
Abstract
Little is known about the impact of proning on oxygenation and ventilatory efficiency on patients with severe Covid-19. In this retrospective observational study we calculated Pa/FiO2 ratio (P/F) as a marker of oxygenation and dead space fraction (Vd/Vt) to assess ventilation. 12 patients who were proned twice or more were included. There was a significant improvement in P/F ratio when prone (110.18 ± 28.11) compared to supine (88.95 ± 19.34) (p < 0.01). There was no improvement in Vd/Vt on proning (p > 0.05). Vd/Vt as a function of time displayed a positive linear correlation in those who did not survive (n = 9) (Rs = 0.48, p < 0.01) but no observed correlation in those who survived (n = 3) (Rs = 0.002, p = 0.97). Our findings indicate that prone position in patients with Covid-19 has little effect on dead space fraction but does improve oxygenation. Rise in dead space with time appears to be a prognostic factor for death in patients with severe Covid- 19.
Introduction
Prone positioning has shown to have significant survival benefits in ARDS. 1 Therefore, this therapy has become standard practice in severe respiratory failure during Covid-19 pandemic. However, there is little evidence in the literature assessing its effect on patients with Covid-19. 2 With this in mind, we have performed a retrospective study of patients receiving treatment with prone-position in the context of Covid-19, and have assessed its impact on efficiency of ventilation (dead space ratio), oxygenation (P/F ratio) and mortality.
Methods
We included all patients admitted to our 18 bed ICU with either PCR-confirmed or clinically presumed diagnosis of Covid-19 pneumonia, who were under mechanical ventilation and completed two or more full proning cycles in the period 12/03/2020 – 20/04/2020. The study was approved by the trust Caldicott Guardian.
Demographic characteristics, data on mechanical ventilation, patient position, end tidal CO2 (EtCO2) and arterial blood gas were obtained from patient charts. P/F ratios were calculated as a measure of the severity of hypoxemia and Vd/Vt fraction (using the Enghoff modification of the Bohr equation) 3 as an indicator of ventilation efficiency. Data analysis was performed using SPSS software.
