
Abstract
Background
Peer support groups reduce psychological morbidity and increase social support for Intensive Care Unit (ICU) survivors. Group formats differ and research, although emerging, is limited. This study explores a continuously running ICU Expert by Experience group, which has a dual role of support and service-user consultative, from attendees’ perspectives.
Methods
A thematic analysis was conducted on interviews with current and past members of an ICU Expert by Experience group. 11 participants took part in online and telephone interviews. Three provided written responses. Final themes were created following a process of data validation with participants.
Results
Four main themes emerged: (1) Support in the difficult recovery journey (2) Relationships and shared experiences (3) Value of professional facilitation (4) Practical considerations.
Conclusion
Patients highlighted the help gained from the group as an integral part of their recovery journey. Results also identified practical implications for those considering setting up similar support groups.
Introduction
Recovery post-Intensive Care Unit (ICU) admission can involve a process of sense-making. 1 Difficulties around understanding ICU experiences may lead to higher emotional distress. 2 Patients often desire interaction with other ICU survivors to understand whether their experiences are normative. 3 Peer-support programmes reduce psychological morbidity and increase levels of social support for ICU survivors 4 ; therefore, can be effective low-cost interventions. 5 However, post-ICU peer groups are not universally available, 6 fall into a range of models, 7 and the evidence base is limited. 4
Experts by experience providing peer support is well established in a variety of settings. 8 There are six general models of ICU peer support: community based, psychologist-led outpatient, models-based within ICU follow-up clinics, online, groups based within ICU, and peer mentor models. 7 Peer support groups offer a forum to share experiences, a means to better understand experiences, and opportunity for reciprocity in giving and receiving support. 9
The Covid-19 pandemic is influencing the development of critical care services, including peer support groups, with nearly half of responders to a recent UK survey offering peer support. 10 Consequentially, it is important to collect and disseminate quantitative and qualitative feedback from participants 9 because research, including experiential insights, is integral to the development of related guidelines. 10 This study explores participants’ views of an ‘Experts by Experience’ (EBE) group established in 2018 as part of a hospital in the South West of the UK’s ICU follow up service. This service evaluation aims to understand how participants experience the group, its format and outcomes using in-depth qualitative data.
Methods
The group is facilitated by a critical care psychologist, supported by a critical care rehabilitation nurse, and serves as both a support and service-user consultative group. Prior to Covid-19, the group ran monthly in-person for 2 hours but transitioned to online fortnightly for 1 hour. Psychological screening questionnaires, which include an opt-in to attend the ICU follow-up clinic, are sent 3 months post-discharge to ICU survivors with a 4 day or longer ICU admission. Those who score for psychological distress, but do not opt-in are offered a critical care psychology assessment. Group recruitment is from those attending the follow-up clinic or assessment appointment, and most group members have engaged in therapy for ICU-related distress with the unit’s critical care psychologist.
