
Abstract
Introduction
Physical, psychological and cognitive impairments are common in survivors of critical illness. 1 These impairments, collectively known as Post-Intensive Care Syndrome (PICS), diminish quality of life and are burdensome for patients, carers and society.2,3 An increasing awareness and recognition of PICS has prompted commitments to enhance multidisciplinary aftercare with the overall goal of improving patient-centred outcomes and health-related quality of life.
Resumption of driving represents a crucial recovery milestone. For those patients who are licence holders, return to driving may promote independence and enable other determinants of recovery such as social activity and return to employment. Driving is, however, a complex task necessitating intact cognition (executive skills, visual perception, attention, memory and comprehension), physical ability (strength, sensation, coordination and reaction speed) as well as emotional preparedness. 4 These elements may all be affected after critical illness. 5
National and international guidance regarding fitness to drive covers neurological, cardiovascular and respiratory conditions.4,6,7 Although specific components of PICS such as cognitive impairment and limb dysfunction are discussed in the guidance, with a legal requirement to notify DVLA of cognitive defects, the combined impact of an individual’s interacting PICS domains on driving suitability is not addressed. Thus, healthcare professionals and individuals lack consistent advice as to when driving resumption can occur. Individuals may self-determine suitability to drive without professional guidance. Premature resumption carries risks to both self and other road users. Conversely, return to driving should not be arbitrarily prohibited or unduly prolonged. Enabling return to driving is important as it allows independence and return to everyday activities. Very little evidence exists to guide clinicians and patients following critical illness. Wolfe and Lehockey (2016) suggest clinicians should take into account functional ability and medical history, including conditions that may impair ability to drive and react, and correlate these factors with the risk for driving accidents. 8 Presently, little is known about when, or if, patients return to driving after critical illness and what barriers patients experience in relation to this activity. The aim of this study was to explore and gain insight into driving practices of individuals following critical illness.
Methods
Design
An anonymised, cross-sectional, questionnaire was used to ascertain both quantitative (age, gender, driving status, time course of driving resumption) and qualitative experiential aspects of driving resumption (via open-ended questions). The primary outcome was the prevalence of driving resumption at 3 months following ICU discharge.
Setting
This study was undertaken in the adult critical care department of a large UK District General Hospital with 18 beds, approximately 800 admissions per year, ICU mortality of 18.9%, and mixed medical/surgical case mix.
Respondents
Driving licence-holding adults having undergone four or more days mechanical ventilation attending the Rehabilitation After Critical Illness outpatient clinic between 3 and 12 months after hospital discharge were eligible to participate.
Fifty consecutive clinic attendees between 2014 and 2015 were invited to complete a short, anonymised questionnaire to solicit quantitative (timing) and qualitative data (open-ended textual responses) about driving resumption. Informed consent was sought from all respondents and completion of the survey was considered indicative of consent. Royal Berkshire NHS Foundation Trust R&D approved this work as a service evaluation.
Materials and procedure
Survey questions were devised by an iterative process and were considered for content and face validity by two researchers (JM and CW). Five questions were included in the final questionnaire (listed in Supplemental Table 1). Respondents could opt to complete the handwritten paper survey whilst in clinic or alternatively in their own time by postal return. Respondents received assurance that any ongoing treatment or care would not be affected by participating in the survey.
Data Analysis
Quantitative data were of the nominal/ordinal form and analysed using SPSS Version 25 using descriptive frequency analyses (percentages). Continuous data were reported as a median and range. The Kaplan-Meier method was used to analyse time-to-event i.e. days from ICU discharge to driving resumption.
Qualitative textual data from the open-ended questions were analysed into themes using framework analysis. 9 This is an established approach used in numerous health research studies, and it is not uncommon to use open-ended survey text as a qualitative data source.10,11 Themes for the framework were derived from the data, with the framework refined as data analysis took place. Data were examined by two researchers to ensure consensus was reached across each theme and how comments were attributed under those themes. These two researchers transcribed and analysed the handwritten survey data independently before agreeing the key themes for the framework analysis. This was then applied across all the data. A third researcher independently reviewed the raw data and choice of themes in the framework to increase robustness and reduce potential bias.
