
Abstract
Background
The Covid-19 pandemic has highlighted weaknesses in the National Health Service critical care provision including both capacity and infrastructure. Traditionally, healthcare workspaces have failed to fully incorporate Human-Centred Design principles resulting in environments that negatively affect the efficacy of task completion, patient safety and staff wellbeing. In the summer of 2020, we received funds for the urgent construction of a Covid-19 secure critical care facility. The aim of this project was to design a pandemic resilient facility centred around both staff and patient requirements and safety, within the available footprint.
Methods
We developed a simulation exercise, underpinned by Human-Centred Design principles, to evaluate intensive care designs through Build Mapping, Tasks Analysis and Qualitative data. Build Mapping involved taping out sections of the design and mocking up with equipment. Task Analysis and qualitative data were collected following task completion.
Results
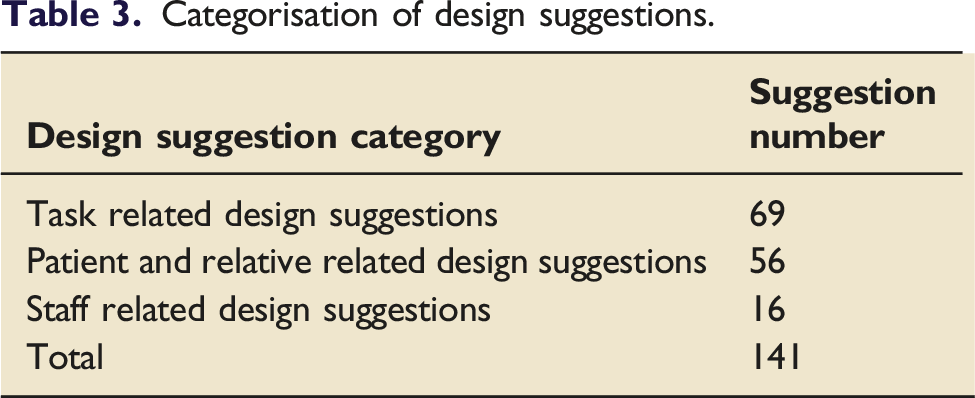
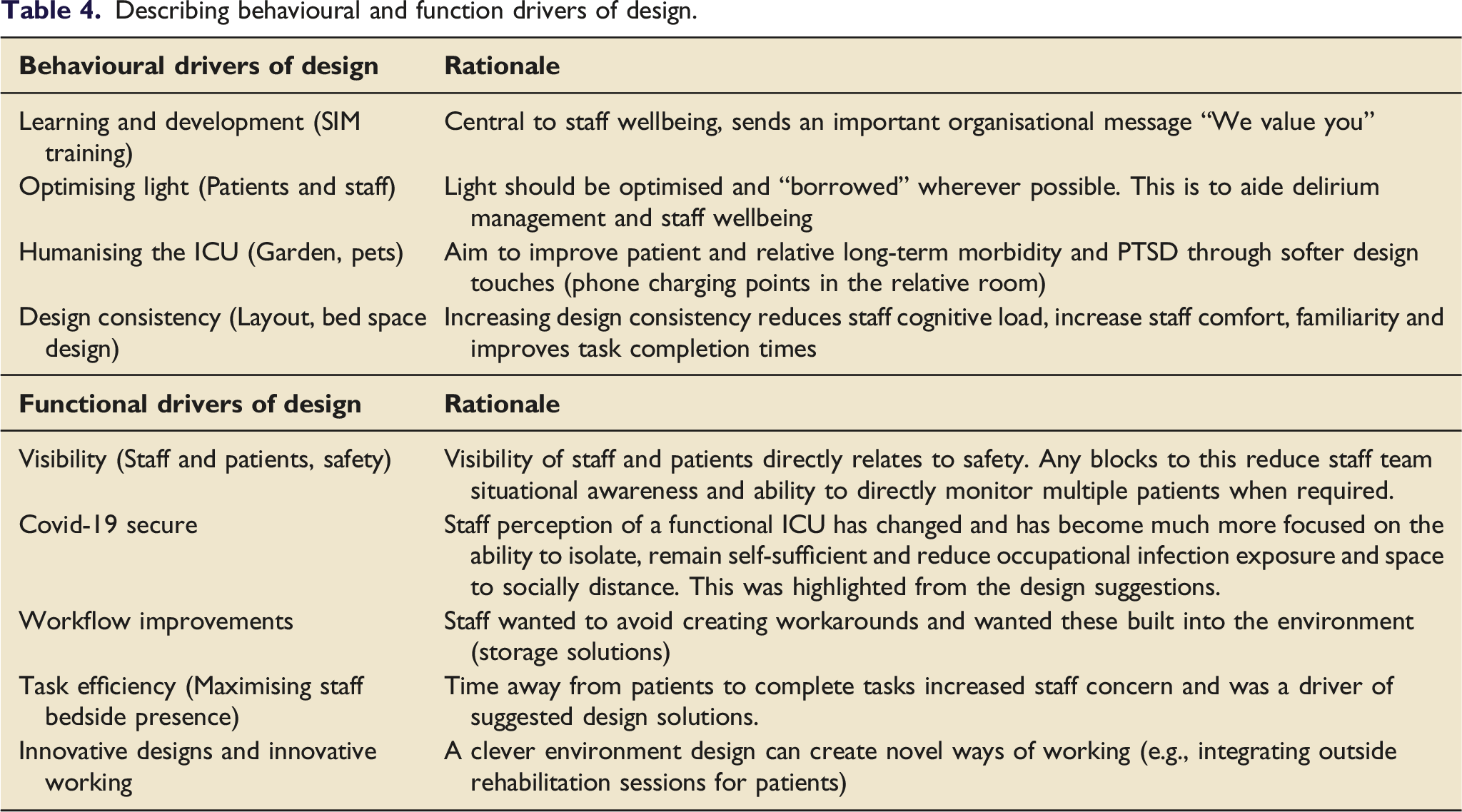
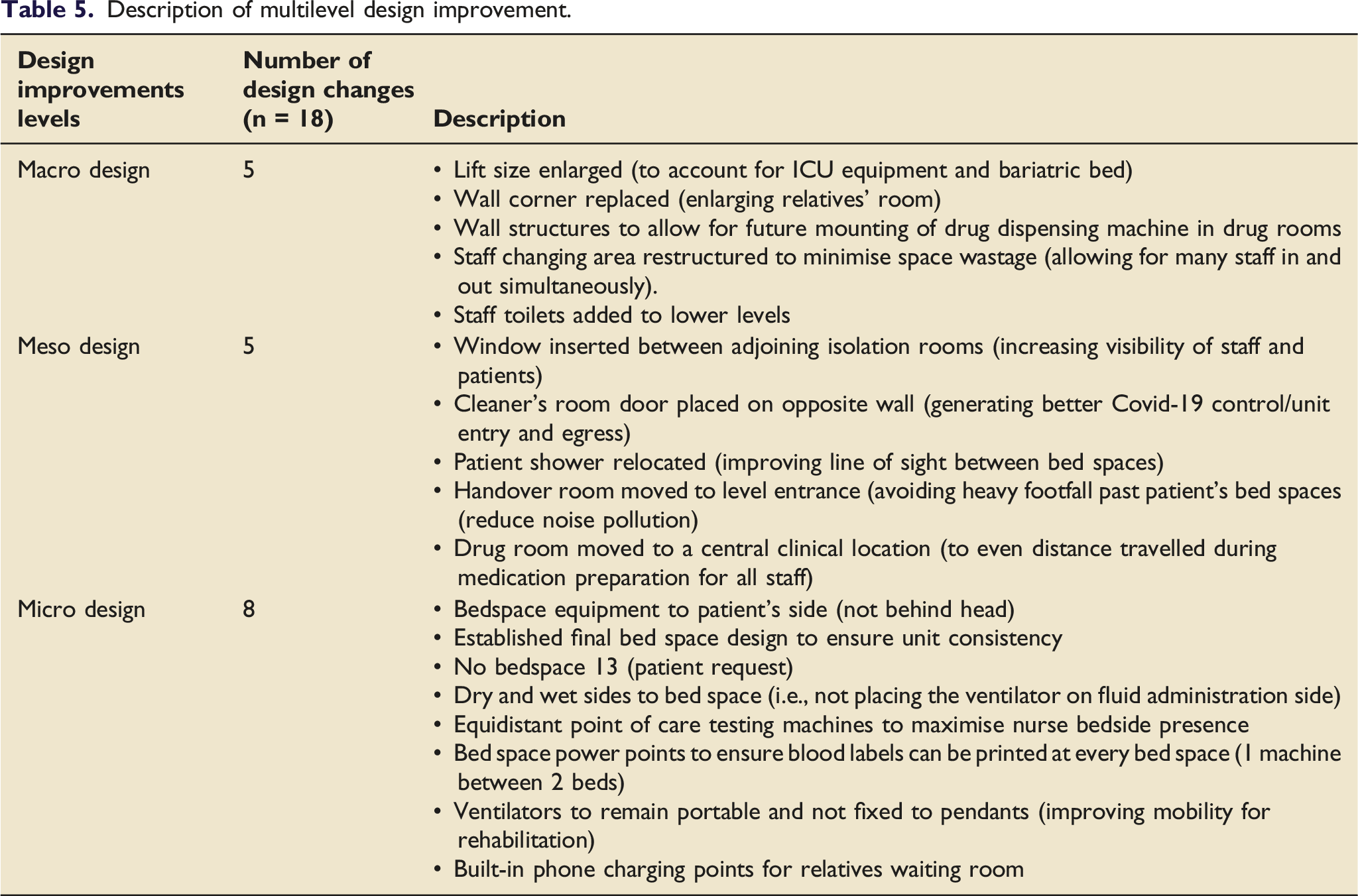
56 participants completed the build simulation exercise generating 141 design suggestions (69 task related, 56 patient and relative related, 16 staff related). Suggestions translated to 18 multilevel design improvements; five significant structural changes (Macro level) including wall moves and lift size change. Minor improvements were made at a Meso and Micro design level. Critical care design drivers identified included functional drivers (visibility, Covid-19 secure environment, workflow, and task efficiency) and behavioural drivers (learning and development, light, humanising intensive care and design consistency).