A research team consisting of a trainee clinical psychologist and three psychology assistants who were not involved in facilitating the group was established with the aim of completing a qualitative investigation of current and previous participants’ experience of the group. Members of the research team attended a EBE group meeting to introduce the research and seek group participants willing to attend a separate consultation session to shape the recruitment process, methods, and interview schedule (Figure 1). The evaluation was approved by the hospital’s Audit, Assurance and Effectiveness Team. Letters, emails, and an information sheet were sent to anyone who had attended the group. Potential participants, including those involved in the consultation process, were asked to contact the research team. Participants provided written consent. Participants were given the option to attend a semi-structured interview online or by telephone or be sent the interview schedule to provide a written response. Semi structured interview schedule.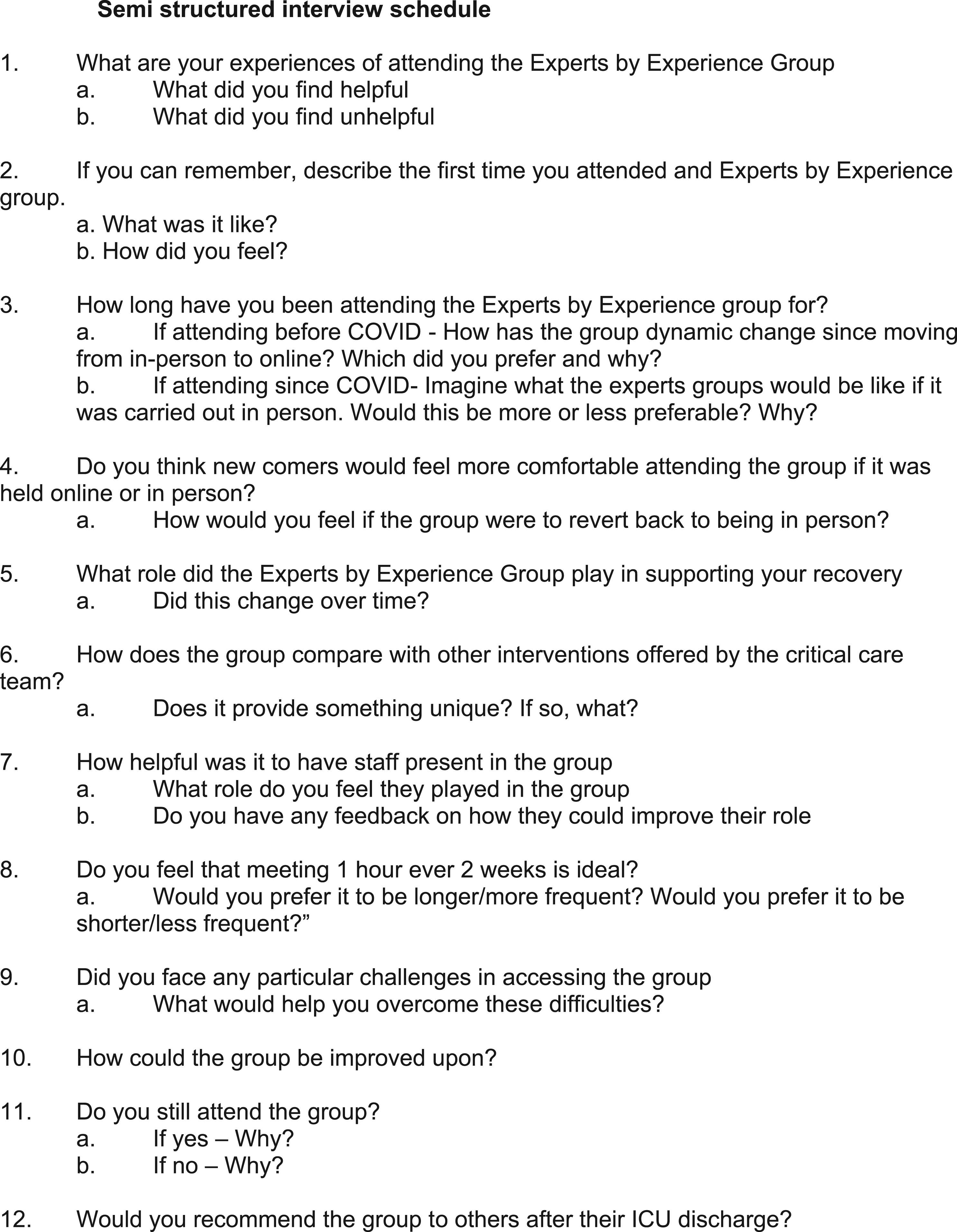
Two researchers conducted interviews, which were audio recorded, transcribed and pseudonymised. Postal questionnaires data was extracted and pseudonymised. Recruitment was terminated following data saturation, where no new themes emerged.