Results
45 out of 50 respondents completed the questionnaire (90% response rate). The median age of respondents was 60 years (range 27–82), and 50% female. 43 respondents possessed a valid driving licence and declared an intention to resume driving. Two respondents had surrendered their licence on medical grounds. The surveyed population was reflective of the diverse critical care unit admission source: emergency admission 39%, post-operative admission 25%, medical inpatient ward admission 29%, other 7%.
43 out of 45 respondents provided information about driving resumption timeframes. The primary outcome, the proportion of respondents who had resumed driving by the 3 months time-point after ICU discharge, was 68% (n = 31). By the 6 months time-point the proportion was 77% (n = 35).
The median interval between ICU discharge and resumption of driving was 8 weeks. The time period for resumption was markedly variable ranging from 1 to 52 weeks post ICU discharge (Figure 1). 16% had not resumed driving by the 1 year time-point. Kaplan-Meier curve time to driving resumption after ICU discharge.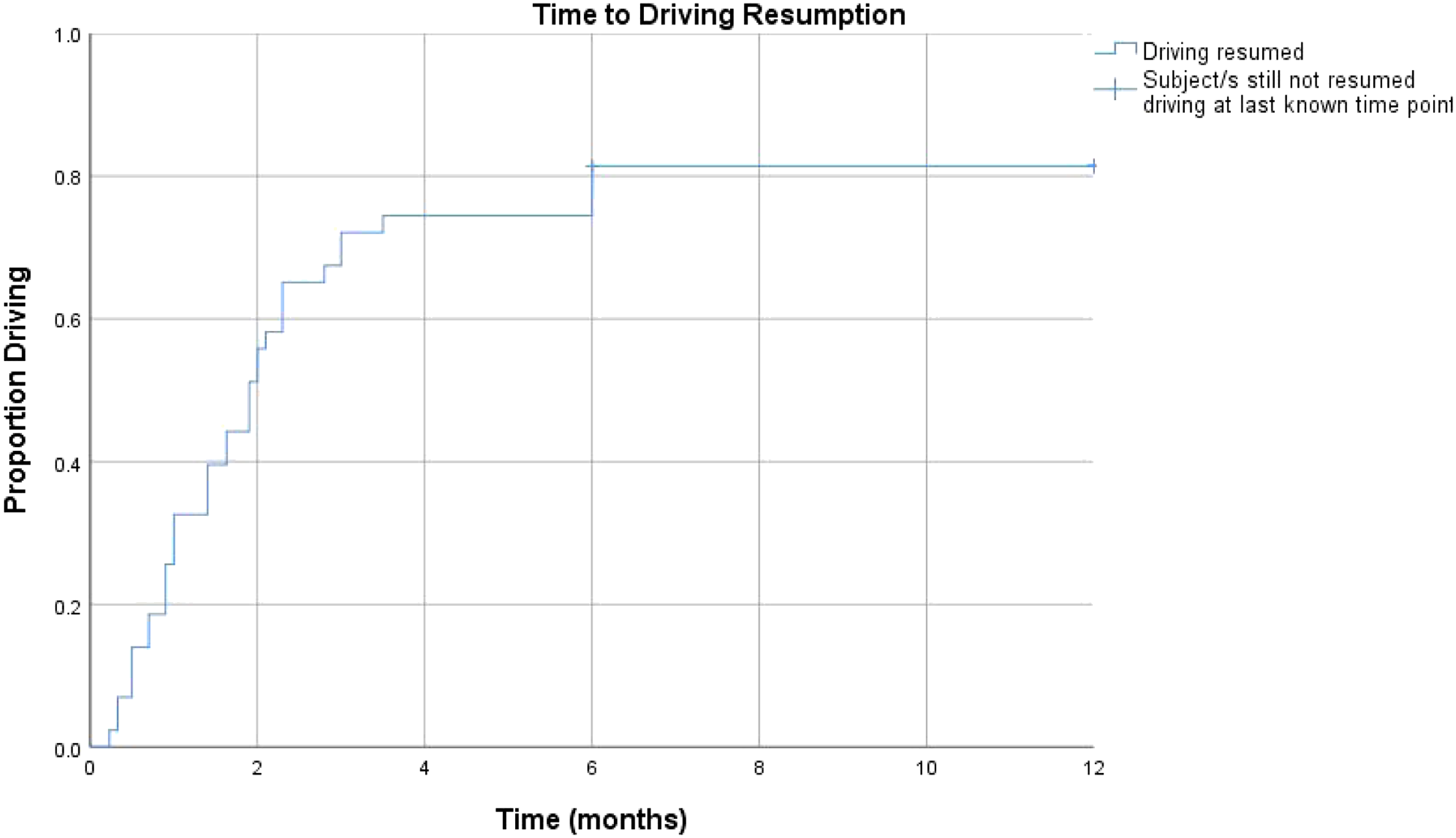
Sources of advice received by respondents.