Conclusion
Success of clinical tasks, infection control, patient safety and staff/patient wellbeing are highly dependent on clinical environments. Primarily, we have improved clinical design by focusing on user requirements. Secondly, we developed a replicable approach to exploring healthcare build plans revealing significant design changes, that may have only been identified once built.
Background
The Covid-19 pandemic has highlighted weaknesses within the current National Health Service critical care provision 1 because of the significant number of patients requiring higher level hospital care. 2 Weaknesses include capacity (supply and demand of beds to staff), lack of flexibility and outdated infrastructure.1,3 Adhering to occupational Infection Prevention Control is challenging with staff repeatedly reporting difficulties in social distancing due to limited clinical space 4 exacerbating staff concerns about occupational virus exposure. 5 Caring for Covid-19 patients is also challenging partly due to infection control issues such as limited number of isolation rooms and waste management systems. Similar environmental and infrastructure problems were common in the United States during the H1N1 pandemic. 6
Even during non-pandemic times, the clinical environment can negatively affect the efficacy of task completion, patient safety 7 and staff wellbeing. 8 Critical care staff often cite hectic and busy environments, distractions and being unable to locate essential equipment 8 causing task completion failure. A human centred approach is one that has traditionally been lacking in clinical workplace designs and workflow issues faced by staff can be directly attributed to this. 10 Human-Centred Design (HCD) principles holds the user central to its design process and actively engages them before, during and after design development. There are four key steps 1. Defining the context of use 2. Specify user requirements 3. Produce design solutions to meet these requirements and 4. Evaluate designs against requirements. In the commercial sector, a functional working environment can increase productivity by 15% and reduce staff sick days. 9 Significant cost and human benefits can be harnessed when designing clinical areas based on requirements of the users themselves. 11
The United Kingdom government has invested in the construction of Covid-19 “secure” Intensive Care Units (ICUs). Our key design aims included reduction in the incidence of nosocomial infections, patient outcomes, staff efficiency and well-being along with a building hard-wired for pandemic resilience. To achieve this we employed a HCD approach. 12
Methods
Aims and objectives
The aim of this work was to create a clinical ICU design centred around staff and patient requirements. To achieve this, we evaluated proposed ICU designs utilising a novel build simulation exercise to elicit user feedback.
Ethics
This work was undertaken as part of a local service improvement initiative Ulysses reference number 6805. This work was fully supported by the Oxford University Hospital NHS Foundation Trust and The University of Oxford. This manuscript has adhered to the Standards for Quality Improvement Reporting Excellence 13 guidelines (Supplementary File 1).