Data analysis
Thematic analysis 11 was used to analyse the data using NVivo software. Data was read for familiarisation. Two researchers not involved in the interviews undertook first and second order coding for separate halves of the data, then compared key concepts and coding schemas from the independent analyses, exploring similarities and differences, to jointly develop emergent themes across all data. One of the researchers involved in the analysis shared emergent themes in two hour-long group meetings with participants, to consult on the themes, before final themes were confirmed. This served to maintain validity and fidelity to the experiences of people attending the EBE group.
Results
Participants
11 participants took part in interviews (seven female and four male) and three completed postal questionnaires. Participants were 33–73 years old, with a mean age of 53. Interview duration ranged between 19-81 min (Mean duration = 37 min). Members of the EBE group tend to have longer ICU stays. 1 The participants in this study had ICU stays ranging 11–39 days with a mean of 19 days. Nine participants were current and five past members of the EBE group.
Four themes arose from the analysis. Quotes are from the data and names are pseudonyms.
Theme 1: Support in the difficult recovery journey
Participants described difficult recovery journeys following ICU care, with numerous challenges, which tended to be expressed as difficulties in recovery post-ICU discharge as opposed to inpatient admission. Phoebe described: ‘I always thought once somebody has been poorly in intensive care, they come out of it, phew, everything's okay. But actually that is when the problems start’. Some spoke of a changed sense of self, Kim said ‘I’m only just now finding (Kim) back, she’s been lost since the coma’.
Sam described the group as ‘a very valuable recovery tool.’ Participants felt the group provided something unique, Harry shared: ‘I don’t think there is an alternative to the group.’ All would recommend the group to other ICU survivors. Although not directly asked by the researchers some participants highlighted the importance of considering an individual’s psychological needs before attending due to the risk of retriggering traumatic experiences, as Blake noted: ‘I had PTSD… I was walking around like a headless chicken because I didn't know that I had it. So, I would suggest a potential issue… is that people may wish to come to the meetings… a bit too early.’ Participants who had left the group reflected on how their psychological recovery supported them to transition out of the group, Steven shared: ‘My PTSD had disappeared… and I was happy with the fact that it’d become a distant memory, maybe it [was] time for me to leave the group.’
Theme 2: Developing meaningful relationships and sharing experiences
Developing meaningful relationships and sharing experiences appeared in every interview. A confidential space felt essential for members. Michelle said: ‘Having that space to reflect and it being a safe space… there's no judgment from others.’ Comradeship was conducive to improved emotional wellbeing, with Phoebe stating: ‘You get stronger… you feel accepted with them, you feel happy with that little group.’ For some it was difficult to join the group. Sally said ‘my initial experience was, it was horrible. I hated it. But now I think it's brilliant’.
Participants frequently mentioned feeling isolated post-ICU discharge, finding it hard to talk to friends or family about their experiences. Rohan shared: ‘It's hard to sort of convey what you've been through to people who haven't really been through a similar type of trauma. Being in a group of similar-minded people is beneficial’. All participants valued the space to communicate with others who had been critically ill, as explained by Sarah: ‘Finding out that… it wasn't just me and that… most of us in the group all felt the same… that's the important thing for me… it just makes people realise they're not on their own.’ While members expressed similarities in experiences, some noticed differences, particularly around reasons for ICU admission, Jack said ‘what you've got to remember, it's different for everyone. You know, I joined it because of my experiences with COVID-19’.
Theme 3: Value of Staff facilitation
All participants spoke positively about facilitation and involvement of ICU-linked staff. Sarah describes the role of their input: ‘When we still don't understand… they can answer those questions… if you've got [the nurse] there, she could have the answer to that. [The psychologist] has usually got the answer to what's going on in here [points to head] … so that works really well.’ It was acknowledged that the flexible structure of the group was feasible due to skilled facilitation. Mark noted: ‘[The group] is very effective. The manner in which it's organised… that’s probably down to the psychologist; she's… a very, very good communicator.’ Skilled facilitation also provided a sense of containment, as Phoebe stated: ‘If somebody sort of has a bit of a rant then that's not really related to what the group is about, [the psychologist is] very good at pulling people sort of back on track.’