Results
Twelve patients were studied, presented in Table 1. There was a statistically significant improvement in average P/F ratio when prone compared to supine (Wilcoxon signed-rank, Z = 12, p < 0.01) with more than a 20% increase. There was no statistically significant change in average Vd/Vt ratio on proning (p > 0.05). Over time, Vd/Vt increased in non-survivors (Spearman Rank Correlation Coefficient, Rs = 0.48, p < 0.01), whilst measurements remain unchanged in survivors (Rs = 0.002, p = 0.97) Figure 1.
Patient demographics, average VD/VT and P/F values across supine and prone and proning cycles (PCs).
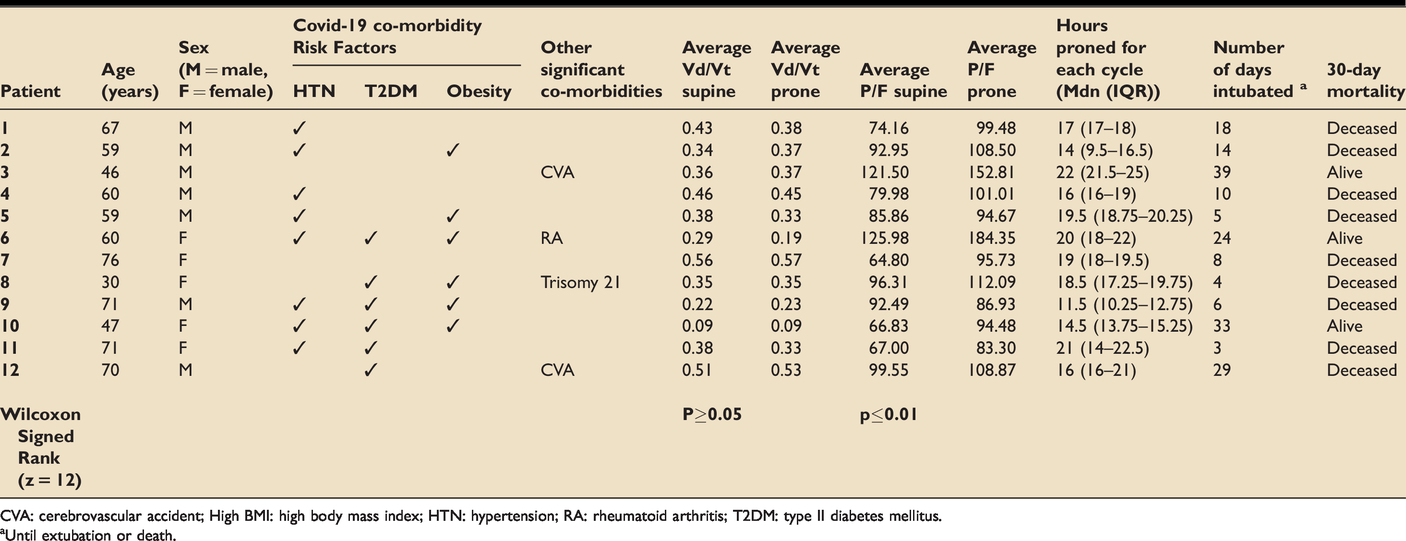
CVA: cerebrovascular accident; High BMI: high body mass index; HTN: hypertension; RA: rheumatoid arthritis; T2DM: type II diabetes mellitus.
aUntil extubation or death.
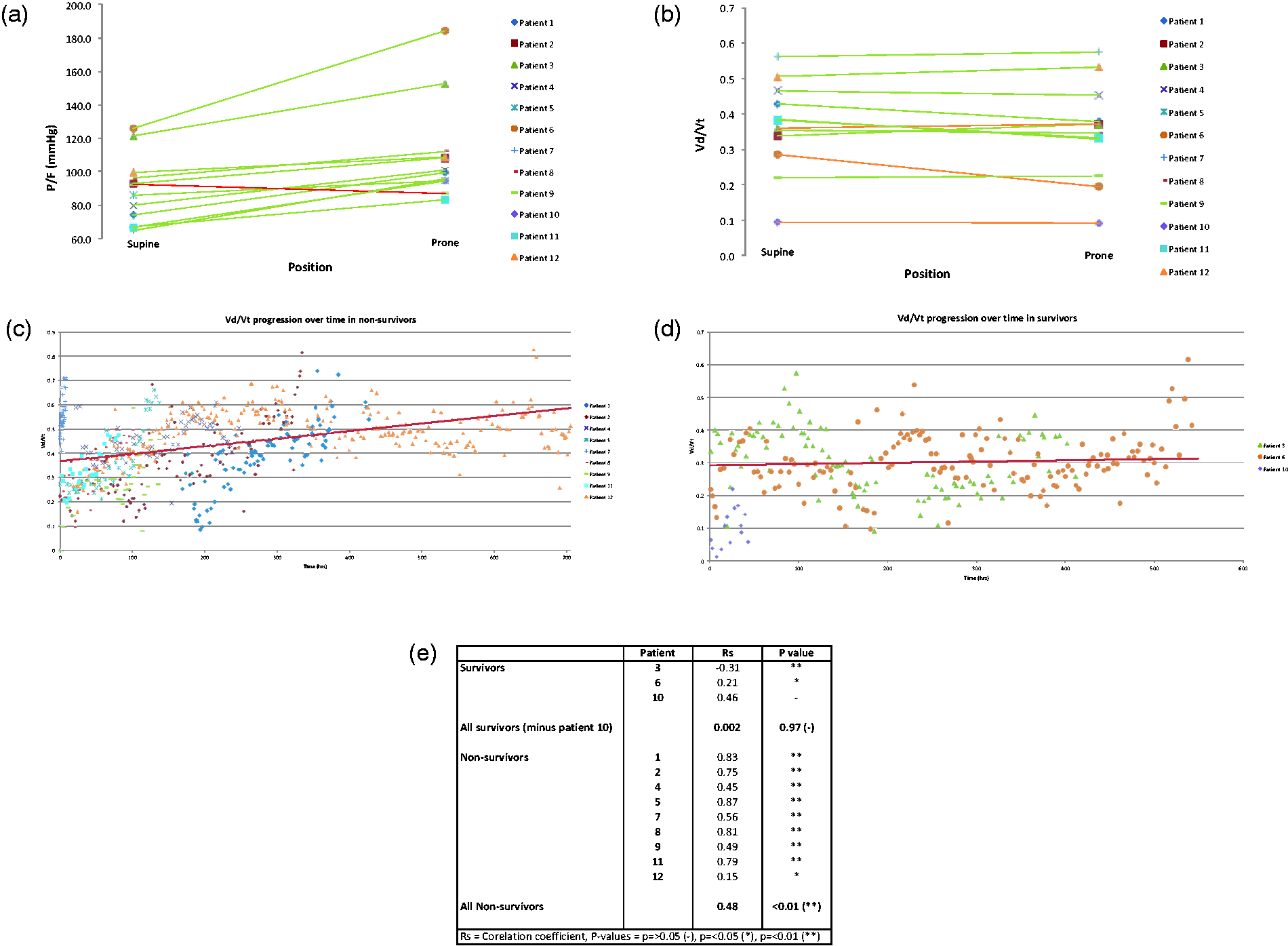
(a) P/F ratio (mmHg) Supine vs Prone for all patients. (a) P/F ratio (mmHg) Supine vs Prone for all patient. (b) Vd/Vt fraction Supine vs Prone for all patients. (c) Vd/Vt against time in non-survivors with linear trend line spotted for all patients. (d) Vd/Vt against time in survivors with linear trend line plotted for patients 3 & 6. (e) Correlation between Vd/Vt and time (hours) in survivors and non-survivors.
Discussion
Our findings indicate that prone position in patients with Covid-19 has little effect on dead space fraction, but does improve P/F ratio. Proning did not appear to have any effect on dead space fraction during disease progression. This poses the question as to whether this therapy adds anything to the management of Covid-19 patients - aside from a transient improvement in oxygenation that would buy time for additional therapies to succeed. In non-survivors, we also observed a progressive rise in Vd/Vt over time. This was not the case in survivors.
In ARDS, a raised dead space fraction has been shown to be a prognostic marker for death 4 , and when considering response to prone position as a therapy, improvements in dead space ratio (but not oxygenation) have been shown to be prognostic for survival. 5 Our findings seem to replicate this in patients with Covid-19. We propose the regular calculation of Vd/Vt as an easy tool to assess the progress of Covid-19 patients.