Human-centred design
Underpinning this work are the HCD principles as per the International Standardisation Organisation 9241-210 document. 11 Whilst the principles of HCD are applied to computer systems, it was felt that this would be a valuable and systematic approach to clinical workspace design. A similar approach has been applied in another healthcare design project. 10 To meet the four HCD principles for this specific project (detailed in the introduction), we developed an ICU build simulation exercise that would specify user requirements (point 1 and 2) and produce design solutions to meet these requirements (point 3). This data would underpin the design process as the build project progressed (point 4).
Design team
The design team consisted of a multidisciplinary team group including ICU clinicians, nurses, and Allied Health Professionals, IT representatives and clinical researchers. Design team members and architects provided specialist construction and regulatory insight into a project. Regular design meetings occurred preceding the ICU build simulation exercise with feedback being used to iterate designs.
ICU Build simulation day
The build simulation exercise utilised several methods to elicit user requirements and workflows. Methods employed during this exercise were Build Mapping, Task Analysis and Qualitative data from staff groups/interactions. These approaches allowed an MDT group of users to explore the designs in ways that are not possible using 2D building plans. Plan mock-ups have been cited as key strategies to highlight strengths and weaknesses of clinical designs. 14 Four facilitators moderated the exercise according to a pre-specified agenda. However the approach was not entirely rigid and remained flexible to the participants and their job roles. Two facilitators had in-depth knowledge of the ICU build and design process, one facilitator had experience with human factors methodology and research data collection methods and one facilitator was an ICU physiotherapist.
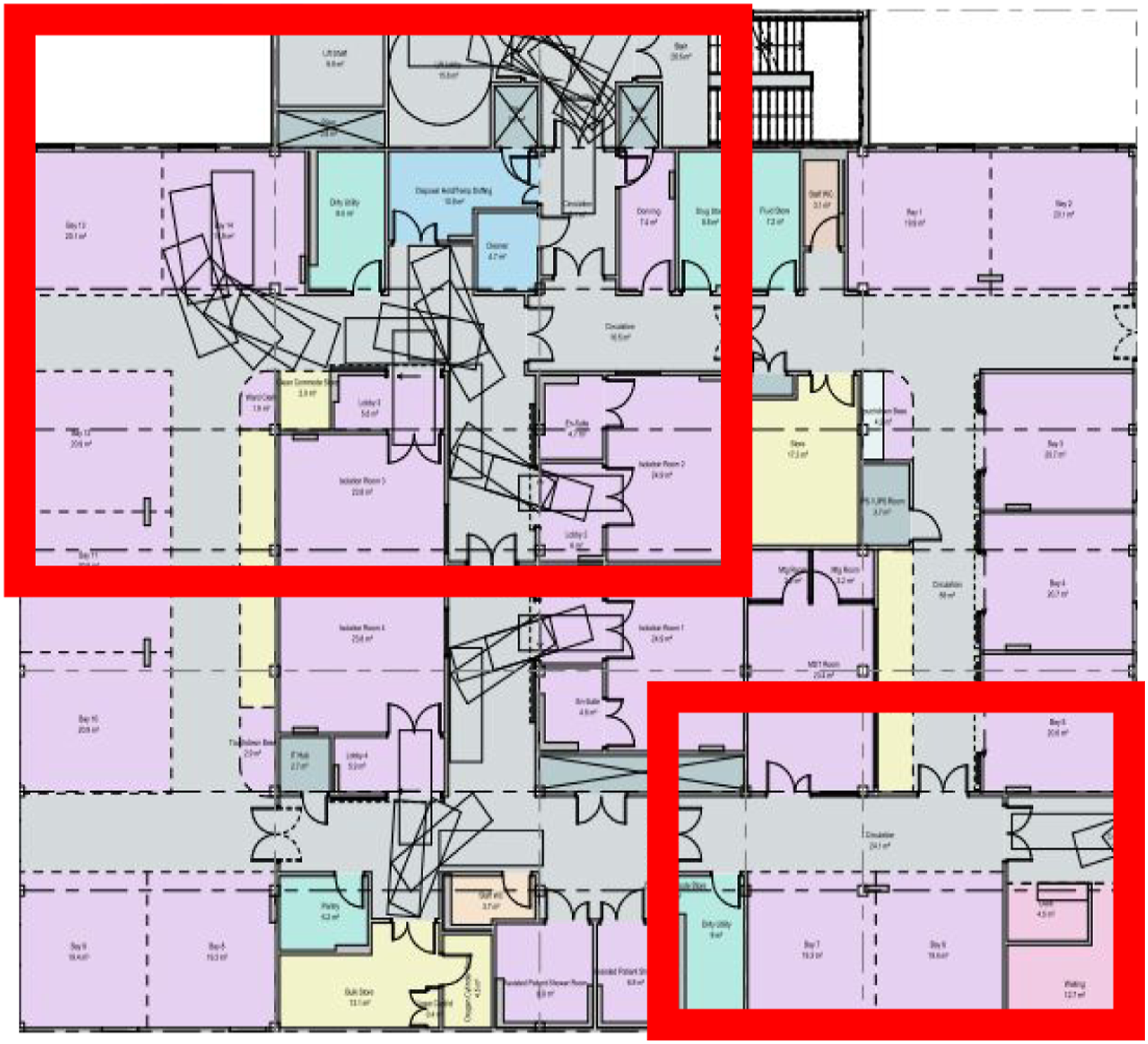
Build mapping
Large sections of the proposed ICU build were mapped to scale using floor tape to outline several key areas (refer to Figure 1). These areas were mocked up using real ICU equipment including beds, ventilators, pumps, chairs, trolleys, and haemofiltration machines to increase the fidelity of the exercise. Given space constraints we were unable to map out entire ICU levels, so we prioritised areas of concern/predictable high activity such as tight corners or lifts (refer to Figure 2). Build Mapping allowed the visual representation of space and ICU orientation prompting staff to consider workflow and day-to-day clinical activities. Mapped areas also provided the opportunity to run predefined task exercises. Mapping of lift sizes. Map of simulated ICU areas.
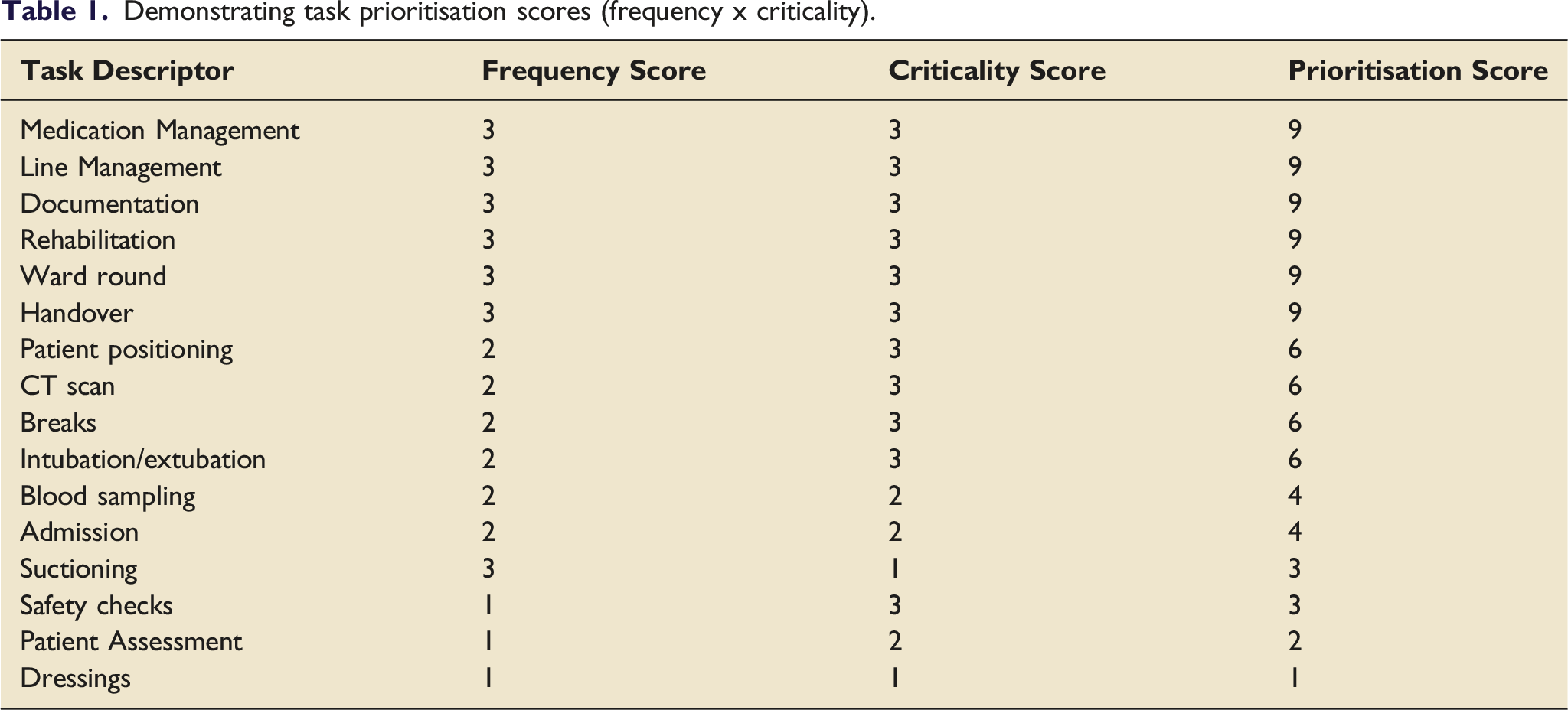
Task analysis
Demonstrating task prioritisation scores (frequency x criticality).