11 participants said that they would like wider ICU staff members to sporadically attend the group. Aimee shared: ‘It would open up a few other avenues really, because the group is very much… focused on psychological wellbeing, but thinking sort of holistically, obviously recovery is not just about the psychological part. It's about all the other parts’. Participants spoke about appreciating access to more information from staff about their ICU stay to fill informational gaps. Andy explained: ‘I actually find it quite nice to meet the people who potentially were looking after me… I just look at their faces and just see if anything jogs my memory’. Steven suggests that the group may be mutually beneficial for staff and group members. ‘It would be helpful for nurses from ICU… to come and see how we're all evolving and striving to repair ourselves.’
Theme 4: Practical considerations
Participants highlighted the advantages and disadvantages of the group being in-person or online. Generally, participants preferred to attend the group in-person but also found the online group acceptable. David elaborated: ‘I’d rather be being in person… you can connect easier physically seeing someone… but… for argument's sake, [if] I was unable to attend because I broke my foot, I'd be quite happy to go online.’ Seven participants spoke about the ease of accessing the group online, with three saying they preferred the online group due to lifestyle factors. Phoebe explained: ‘Sometimes there is an assumption that the people who come to this group are retired or sort of not in employment…. Personally… when it does go back to being in-person, I probably won’t be able to go more than every couple of months or so.’ Some suggested a mixture of online and in-person as the most beneficial, particularly for those attending for the first session. Tessa commented: ‘To go into [the group for the first time] is quite scary… maybe having that virtual session just to get an overview of what it's going to be like, I think is good’.
Suggestions of ideal group frequency varied according to respondents. Harry remarked: ‘It’s got to be every week really… especially with people that are on their own’ suggesting that participants who had less social support and more free time preferred longer and more frequent meetings. Conversely, some participants were comfortable with the meetings being less frequent, as Mark stated: ‘Biweekly is probably about right, but I think for others it might be too frequent… it depends where you are in your recovery.’ This highlights the varying needs of individual as they move along their recovery journey.
All participants shared that they were content with the flexible structure of the group. The group has no formal agenda. Nine participants liked this as it provides space for members to mould the session. Sarah described: ‘Not having an agenda is good in a way, because it sort of opens the floor for whatever may be going on at the time for each person’. Some emphasised the importance of still having a level of structure to ensure the group fulfils its role and to prevent it going off-topic. As summarised by Michelle: ‘Don't rule out having an agenda - but don't make it rigid.’
The perceived role of the group differed between participants, some maintained that it was a consultation group while others felt it was a support group. There were differing perceptions on what the focus of the group should be. Sally mentioned “It seems to me it’s becoming more of a support group than the group who were feeding experiences into the system…it’s to make a difference for those who come next and rather than use it for a support group because you're not feeling well’; whilst Fred said, ‘it's really important to keep the expert group as a support group for ICU survivors.’ Some participants mentioned wanting more clarity around the purpose of the group.
A review of the group’s attendance data indicates the average attendance per session is 10 people. Attendance at the group is not time limited. Clinical experience is that members leave once their ICU related experiences feel more integrated and in the past. Interestingly this process has enabled group attendance to remain around 10–12. Participants expressed general satisfaction with the group size. Six participants suggested that larger group sizes would have a negative effect, with Phoebe speculating: ‘Some people wouldn't get a chance to talk that often… especially if they needed to… get things off their chest.’ Additionally, Mark noted ’It's about 10 to 12 people there. It seems a decent number… if you were to double that number; I think it would lose the dynamism.’
Discussion
The service evaluation explores participants’ experiences of an ICU Experts by Experience group. Four themes emergence from the data: support in the difficult recovery journey; developing meaningful relationships and sharing experiences. value of staff facilitation; and practical considerations. There was unity in the recognition of complex recovery journeys and the importance of meaningful relationships to share these experiences. This evaluation provides additional depth to emerging evidence of post-ICU support groups potentially reducing psychological morbidity and improving social support . 12 This is particularly pertinent as the group’s patient population experienced high psychological morbidities following critical illness.