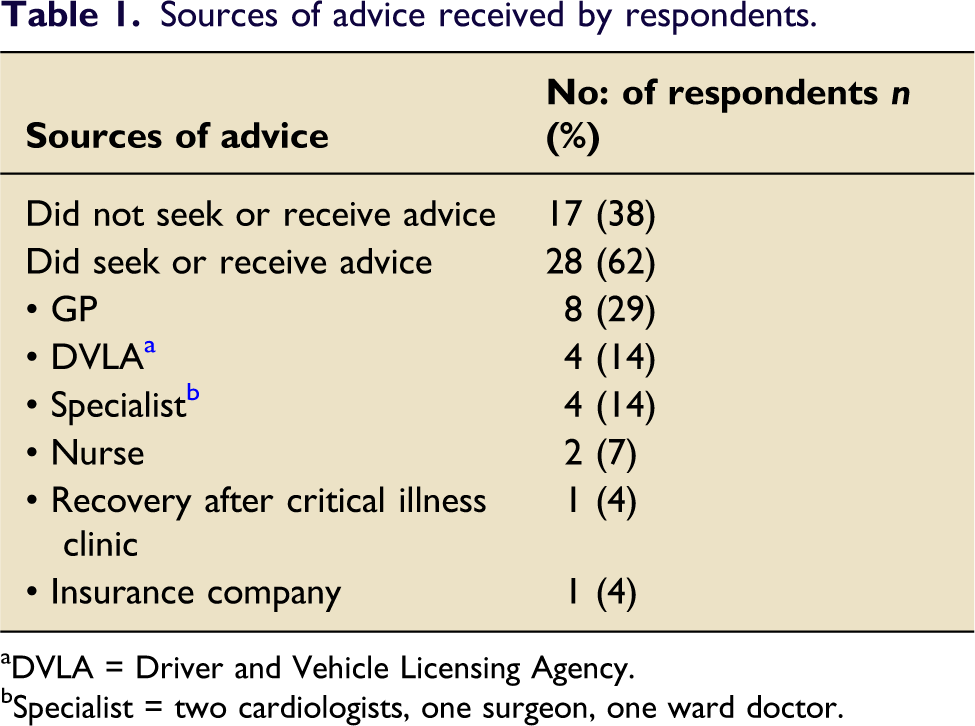
aDVLA = Driver and Vehicle Licensing Agency.
bSpecialist = two cardiologists, one surgeon, one ward doctor.
