
Abstract
Anticipated sequelae of critical care admission for COVID-19 disease remain unclear. Our Edinburgh-based critical care follow-up service identified patterns with nerve injury in 13 of 35 patients who attended following a critical care admission between 15/03/2020 and 25/12/2020. This included 7 cases of meralgia parasthetica, 1 brachial plexopathy, 2 common peroneal neuropathies and 3 ulnar neuropathies. All cases of upper limb neuropathy and foot drop occurred in patients in whom prone positioning was used, with meralgia parasthetica occurring additionally in patients who remained supine.
Introduction
Late manifestations of COVID-19 disease and the consequences of treatment are becoming apparent. Our critical care follow-up service observed patients presenting with different patterns of neuropathies.
Methods
All critical care survivors of COVID-19 symptomatic of post-intensive care syndrome received face-to-face review in our critical care follow-up clinic in Edinburgh, UK (additional to physiotherapist review prior to hospital discharge). Patients included were identified retrospectively for a critical care admission precipitated by COVID-19 disease during the period 15/03/2020 to 25/12/2020 and data obtained from electronic patient records. Our local Quality Improvement Team deemed this a service evaluation and ethical approval was not required.
Results
Association of nerve injury with requirements for mechanical ventilation and prone positioning.
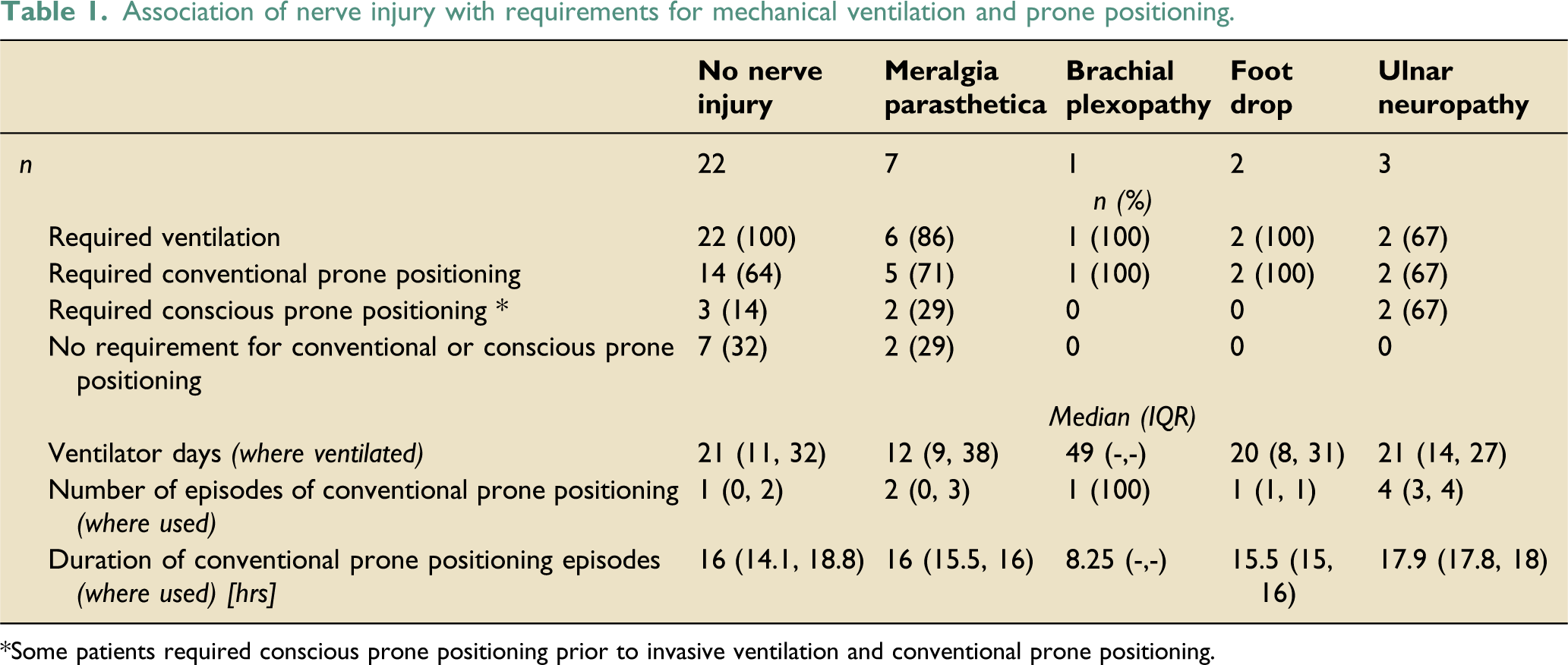
*Some patients required conscious prone positioning prior to invasive ventilation and conventional prone positioning.
Nerve injuries were identified in 13 patients: 7 cases of meralgia parasthetica (MP), 1 brachial plexopathy (BP), 2 common peroneal neuropathies (CPN) and 3 ulnar neuropathies (UN). All cases of upper limb neuropathy and CPN were identifiable prior to hospital discharge but some cases of MP were only identified at clinic review. Median time from ICU discharge to clinic follow up was 135 days (IQR: 94–161 days).
The most serious injuries of BP, CPN and UN universally occurred in patients in whom prone positioning was used (either conventional or conscious). Two (29%) cases of MP occurred in patients who remained supine. The number and duration of episodes in the prone position were uniform and within a narrow range. The number of ventilator days for the patient with BP was notably longer (49 days).
Discussion
We observed a high number of nerve injuries in patients admitted for COVID-19 disease, with more significant injury occurring where prone positioning was used. International consensus guidelines recommend the ‘swimmer position’1-3 for safe prone positioning of ventilated patients. The upper limb movements required can lead to neuropathy from traction and compression, and asymmetrical pressure distribution at the pelvis or knee may cause lower limb nerve compression against bony prominences.
We recognise that nerve injury is rarely commented on in studies related to critical care follow-up and the true incidence remains unknown. Notably, large studies of prone positioning such as the PROSEVA trial 4 do not list nerve injury when reporting on complications. This may be because it is difficult to differentiate nerve injury from critical care weakness early on; however, we found all upper limb and common peroneal nerve injuries identifiable prior to hospital discharge.
We recognise the limitations of this evaluation, most significantly the risk of selection bias from those who were screened and triaged as asymptomatic by telephone consultation and consequently did not attend a face-to-face clinic review. Establishing causality is beyond its scope but several scenarios could be plausible.
The volume of patients presenting contemporaneously may simply have allowed identification of injury patterns that were previously unrecognised, or the risk of nerve injury where prone positioning was used could have been increased due to poor technique by staff new to critical care and experienced staff dealing with an unprecedented volume of patients.
Alternatively, this cohort may be inherently at higher risk of nerve injury, either due to the prevalence of comorbidities such as diabetes mellitus, or an independent mechanism related to infection with the SARS-CoV-2 virus. Further work would be required to attempt to answer this question.
Conclusion
Nerve injury occurred frequently in our cohort with more significant injury observed in those in whom prone positioning was used. Careful technique when positioning patients prone remains extremely important.
Early differentiation of specific nerve injuries in patients recovering from critical illness can be challenging. Reassuringly, severe cases appear likely to be diagnosed during hospital admission; however, patients with less severe injury are at risk of discharge to primary care undiagnosed and untreated. We suggest nerve injury should be actively screened for during recovery, and our experience supports the role of face-to-face follow-up clinics in identifying complications of critical care. It is vital that critical care rehabilitation and follow-up services receive adequate resourcing beyond the pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.