The risk factors for post ICU psychological distress include a previous history of anxiety or depression.
13
Some participants describe a changed sense of self following critical illness, an aspect often discussed in the group. Many participants have completed trauma focused therapy, so it is possible that re-experiencing symptoms have reduced but a sense of a different relationship with their body remains. PTSD can result in a sense of permanent negative change.
14
Potentially post-ICU support groups facilitate post-traumatic growth whereby psychological struggle following adversity can lead to positive growth.
15
There is a requirement to provide integrated physical and mental health services.
16
NICE
17
recommends stepped models of care (Figure 2), which may be appropriate to conceptualise critical care psychology services. The EBE group sits at step 3, for those with more complex needs, whilst groups offering time limited interventions focused on psychoeducation sit at step 1 or 2. Stepped-care model: a combined summary for common mental health disorders.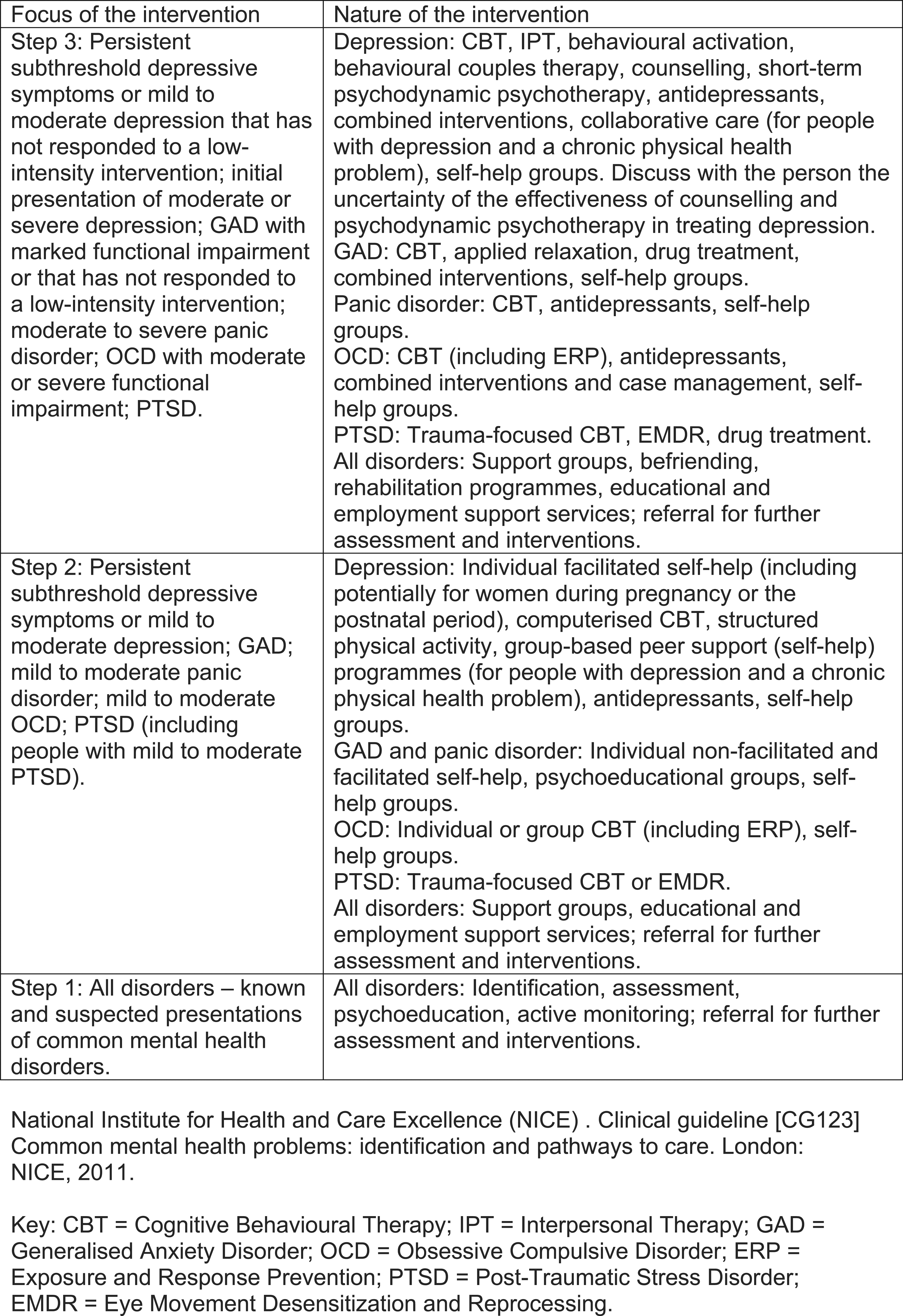
Coivd-19 ICU survivors are mentioned in the data. There has been discussion around establishing a separate group. Options were limited by resourcing but discussion in the group suggest that it has been helpful for Covid-19 survivors to recognise the impact of other critical illness to normalise their own experiences. The population of the group evolves so a significant proportion of the current group members are Coivd-19 ICU survivors.
The EBE group provides intervention aligned with the Social Support Needs Framework18,19 which highlights support in four domains: Informational, Emotional, Appraisal and Instrumental. Through the EBE group ICU survivors make sense of their informational needs via sharing information with other patients and ward-linked staff. Emotional needs are met through the development of meaningful relationships as they adapt to community-based recovery. The EBE group provides the ability to share goals and progress, to bolster emotional support, and to meet appraisal needs through ICU-based staff and other survivors; therefore, contextualising experiences.
The themes of supporting recovery and developing relationships to share experiences indicate the processes involved, whilst those of staff facilitation and practical consideration reflect the group tasks. Peer support includes acceptance, respect, reciprocity, mutual responsibly, trust and integrity 9 and allows ICU survivors care debriefing, sharing experiences and altruism. 20 Attendees appreciate the group’s minimal structure; where skilled facilitation sets group boundaries, creates group safety, and allows flexibility to determine content. Wider research supports the notion that groups are more effective and safer when run by skilled and trained facilitators 21-23 and are effective in supporting those living with mental health difficulties. 24