Qualitative analysis
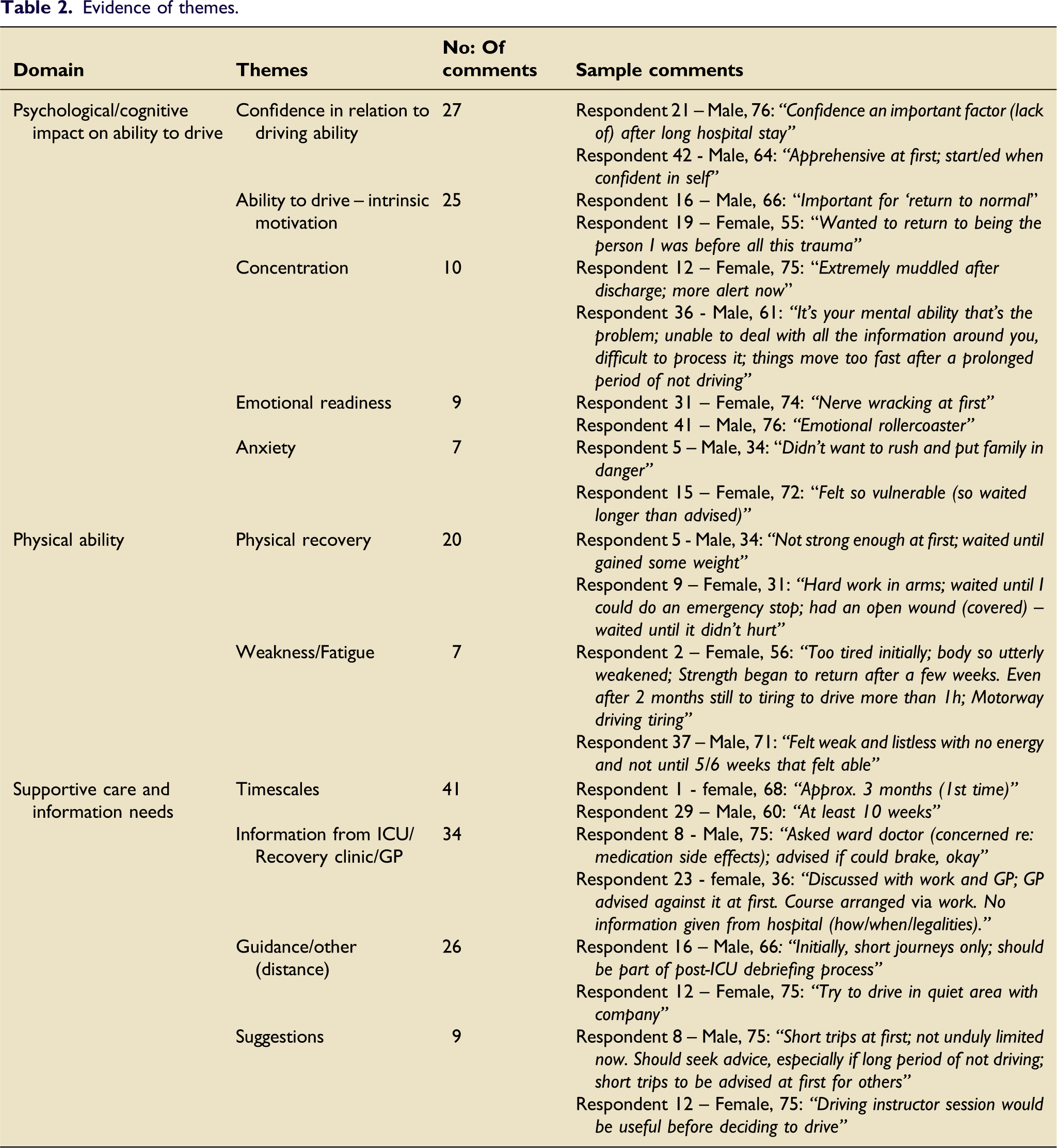
Evidence of themes.
