
Abstract
The development of facial pressure injury (PI) during prone position is frequently described. During the COVID-19 pandemic, the number of patients with facial PIs increased. This quality improvement project describes the effectiveness of using silicone adhesive multilayer foams for preventing facial PIs in COVID-19 patients in need of prone position therapy. After introduction of foam dressing on chin and forehead to the standard protocol procedures for PI prevention, the decrease in number of patients developing facial PIs was statistically significant. Based on these results, the use of silicone adhesive multilayer foam will be implemented as a standard procedure for facial PIs prevention.
Introduction
Facial pressure injuries (PI) are common in patients with acute respiratory distress syndrome (ARDS) in need of prone position therapy.1,2 In our institution, the standard protocol for facial PI prevention for patients in prone position is to position the face in a disposable polyurethane foam prone head positioner with minimal head turning every 1 to 2 hours. However, during the first and second wave of the COVID-19 pandemic in Germany, we recognized a surge of facial PIs in prone positioned COVID-19 patients. Based on the result of a non-clinical study, case reports and expert recommendations,3–6 we changed our PI prevention management. In addition to the standard protocol, we started to use silicone adhesive multilayer foam (Mepilex® border flex) for preventing PIs at chin and forehead (Figure 1) beginning from 01/2021 at one of our ICUs. To evaluate the effectiveness of the new prevention management on PI development at chin and forehead, we performed a retrospective patient chart analysis. Illustration of how to apply silicone adhesive multilayer foams to a patient’s face.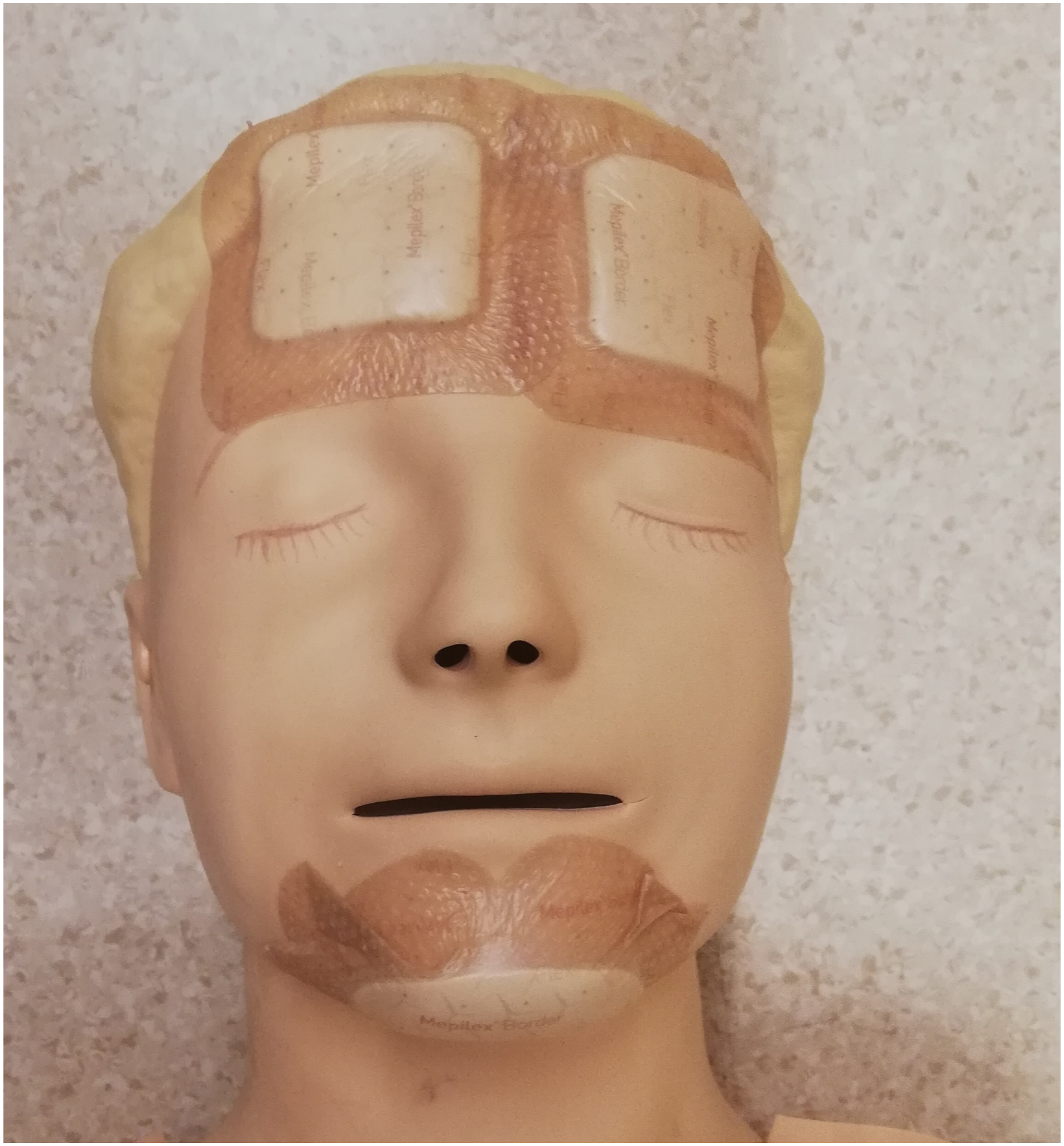
Method
All patients with COVID-19 and with mild to severe ARDS, admitted to the specific ICU until 05/2021 and with at least one documented pronation cycle were included in this retrospective chart analysis. Patients were excluded if they were transferred from other ICUs of our institution because some of the ICUs started also using foam dressing for preventing PIs which could be seen as a bias in our analysis.