The observed improvement in oxygenation upon proning is most likely, and in similarity to ARDS, due to a decrease in shunt causing an improvement in V/Q mismatch. However, the mechanism by which this happens appears to be in contrast to that of classic ARDS physiology where the improvement in shunt is via an optimization of lung recruitment. 6 There is poor recruitability in a significant subset of Covid-19 patients7,8 and thus we suggest improvements in shunt are through alternate mechanisms.
We hypothesize that prone position in Covid-19 patients improves oxygenation through a strictly mechanical blood flow pattern, but with no impact in lung parenchyma and recruitability. It has been proposed that the severe hypoxaemia observed in such patients is also contributed to by the loss of hypoxic pulmonary vasoconstriction leading to high levels of shunt,9,10 unrelated to parenchymal changes. Our data appears to support this hypothesis.
Drawing firm conclusions from this data is not possible. Firstly, this is a retrospective study. Secondly, proning was used mostly as a rescue measure, rather than directed by any standard protocol. Thirdly, we were forced to transfer many patients due to bed pressures during the surge. This may have biased our selection towards the sickest patients who weren't fit for transfer. However, given our cohort contains some of the sickest Covid-19 patients, we believe this data to be of value. Further work is required to replicate our findings on a larger scale.
Conclusions
In summary, our data suggest patients with severe Covid-19 pneumonia may not behave like classic ARDS. Their response to prone positioning has been limited to an improvement in oxygenation, with no impact on dead space. This raises questions regarding the usefulness of prone position in Covid-19 patients beyond a temporary measure for oxygenation. Over time, deterioration of dead space has been observed in non-survivors. Hence, we propose the use of dead space fraction as a potential bedside marker for prognosis and progression of the disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.