Qualitative data
Qualitative data were captured through facilitator observations and participant feedback during task scenarios. Ad-hoc comments were captured throughout the day. All data was entered into an excel spreadsheet.
Setting
This work was undertaken in a large teaching hospital Trust. The ICU build simulation was held in a large open space within hospital grounds creating an accessible exercise for staff who had clinical commitments.
Participant selection
All potential users of the proposed ICU environment were invited to participate in the build simulation exercise. Participants were a convenience sample of users of the new ICU unit which included staff, patients, and relatives. Importantly, we wanted to capture a range of professions and perspectives on the current designs to identify differing user requirements
14
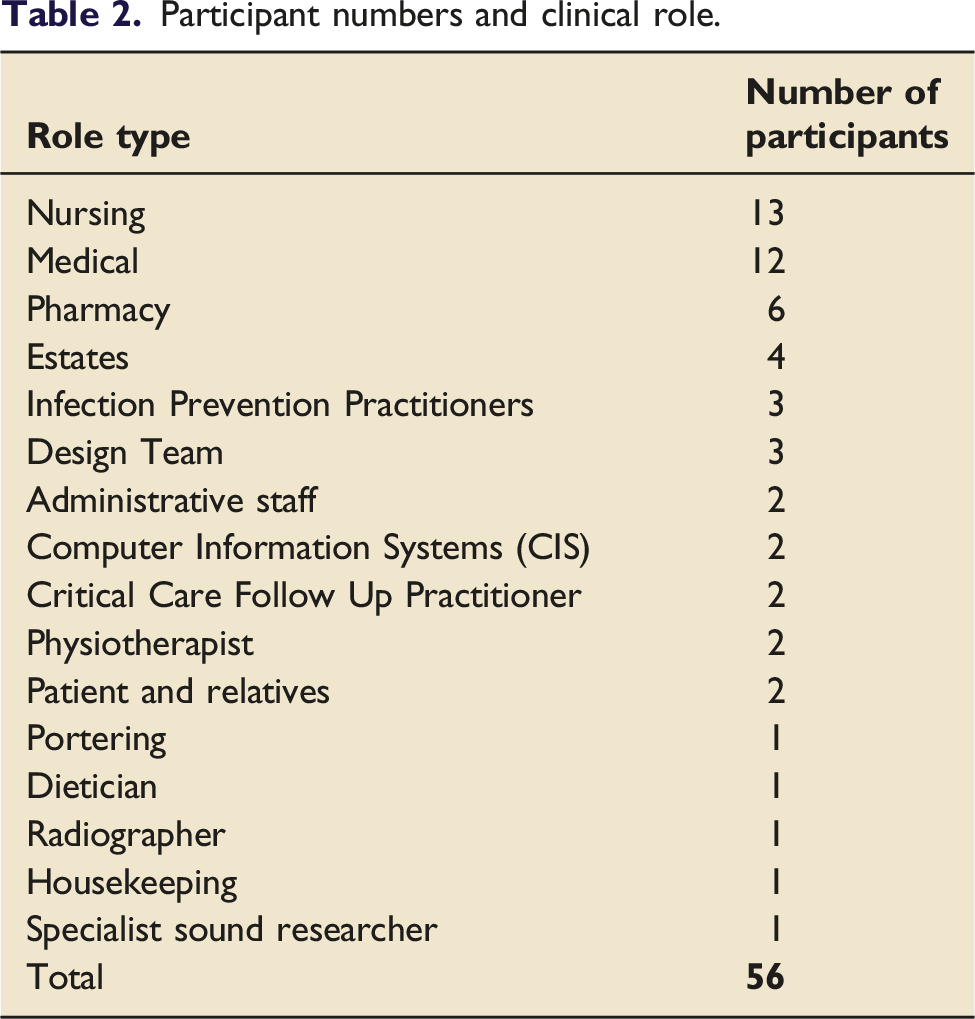
unique to certain staff groups and patients. Critical care generally consists of two user groups requiring representation, a core and transient user group. • Core groups include patients, relatives, nurses, doctors, physiotherapists, dietitians, pharmacists administration, housekeeping, IT specialists • Transient groups include radiographers, porters, engineers, infection prevention teams, visiting specialist clinical teams
Paper concepts and definitions
Design changes vary in significance, difficulty and costliness and occur on many infrastructural levels. To ensure that this was well represented within the data we created a multilevel categorisation system for any design improvements generated from the ICU build simulation exercise. For the purposes of this work, we have defined the design levels presented within the results section: • Macro level design-refers to high cost or structural building changes. • Meso level design- refers to room function changes, insertion of windows or doors • Micro level design- refer to interior design and room layout changes, bedspace design and storage for consumables
Analysis
Data were thematically analysed and sorted. 15 The data was not required for theory generation, but exploratory in describing staff workspace requirements. Some of the qualitative data has been quantified to give a more concise overview of results. Quantifying qualitative data has been utilised in previous studies as a way to understand and present complex qualitative data. 16 To ensure retention of the richness of the qualitative data, narratives informed a design report, providing the foundation of further design meetings. A pragmatic approach was taken to analysis given the required output of the exercise. All facilitators were given access to the results of the day and asked to feedback if any information had been misrepresented. No concerns were raised regarding the credibility 17 of the data.
Results
Demographics
Participant numbers and clinical role.
Design outputs
Categorisation of design suggestions.
Describing behavioural and function drivers of design.
Description of multilevel design improvement.
Discussion
The primary aim of this service improvement project was to create an optimal ICU design based on user requirements underpinned by the principles of HCD. Through this work, we have demonstrated a systematic data collection approach that informed the design of a Covid-19 secure ICU build.