Psychological and cognitive impact on ability to drive
The psychological and cognitive aspects of resuming driving was strongly influenced by confidence, a prominent theme that was raised by many respondents (n = 27). It was reported both negatively and positively, with a lack of confidence an important factor in returning to driving, and on extent of driving. Some respondents, however, reported no issues in returning to driving, Confidence determined how, when, and how much people returned to driving. Various strategies were used to mitigate against this, including having accompanied practice. Some respondents suggested ‘driving buddies’ and with many advocating local drives first. Self-confidence was reported to increase once driving had been attempted. “… started with short trips of less than 1 mile, which gradually got longer. Accompanied practice, a ‘driving buddy’ was useful for confidence” (Respondent 3)
Distinct from confidence, emotional readiness related to respondents reporting being ready to drive again, as opposed to being confident in their ability. They cited confidence and emotions as different, and that emotional problems might be at the root of recovery and ability to drive: “This was an emotional and confidence thing rather than a physical.” (Respondent 41) “I found it a bit stressful at first – but I needed to drive again. But I now get a bit angry at drivers” (Respondent 10)
Intrinsic motivation to drive as part of motivation to resume normal activities with driving a marker of recovery was identified by respondents. “… (driving is) important for ‘returning to normal’” (Respondent 16) “Stubbornness, determination and denial. A desire to get my independence back” (Respondent 23)
Reduced ability to concentrate, feeling muddled and being mentally unprepared, with slower response times and decreased mental alertness were reported. This theme also related to spatial awareness, and one driver reported having a minor accident (described as a ‘scrape’) on their first drive since discharge and directly attributed this to being unable to concentrate post-ICU. Respondents varied in their self-awareness of their mental capacity to drive. “… things move too fast after a long period of not driving” (Respondent 36) “(I needed to) be mentally ready; I can’t do long journeys – am tired and have no concentration” (Respondent 13) “I did a test drive to check spatial awareness etc..” (Respondent 8)
Physical ability
Features of physical ability to drive included: weakness and fatigue, and physical recovery. Individual physical recovery and the ability to perform key driving functions, such as emergency stops, were a determining factor in driving resumption. For some respondents this aspect prevented driving for several months. “I was physically exhausted at first. I had no shoulder or ankle flexibility” (Respondent 23)
Weakness and fatigue were also cited by respondents. “Accompaniment was helpful if I got too tired… (or I was) concerned about fatigue” (Respondent 3)
“A stay in ICU is such a shock, your body is so utterly weakened. When recovering you take one step at a time and meet the challenges. Certainly, driving was not my first concern. . . As a few weeks passed, my strength began to return . . . Even after 2 months I’m still too tired to drive for an hour, especially motorway driving.” (Respondent 2)
The connection with mental and psychological readiness was also outlined: “I wanted to wait until my legs felt strong to use the footbrake in an emergency and my brain was quick to respond” (Respondent 6)
Supportive care and information needs
Sources of information accessed by individuals about driving following critical illness was highly variable. Respondents reported that advice from GPs or medical teams often focused on physical function; ability to undertake an emergency stop was commonly used as a proxy for readiness to drive. This was not always regarded as helpful, with some respondents suggesting a driving test, or some sort of cognitive check prior to driving resumption was needed. Mental and cognitive ability were not interrogated, other than subjective ‘readiness’. “Asked doctor as wanted to be sure; doctor advised it was okay if I could do an emergency stop” (Respondent 9) “No guidance, our doctor said that I should start when I felt ready” (Respondent 16)
Timescales for those who returned to driving varied significantly, with feelings of being ‘ready’ most commonly cited by respondents, thus suggesting this subjective notion of readiness was important for mental preparedness with many respondents articulating that they did not feeling ready to tackle long drives. “(it has) taken 18 months to feel I could drive safely” (Respondent 14) “To begin with I just sat in the car without actually driving, 6 weeks on I’m only driving short distances.” (Respondent 21)
Respondent-generated ideas to assist with driving resumption included driving re-tests, time with driving instructors to build confidence and motorway driving courses. Graded exposure to driving was a recurring theme, with many people initially ‘testing’ their ability to drive safely by undertaking short distance journeys. Clear accessible guidance after critical illness was advocated by respondents.
Discussion
This single centre study elicited the incidence, time-course and experience of driving resumption among 45 adult critical illness survivors who had undergone four or more days of mechanical ventilation in a mixed general UK NHS intensive care. We showed that driving resumption was frequently delayed or not achieved; 32% of driving licence holders had not resumed driving by 3 months following ICU discharge and 16% had not resumed driving by 1 year.
Numerous barriers to driving resumption were cited by respondents. Lack of confidence was a highlighted factor. Respondents in this study often cited accompanied and local drives to rebuild confidence and enable return to driving. Intrinsic motivation was also key. Respondents wished to resume normal activities as soon as possible, with driving being a defining activity in people’s recovery and sense of self-worth. This echoes findings from previous research highlighting the desire to regain independence following critical illness. 12
Ability to perform an emergency stop is not included in any guidance or standards, however from our survey it appears to be used as a proxy by healthcare professionals and patients in determining readiness to resume driving. Only one respondent underwent a return to driving course, but this may be an avenue for survivors to explore to enable safe and timely resumption of this activity.