The facilitation of ICU peer support groups requires the fostering of collaborative relationships between participants; therefore, cofacilitation can help manage the challenges of responding to what can often be quite intense emotions. 9 However, at times due to the pressures created by Covid-19, the group was facilitated by one person. The results indicate that attendance of ICU-based staff is important, potentially for both participants and staff. The outcomes for peer support groups could exist across a broad range of dimensions including traumatic growth, a space where themes emerge which facilitate care improvements and improvement of critical care staff morale. 9
Limitations
This study reports the subjective experience of participants recruited from one peer support group. Although efforts were made to recruit anyone who had attended, it is possible those who had a negative experience may not have wished to be involved. Further research is needed to ascertain effective post-ICU group formats, the range of potential outcomes and underlying mechanisms.
Implications for practice
The implications for local practice included greater clarity around the role of the group. The results touch on the sense that group members have different social support needs. A group email invitation is sent, to which a sentence has been added stating “the function of the group is to provide a safe and supportive reflective space to discuss the impact of critical illness and to contribute to the development of services for ICU patients”. Group members are now invited to send agenda items. The frequency and online format continues. A recent increase in ICU Rehabilitation staffing has enabled involvement of a broader range of ICU-based staff.
Practical considerations to starting a group include group size, purpose, structure, frequency, and duration. 9 It is unlikely that one model fits all; however, a flexible structure with skilled moderation allows adaptation to a variety of needs. Intensive care survivors support needs change as they transition through their recovery process. 19 Peer support groups containing a mix of people at different points in the journey can potentially match needs and support.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.