It is not uncommon that clinical areas are designed without fully accounting for clinical workflows 10 or the patient perspective. 18 ICU is widely acknowledged to be a stressful environment, not only because of patient acuity and workload, but also because of design issues such as lighting, high mounted-monitors, power points which cause tangled wires and an excess of noise. 19 We (the design team) made 18 multilevel improvements to the original ICU design by understanding staff workflows, patient/relative/staff requirements and what drives these design requirements using the data from this exercise. Importantly, these requirements (without this exercise) may only have become apparent once the clinical area was in use, drastically limiting possible modifications.
Task focused design suggestions (n = 69) were commonest within the qualitative data. A highly-functional workplace has far reaching effects on individuals (staff and patients) and the organisation. 10 These effects may include better task efficiency, cost saving, allow employees to function at their best 10 and reduce occupational injury. 14 The design team considered the process of patient transfer during the simulation event. Transfer of a critically unwell patient is considered high-risk for adverse events. 20 The frequency at which inter and intra hospital transfers of Covid-19 patients occurs has increased (sometimes labelled as unprecedented numbers) to manage ICU capacity. 21 A significant design change was to increase the size of the lift access to and from the ICU (see Figure 1). This was responsive to a changing patient group, with Covid-19 patients often requiring many more supportive machines and bariatric beds also being in use. A larger lift was able to easily accommodate this patient transfer (which traditional lift sizes would not), thus making the process less logistically challenging for staff during a high-risk situation.
We also considered staff daily workflows 22 during task completion and aimed to maximise nurse bedside presence. Design solutions included equidistant point of care testing, drug rooms, drug preparation areas and label printing machines. Reducing time away from the patient is essential for any future ICU design given the high workload and lower nurse to patient ratios employed during the Covid-19 pandemic. 3 Another overarching functional design driver evident within this data was ensuring that the ICU design was Covid-19 secure: meaning that it was fit for purpose, was able to accommodate both highly infectious patients and “normal” ICU patients and minimised infection risks to both staff and patients. It is estimated that up to 1 in 15 Covid-19 infections are nosocomial. 23 Similarly, staff inability to socially distance is cited as a leading cause of staff-related nosocomial outbreaks. 24 These results indicate that environmental factors contribute to infections partly due to inadequate clinical workplace design. We aimed to mitigate this by increasing staff rest and handover areas where large numbers of staff would be present at any one time. We also improved the unit entry and egress points during the donning and doffing procedure by changing locations of doors to create clean ‘ante-chambers’ if required. The rooms were designed to allow for flexibility in the clinical space and use depending on clinical demand (infectious or non-infectious patients).
