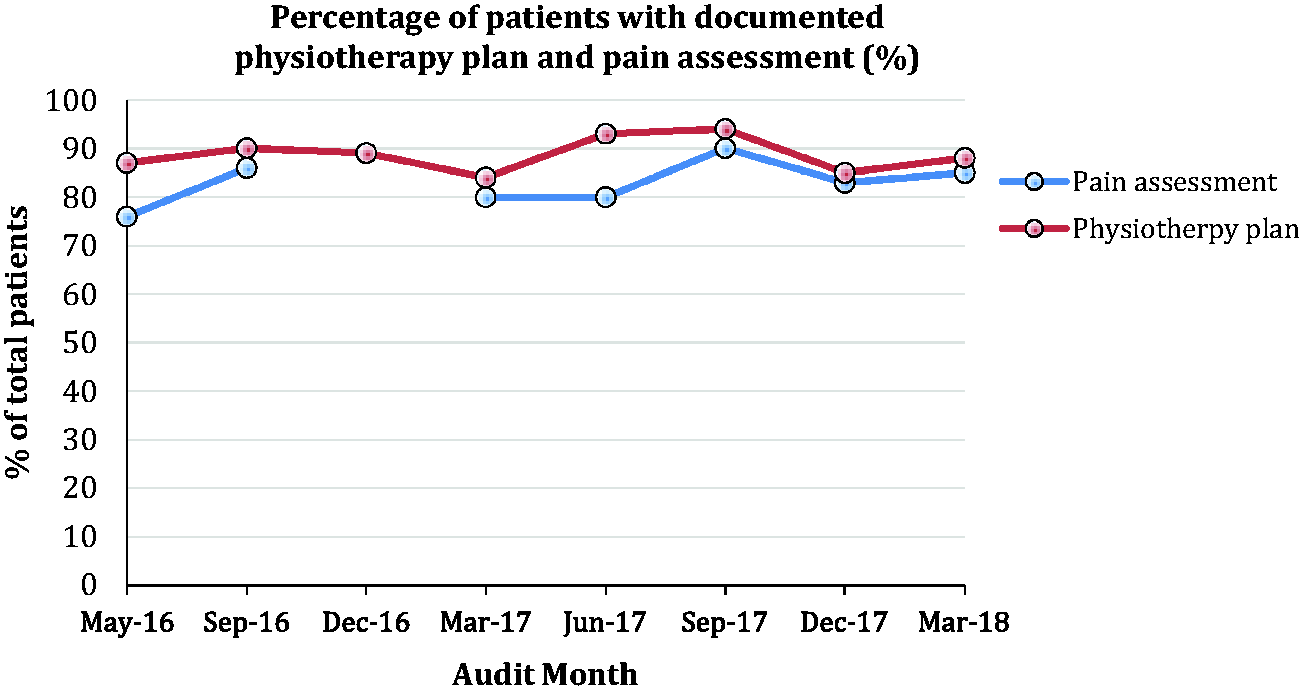
Discussion
This coordinated project across 14 critical care units in Greater Manchester has improved delirium screening and care. The initial large reduction in the point prevalence of delirium may have been a genuine reduction in cases or an artefact of higher sampling rates. However, subsequent years have been successful in demonstrating a sustained low rate of delirium. We anticipate it will be impossible to reach zero rates of delirium and that the plateau we have reached now may represent a cohort of patients with unavoidable delirium and risk factors that cannot be modified.
Delirium screening has improved and we hope this will continue as more staff complete the regional study day and e-learning package. We have also uploaded a video to the GMCCN website demonstrating how to perform a CAM ICU screen correctly. The introduction of patient passports has contributed to improving compliance with providing personalised care for each patient and provides a standard place to record each patient’s need for sensory and mobility aids. There are still a number of areas we would like to see greater improvements. One of our standards is that every patient should be able to see a clock displaying both time and date. This has improved from 33% in the initial audit, but the aim is for 100%, which is proving to be an ongoing challenge, particularly in the large units. We would also like to see an improvement in the availability of sleep packs. The data for this section was not always complete on the audit proformas, but the limited results we did have indicated that sleep packs were not always offered.
There are numerous strengths to our project. We have received network-wide cooperation and had far-reaching impact across all the trusts in the Greater Manchester area, raising both the profile and priority of delirium. We have seen a cultural change with regard to the necessity of delirium screening and produced a more holistic and non-pharmacological multi-disciplinary approach to the treatment.
As with all studies there have been a few limitations. The before and after nature of the study means there will have been confounding factors and likely other improvements running concurrently that will have contributed to the improvement in our rates of delirium. The multi-faceted approach to treatment also means we cannot be sure which aspect of our care bundle has had most impact on our delirium reduction.
This project has demonstrated that a network-wide quality improvement project can produce sustained improvements in delirium care in multiple critical care units across a city-wide area.
Footnotes
Acknowledgements
We would like to acknowledge the work of all the members of the Delirium reduction Working Group, without which this article would not be possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: James Hanison has received an honorarium from Orion Pharma. Daniel Conway has received an honorarium from Orion Pharma and is chair of the Critical Care Rehabilitation Group for the GMCCN.
Supplemental material
Supplemental material for this article is available online.