The following data were extracted: age, gender, BMI, number of pronation cycles and total time of prone position, ARDS severity and number of PIs on chin and/or forehead.
Data are displayed as mean and standard deviation or number and percentage based on scale measure. Differences between groups were analysed using t-test or chi-square test.
Results
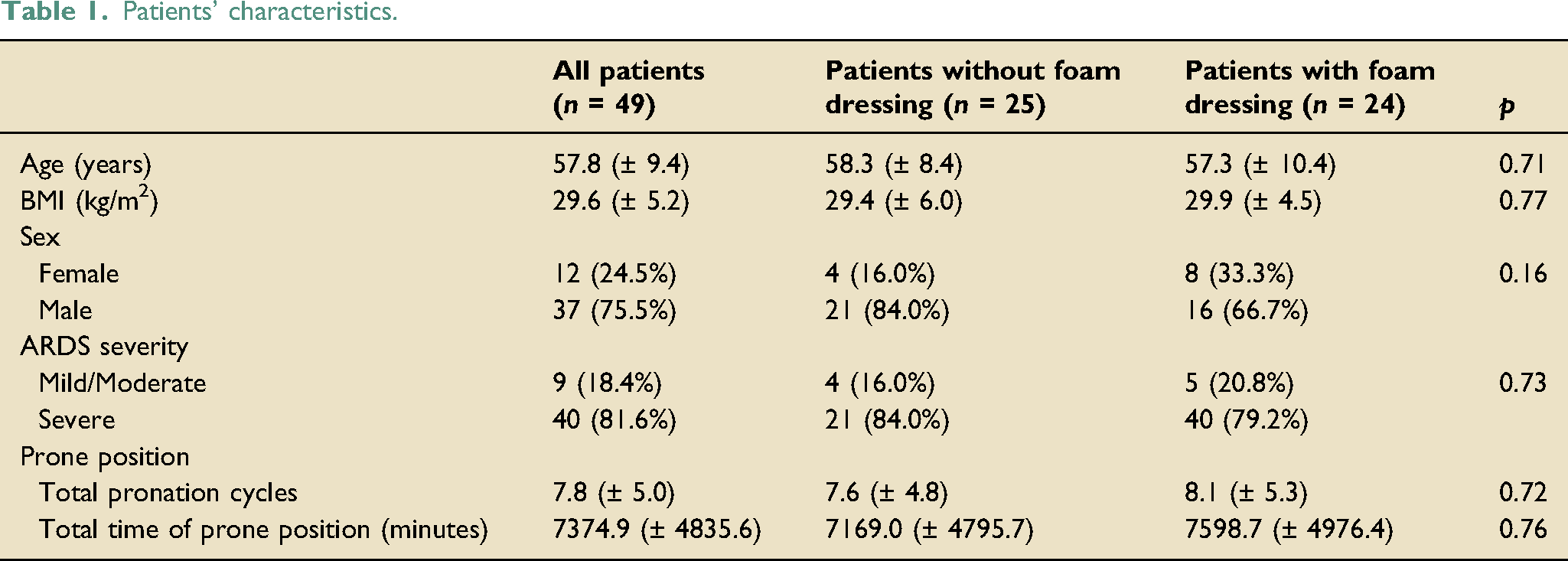
Patients’ characteristics.