Patient and relative design suggestions (n = 56) related to patient wellbeing and humanising the ICU. Historically, the design of critical care units have largely been based on tasks and lost sight of humanisation. 18 Softer design touches from this work fell at a micro design level. Although termed micro, the importance should not be underestimated. This work gave the design team an opportunity to focus the ICU design around patients and staff giving careful thought to lighting solutions, decoration, patient communication, family provision 18 and noise. 25 Specifically, we moved staff communal areas (handover rooms/hubs) to nearer the unit entrance to minimise footfall during shift changeover that would inevitably disturb patients. Similarly, the relative waiting room size was also increased to ensure the ability to safely distance for our visiting families. Bed space design also centred around patient requirements and noise. This included removing all equipment from behind the patient’s head as patient feedback from the exercise showed that unfamiliar noises (collecting aprons, drug preparations) that were out of sight caused great anxiety (see supplementary File 2).
The fewest number of design suggestions related to staff areas (n = 16) demonstrating low staff expectations. Covid-19 has shone a light on the importance of staff care with the expectation that NHS Trusts should provide a clinical environment that facilitates this. 26 Unfortunately, this issue was not as widely highlighted in previous pandemics. 6 Improvements to clinical environments is cited as a strategy that can improve staff wellbeing. 27 A negatively perceived clinical environment can lead to increasing incidence of stress, burnout and poor job satisfaction. 8 All of which directly affect patient safety and satisfaction of hospital care. 28 Despite staff having low expectations themselves, the design team were very much focused on this aspect, paying particular attention to staff areas which would include sleep pods, hot food, cold water fountains and outside space. We also examined the staff changing facilities during this exercise and changed the design of these to ensure that during staff changeover time (high footfall), that many staff were able to enter and exit simultaneously.
Limitations
There are some limitations of this work. Firstly, not all the ICU building was tested as described in the methods. This was limited by event facilities, but we endeavoured to test problematic areas. We were unable to test all the tasks previously identified but again prioritised those that were clinically critical. The data is limited to the user requirements within our local area so these may not be entirely generalisable. However, the design simulation method to obtain requirements is generalisable and useable in other clinical build projects.
Conclusion
We have used HCD methodology to feed into the design process for a modern, bespoke, pandemic resilient ICU build design by focusing on patient and staff requirements and workflows. Our process has engaged all users of this clinical space, creating a co-design and human-centred approach. We have developed and presented a replicable and novel approach to exploring healthcare build projects using simulation and user feedback that may be utilised in similar projects.
Supplemental Material
sj-pdf-1-inc-10.1177_17511437221092685 – Supplemental Material for Building a Covid-19 secure intensive care unit: A human-centred design approach
Supplemental Material, sj-pdf-1-inc-10.1177_17511437221092685 for Building a Covid-19 secure intensive care unit: A human-centred design approachl by Jody Ede, David Garry, Graham Barker, Owen Gustafson, Elizabeth King, Hannah Routley, Christopher Biggs, Cherry Lumley, Lyn Bennett, Stephanie Payne, Andrew Ellis, Clinton Green, Nathan Smith, Laura Vincent, Matthew Holdaway and Peter Watkinson in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_17511437221092685 – Supplemental Material for Building a Covid-19 secure intensive care unit: A human-centred design approach
Supplemental Material, sj-pdf-2-inc-10.1177_17511437221092685 for Building a Covid-19 secure intensive care unit: A human-centred design approachl by Jody Ede, David Garry, Graham Barker, Owen Gustafson, Elizabeth King, Hannah Routley, Christopher Biggs, Cherry Lumley, Lyn Bennett, Stephanie Payne, Andrew Ellis, Clinton Green, Nathan Smith, Laura Vincent, Matthew Holdaway and Peter Watkinson in Journal of the Intensive Care Society
Footnotes
Author contribution
All authors have contributed significantly to the design of the ICU building, data collection and have reviewed and approved this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter Watkinson worked part time for Sensyne Health and has received grant funding from National Institute for Health Research, Wellcome, and Sensyne Health outside the submitted work. All other authors declare no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research Trainees Coordinating Centre, NIHR300509.
Data requests
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.