There is a clinical responsibility too that needs to be considered. As shown in our study, from whom, and how, these survivors gain their information about driving resumption is highly variable. Clinicians need to consider cognition, and especially the executive component of cognition, alongside the patient’s physical function which is often the primary focus. Medications may impair ability to drive. Current DVLA guidance acknowledges there is no single marker of impaired cognitive function relevant to driving and a comprehensive approach to assessment is required. 4 In cases where cognitive ability is difficult to determine, a further neuropsychiatric/psychological assessment may be needed or an in-car, on-road assessment.4,8 Recovery after critical illness clinics provide an suitable forum for return to driving discussions.
An unnecessary delay in driving resumption could impact the mental health of critical illness survivors, further impeding recovery. Isolation and depression have been noted in older adults who have experienced a similar loss of independence.13–16 Commentary from individuals in the public domain describe how in old age the car begins to represent life with feelings of freedom and normality being restored, even if only temporarily. 17 The nature of not being able to drive represents an unwelcome agonising change. 18 Frailty associated with critical care survivorship may mean that individuals of a lower age demographic may entertain similar thoughts and feelings.
Many individuals rely on driving as a means of accessing work and social support, especially in rural areas and communities. Approximately one million people in the UK and over three million people in the US are primarily employed as drivers or are required to drive as part of their job, reflecting the importance of driving after critical illness to the economy as well as individual financial stability.19,20
Driving enables resumption of other important activities alongside work. Critical illness survivors often have on-going health requirements and for ease of access a vehicle is frequently required. Accessing hobbies and leisure pursuits is vital for enhancing quality of life. 21 Driving enables parental and carer responsibilities often required of individuals in this demographic.
To our knowledge this is the first published study to explore the principal themes and metrics specific to driving after critical illness. Limitations of our study include the single-centre methodology which may not reflect the UK-wide or global picture. The qualitative data reflect only written textual responses and was gathered from open-ended questionnaires in a small, self-selected sample, and interviews may have yielded more in-depth data. However, similar studies using textual analysis have still yielded important implications for practice,11,22,23 as in our study. Clinical data about type/severity of critical illness or hospital length of stay following critical illness were not collected, nor was any involvement in trauma related to driving or road traffic accidents. It is recognised that varying lengths of hospital stay may have impacted on the results obtained. The questionnaire was not pilot tested or validated prior to use which would have helped improve design, clarity of the questions and reduced the risk of bias. Data from non-responders would have added insight into this topic and potentially influenced results. Strengths of our study include the high response rate and the wealth of qualitative data ascertained relative to survey length.
Conclusion
Significant time delay to driving resumption and numerous barriers associated with driving resumption were evident within this cohort of critical care survivors. Inconsistency of information received by respondents about driving resumption after critical illness in this study reflects lack of published guidance. Although the deleterious effects of a critical care stay are well documented 24 research about the impact these have on subsequent driving ability is lacking. The balance between avoiding unnecessary delay to driving resumption whilst averting premature return warrants further investigation. Reducing avoidable delay to driving where appropriate should be viewed as a low-cost high impact intervention to enhance health related quality of life. Further research is needed to understand the epidemiology, enablers and barriers to driving in this population.
Footnotes
Availability of data and material
The survey data that support the findings of this study are available from the corresponding author, (CA), upon reasonable request.
Authors contributions
JM, CW, NP and MG were responsible for study conception and design.
CA and JM were responsible for quantitative data analysis and interpretation.
NP and JM were responsible for qualitative data analysis and interpretation.
JM and CA prepared the manuscript.
All authors contributed to manuscript revision and approved the final version for submission.
JM acts as the guarantor for the intellectual integrity of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was confirmed as service improvement that did not require ethical approval
Consent to participate
Informed consent was obtained from all individual respondents included in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.