Overall, 23 out of 49 patients (46.9%) developed a PI at the chin and/or forehead. In the group where a silicone adhesive multilayer foam was not used (no-foam group), 17 out of 25 patients (68.0%) developed a PI; in the group where a foam dressing was applied (foam group), 6 out of 24 patients (25.0%) developed a PI (p = 0.003). Differences could be observed in developing chin or forehead PIs. Eleven out of 25 patients (44.0%) in the no-foam group developed a PI at the forehead compared to five out of 24 patients (20.8%) in the foam group (p = 0.84). Statistically significant differences could be observed regarding the development of PIs at the chin. Eleven out of 25 patients (44.0%) in the no-foam group developed a PI compared to 4 out of 24 patients (16.7%) in the foam group (p = 0.038) (Figure 2). Distribution of pressure injuries at different body areas using and not using multilayer foam dressings.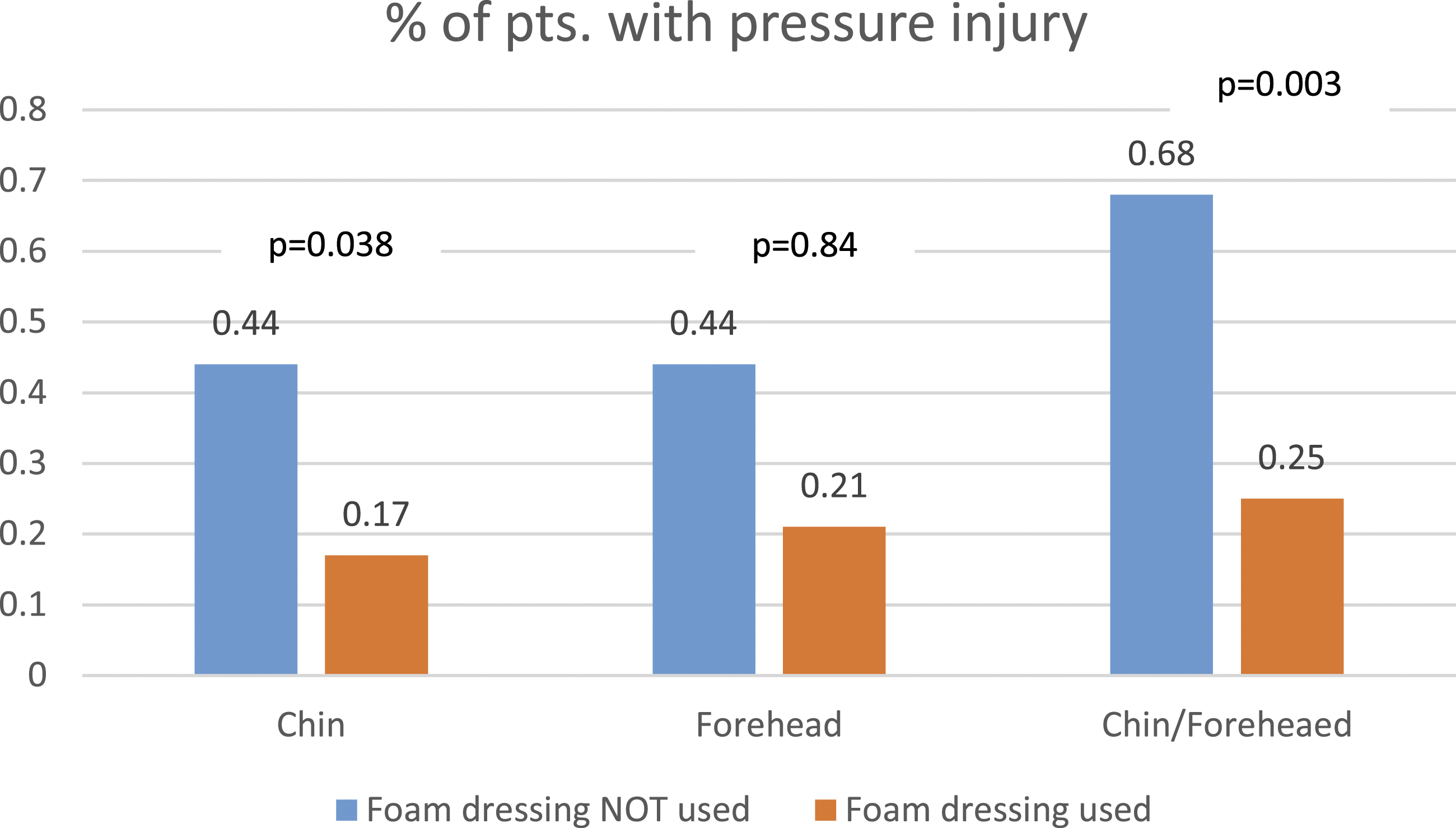
Discussion
Our retrospective patient chart analysis revealed a statistically significant reduction in the development of PIs at chin and/or forehead after applying a silicone adhesive multilayer foam dressing on chin and forehead during prone position. Our results are in line with those of other studies and case reports.5,6
According to Peko and colleagues, silicone adhesive multilayer foam dressings are able to prevent the development of PI due to cushioning the skin area at risk, absorbing shear loads within the dressing and alleviating the bodyweight loads. 3 These foam dressings have also been applied to other body areas, for example, the sacral region or the heels, and have shown protective effects in the development of PIs.7,8
Even though a multilayer foam dressing seems to be able to prevent PIs in the facial region, other influencing factors on PI development should be carefully considered when turning the patient in prone position. Some of these factors are not influenceable (e.g. the amount of vasopressive drugs) but those that could be influenced should be subject of permanent quality control. For example, some clinical experts recommend that turning the patient should be executed by trained staff only and that the head should be turned on a regular basis.2,9 Both measures could be trained and improved.
Preventing PIs in prone-positioned patients is a great challenge and should be a subject of further research.
Conclusion
Applying silicone adhesive multilayer foam dressings on facial skin areas at risk for developing PIs seems to be a feasible and effective measure for PI prevention in COVID-19 patients with ARDS and with the need of prone position therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.